
Figure 2.
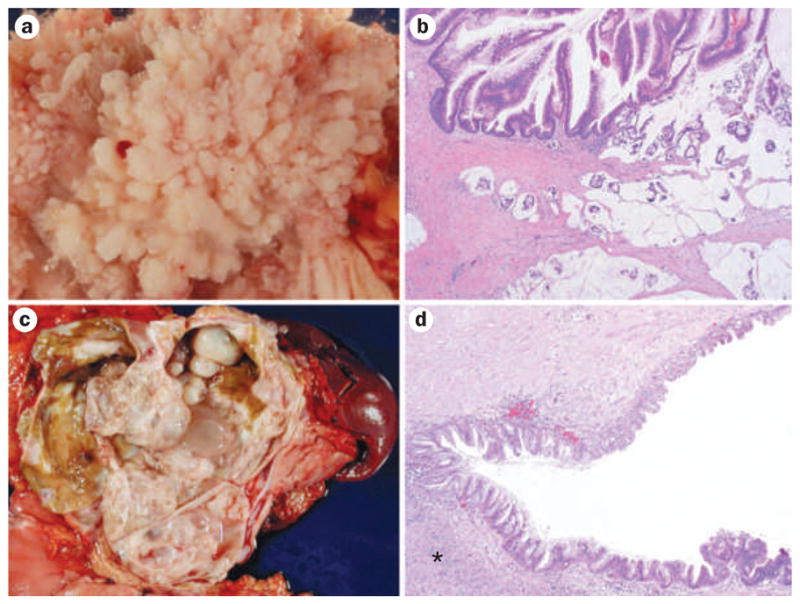
Cystic precursor lesions of pancreatic cancer. a | An extensive intraductal papillary growth of a large intraductal papillary mucinous neoplasm (IPMN) (image taken with specimen immersed in water). b | Histology displays finger-like papillae and high-grade dysplasia (upper part of image) with an invasive colloid adenocarinoma (lower part of image); these lesions are often located in the main pancreatic duct and show characteristic intestinal differentiation (hematoxylin and eosin staining, 20× original magnification). c | A large multicystic mucinous cystic neoplasm (MCN) in the pancreatic tail. d | A diagnostic sign for MCN ovarian-like stroma (indicated with an asterisk) underlies the neoplastic epithelium. The latter often shows abrupt transition in the degree of dysplasia; note the flat epithelium with mild cytoarchitectural atypia at the upper part of the image versus the more dysplastic and papillary growth pattern in the lower part of the image (hematoxylin and eosin staining, 40× original magnification).