

Abstract
Pyogenic granuloma is one of the inflammatory hyperplasias seen in the oral cavity. This term is a misnomer because the lesion is unrelated to infection and in reality arises in response to various stimuli such as low-grade local irritation, traumatic injury, or hormonal factors. It predominantly occurs in the second decade of life in young females, possibly because of the vascular effects of female hormones. Clinically, oral pyogenic granuloma is a smooth or lobulated exophytic lesion manifesting as small, red erythematous growth on a pedunculated or sometimes sessile base, which is usually hemorrhagic. Although excisional surgery is the treatment of choice , some other treatment protocols such as the use of Nd:YAG laser, flash lamp pulsed dye laser, cryosurgery, intralesional injection of ethanol or corticosteroids, and sodium tetradecyl sulfate sclerotherapy have been proposed. We present the case of a 25–year-old pregnant woman with large oral pyogenic granuloma.
Keywords: Inflammatory hyperplasia, oral cavity, pregnancy, pyogenic granuloma
Introduction
Pyogenic granuloma (PG) is a localized granulation tissue of the oral cavity or skin that is considered to be non-neoplastic in nature. The first report of PG in English literature was described by Hullihen in 1844, but the term “pyogenic granuloma” or “granuloma pyogenicum"” was introduced by Hartzell in 1904. Although it is a common disease in the skin, extremely rare in the gastrointestinal tract, except for the oral cavity where it is often found on keratinized tissue. There are two kinds of PG histologically, lobular capillary hemangioma (LCH type), and non-LCH type.
Case Report
A 25-year-old pregnant woman in third trimester reported a growth in the mouth involving lower left posterior region, which bled frequently and interfered with eating. Intraoral examination revealed a large soft tissue mass in the lower left lingual vestibule approximately 3 × 7 cm in size. It had a smooth surface laterally and superiorly except for the region near the teeth where it showed occlusal indentations of upper teeth resulting in small ulcerations. The growth was pedunculated and attached to the marginal gingiva interproximally between 34 and 35, and extended on the buccal aspect covering the entire buccal and lingual surfaces of 34 and 35 [Figures 1 and 2]. IOPA radiograph of 34 and 35 revealed a slight amount of interdental alveolar crestal bone resorption, which may be suggestive of pressure effect [Figure 3].
Figure 1.

A large soft tissue mass in lingual vestibule
Figure 2.

Extension of the soft tissue mass from lingual vestibule to the buccal aspect of 34 and 35
Figure 3.
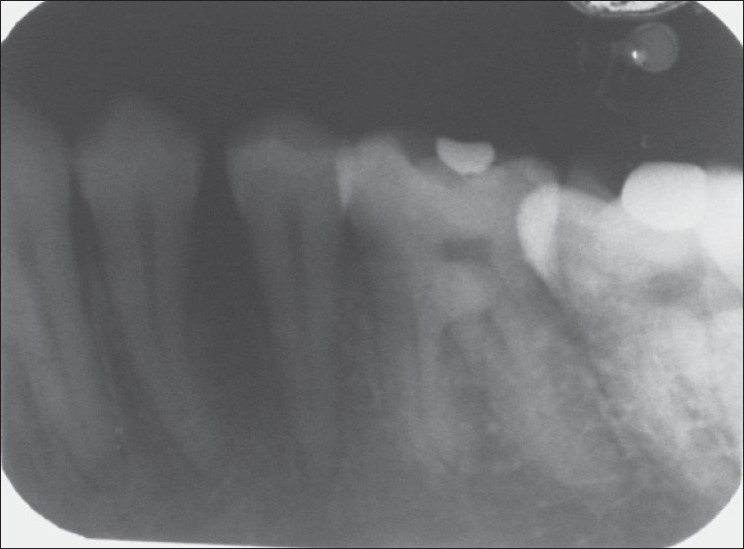
Intraoral periapical radiograph of 34 and 35 revealed interdental alveolar crestal bone resorption
The hemogram of the patient was within normal limits and excisional biopsy of the growth was carried out under local anesthesia. The excised specimen is shown in Figure 4. Photomicrograph of H and E-stained section shows ulcerated stratified squamous epithelium with an underlying fibrovascular stroma. The stroma shows large number of budding capillaries, plump fibroblasts and areas of extravasated blood and a dense chronic inflammatory cell infiltrate [Figure 5]. The patient's history, clinical, radiographical, and histopathological findings were suggestive of pregnancy tumor.
Figure 4.

Excised specimen
Figure 5.
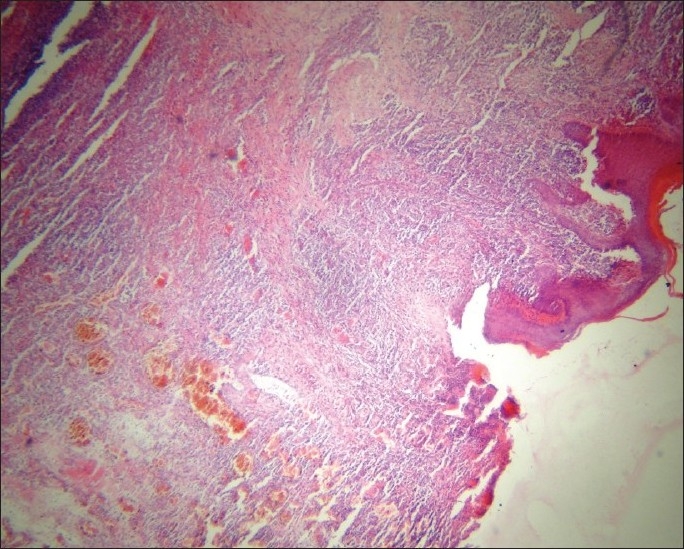
Photomicrograph of H and E stained section showing ulcerated stratified squamous epithelium with an underlying fibrovascular stroma including large number of budding capillaries, plump fibroblasts and a dense chronic inflammatory cell infiltrate
Discussion
PG of the gingiva develops in up to 5% of pregnancies, hence the terms “pregnancy tumor” and “granuloma gravidarum” are often used. The hormonal imbalance coincident with pregnancy heightens the organism's response to irritation,[1]; however, bacterial plaque and gingival inflammation are necessary for subclinical hormone alterations leading to gingivitis. Generally, it appears in the 2nd - 3rd trimester of pregnancy, with a tendency to bleed and a possible interference with mastication. Estrogen enhances vascular endothelial growth factor (VEGF) production in macrophages, an effect that is antagonized by androgens and which may be related to the development of pregnancy tumor. These regulatory effects of sex steroids may be manipulated as therapeutic or prophylactic measures in pregnancy tumor.[2] Progesterone functions as an immunosuppressant in the gingival tissues of pregnant women, preventing a rapid acute inflammatory reaction against plaque, but allowing an increased chronic tissue reaction, resulting clinically in an exaggerated appearance of inflammation.[3] Angiostatin was expressed significantly less in PG than in healthy gingiva and periodontally involved gingiva. The molecular mechanism for regression of pregnancy tumor after parturition remains unclear. It has been proposed that, in the absence of VEGF, Angiopoietin-2 (Ang-2) causes blood vessels to regress. The protein level of Ang-2 was highest in the pregnancy tumors, followed by those after parturition and normal gingiva. The amount of VEGF was high in the granulomas in pregnancy and almost undetectable after parturition.
Although conservative surgical excision and removal of causative irritants are the usual treatments,[1] the excision should extend down to the periosteum and the adjacent teeth should be thoroughly scaled to remove the source of continuing irritation.[4] The Nd:YAG laser is used nowadays because of the lower risk of bleeding compared to other surgical techniques.[5]
Surgical excision of a PG lesion after delivery seemed the best treatment option[6]. The majority of cases are symptomatic and show bleeding; nodules (71.9%) with soft consistency (62.3%) and a red surface (73.2%)[7]. Simple excision is enough to prevent recurrence but the aetiology and pathogenesis must be known to understand its nature[8]
Recently, the flash lamp pulsed dye laser, cryosurgery, sodium tetradecyl sulfate sclerotherapy were used. Particularly for highly recurrent lesions, intralesional injection of absolute ethanol, corticosteroids were successfully attempted. If uncontrolled bleeding occurs, management should be based on the individual condition and should range from supportive therapy such as desiccation of bleeders; local, firm compression to blood transfusion, as well as medication to accelerate fetal lung maturity or even termination of pregnancy to save the patient's life. Thus, during pregnancy, careful oral hygiene, removal of dental plaque and use of soft toothbrushes are very important to avoid occurrence of a pregnancy tumor.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Eversole LR. 3rd ed. Hamilton: BC Decker; 2002. Clinical outline of oral pathology: Diagnosis and treatment; pp. 113–4. [Google Scholar]
- 2.Kanda N, Watanabe S. Regulatory roles of sex hormones in cutaneous biology and immunology. J Dermatol Sci. 2005;38:1–7. doi: 10.1016/j.jdermsci.2004.10.011. [DOI] [PubMed] [Google Scholar]
- 3.Ojanotko-Harri AO, Harri MP, Hurttia HM, Sewon LA. Altered tissue metabolism of progesterone in pregnancy gingivitis and granuloma. J Clin Periodontol. 1991;18:262–6. doi: 10.1111/j.1600-051x.1991.tb00425.x. [DOI] [PubMed] [Google Scholar]
- 4.Neville BW, Damm DD, Allen CM, Bouquot JE. 2nd ed. Philadelphia: WB Saunders; 2002. Oral and maxillofacial pathology; pp. 437–95. [Google Scholar]
- 5.Powell JL, Bailey CL, Coopland AT, Otis CN, Frank JL, Meyer I. Nd: YAG laser excision of a giant gingival pyogenic granuloma of pregnancy. Lasers Surg Med. 1994;14:178–83. doi: 10.1002/1096-9101(1994)14:2<178::aid-lsm1900140211>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]
- 6.Lindenmuller IH, Noil P, Mameghani T, Walter C. CO2 laser-assisted treatment of a giant pyogenic granuloma of the gingival. Int J Dent Hyg. 2010;8(3):249–52. doi: 10.1111/j.1601-5037.2010.00449.x. [DOI] [PubMed] [Google Scholar]
- 7.Gordon-Nunez MA, de vasconcelos M, Benevenuto TG, Lopes MF, et al. Oral pyogenic granuloma: a retrospective analysis of 293 cases in a Brazilian population. J Oral Maxillofac Surg. 2010;68(9):2185–8. doi: 10.1016/j.joms.2009.07.070. [DOI] [PubMed] [Google Scholar]
- 8.Saravana GH. Oral pyogenic granuloma: a review of 137 cases. Br J Oral Maxillofac Surg. 2009;47(4):318–9. doi: 10.1016/j.bjoms.2009.01.002. [DOI] [PubMed] [Google Scholar]