

Abstract
Background:
Bone tumors remain a daunting challenge to orthopedic surgeons. The challenge is heightened in developing countries due to limited diagnostic and therapeutic facilities as well as due to ignorance. The published literature on this subject is sparse in our environment.
Objective:
To determine the pattern of bone tumors including their relative frequencies, age and sex distributions, anatomical sites of occurrence and clinico-pathological characteristics as seen in a tertiary care hospital of south India.
Materials and Methods:
This is a retrospective review of all the histologically confirmed bone tumors seen at JSS Medical College and Hospital, Mysore over an 8 year period: 2002 to 2009.
Results:
A total of 117 patients (aged 5 to 82 years) with a mean of age of 26.87 years were studied. Seventy-six patients (64.96%) were males and 41 (35.04%) were females. The peak age incidence for primary bone tumors was in the age group of 11-20 years and that for metastatic bone tumors was more than 60 years. Sixty-seven (57.26%) of the tumors were benign. Among these, osteochondroma was the most common, accounting for 26 cases (22.22%) followed by Giant cell tumor (24 cases, 20.51%). Osteosarcoma accounted for 35.14% (13 cases) of all the primary malignant tumors in the study. Lower end of femur was the most common site for primary bone tumors and accounted for 30 cases (25.64%) followed by upper end of tibia and fibula (24 cases, 20.51%). The most common site for metastatic bone tumors was upper end of femur including hip joint followed by spine.
Conclusion:
This study showed that primary bone tumors are mainly benign, occurred predominantly in the second decade of life with a male preponderance. Osteochondroma and osteosarcoma are the most common benign and primary malignant bone tumors, respectively. The most common primary foci for metastatic bone tumor are from the respiratory tract.
Keywords: Bone tumors, giant cell tumor, metastasis, osteosarcoma, osteochondroma
INTRODUCTION
In comparison to the myriad of other tumors, bone tumor is relatively uncommon, constituting only 0.5% of the total world cancer incidence.[1] Bone tumors remain a daunting challenge to the orthopedic surgeons and the pathologists. The challenge is heightened in developing countries due to limited diagnostic and therapeutic facilities as well as due to ignorance. The published literature on the subject is sparse in our environment. As already mentioned, bone cancer is not a common malignant disease, and perhaps for this reason its etiology is not very clear. Furthermore, very few studies have been conducted in this field. Among different types of primary bone cancer, Osteosarcoma constitutes the highest proportion (36%) of cases, followed by chondrosarcoma, osteoclastoma and Ewing's sarcoma. The clinicians and the pathologists handling management responsibility must have high index of suspicion as to the nature of bone lesion in order to establish the diagnosis of bone tumors.
The purpose of this study is to determine the pattern of bone tumors including their relative frequencies, age and sex distributions, anatomical sites of occurrence, and clinico-pathological characteristics as seen in a tertiary care hospital of south India.
MATERIALS AND METHODS
A retrospective review of the clinical and histo-pathological records of patients with established diagnosis of bone tumors at the JSS medical college and hospital, Mysore, was done covering the period between January 2002 and December 2009. The clinical data such as the age, sex, anatomical site, radiological and histo-pathological findings as well as the record of other investigations and management were extracted from the clinical case notes of patients. Where necessary when histo-pathological work up was required, new sections were prepared from the paraffin blocks and stained with routine hematoxylin and eosin stain. Bone tumors of odontogenic origin and infectious lesions were excluded from this study. A total of 117 neoplasms were observed from the all age groups; 104 of these neoplasms were primary bone tumors, others being secondary in origin.
The classification was based on the current World Health Organization (WHO)[2] histological classification of bone tumors. The data were analyzed manually using frequency distribution and percentages.
RESULTS
The types, age, and sex distribution, and sites of bone lesions encountered, with their relative frequencies are summarized in [Tables 1 and 2]. A total of 117 patients (aged 5 to 82 years) with a mean age of 26.87 years were studied. Seventy-six patients (64.96%) were males and 41 (35.04%) were females.
Table 1.
Histological types and age range distribution of bone tumors
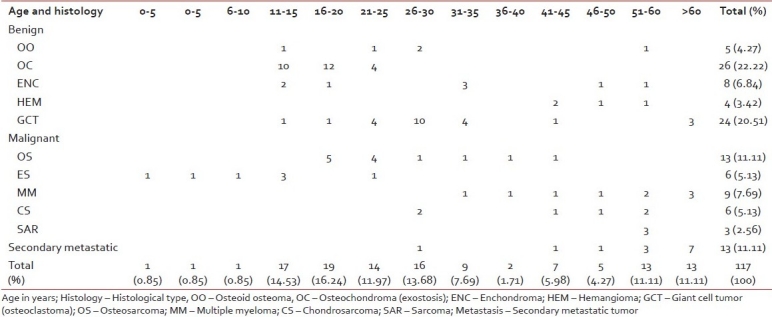
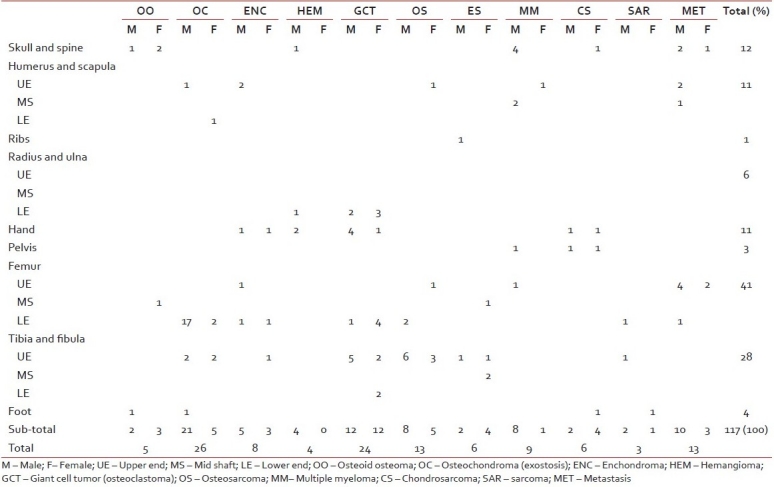
Table 2.
Anatomical sites and sex distribution of bone tumors
Sixty-seven (57.26%) of the tumors were benign. Among these, osteochondroma was the most common, accounting for 26 cases (22.22%) followed by Giant cell tumor (24 cases, 20.51%). Other benign tumors observed were enchondroma 6.84%, osteoid osteoma 4.27%, and hemangioma 3.42%. Osteosarcoma accounted for 11.11% (13 cases) of primary malignant tumors (37 cases, 31.62%) in this study. Others were Ewing's sarcoma (5.13%), chondrosarcoma (5.13%), multiple myeloma (7.69%), and sarcoma (2.56%).
The peak age incidence for primary tumors was in the age group of 11-20 years (30.77%). The lowest relative frequency of tumor occurrence was in the 0–10 years range (three cases) and all of them were Ewing's sarcoma. Lower end of femur being the most common site for primary bone tumors, accounted for 30 cases (25.64%) followed by upper end of tibia and fibula (24 cases, 20.51%).
Osteochondroma accounted for 22.22% of all the tumors, which made it the most common benign tumor. The male to female ratio was 4.2:1. Twenty-three of these occurred in the long bones of femur and 22 in tibia in the age range of 11-20 years.
Giant cell tumors accounted for 20.51% of all the tumors, which made it second most common benign tumor. The male to female ratio is 1:1. Five cases were observed at the distal end of femur, seven cases at the proximal end of tibia, five cases at the lower end of forearm, and five in the small bones of the hand. A majority of the cases were seen between 21 and 35 years (75 %), whereas three were seen over 60 years of age.
Osteosarcoma accounted for 11.11% of all the tumors and was found to be most common primary malignant bone tumor. The male to female ratio was 1.6:1. Nine cases were observed at the proximal end of tibia, two cases at the distal end of femur, one at the proximal end of femur, one case at the proximal end of humerus and nine were in the age range of 16-25 years. Eleven patients had conventional intramedullary osteosarcoma, while one had telangiectatic and one had giant cell variant.
Multiple myeloma accounted for 7.69% of all the tumors with a male to female ratio 8:1. Most of the myeloma cases had multiple sites involvement with predilection to the axial skeleton including skull and spine.
We had 13 cases of the metastatic bone tumors in our study with a men to women ratio 3.3:1; a majority of the cases were of more than 50 years of age (76.92%). The sites for the primary tumors were lung cancer (38.46%), prostate cancer (7.69%), breast cancer (7.69%), liver cancer (7.69%), gastrointestinal cancer (23.07%), and unknown cancers (15.38%). The common metastatic sites were femur with pelvis (53.85%), spine (23.07%), and humerus with ribs (23.07%).Of all the cases in the radiographic patterns, osteolytic types accounted for 76.92%, followed by osteosclerotic and mixed types.
The age and anatomical site distribution of other tumors are mentioned in [Tables 1 and 2].
DISCUSSION
In the present study, a significant proportion of neoplastic bone lesions were seen to occur in children constituting 33.33%. This finding is similar to reports by Omololu et al.,[3] and Mohammed et al.[4] in their studies of bone tumors in all age groups.
Osteochondroma was the most common benign bone tumor accounting for 20-40% of all the benign tumors. In a study by Mohammed et al[1] and Senac et al.,[5] osteochondroma was the most common lesion, occurring in 22.5 and 22.3% of children, respectively. Long bones of femur, tibia, and humerus were found to be the principal bones affected. These findings are similar to our institutional study.
In our study, giant cell tumor accounted for 20.51% of all cases. These findings draw parallel results to our literature. It was also noted that its incidence before the fusion of epiphysis was not common. The most common bones involved were the long bones; less commonly the jaws, vertebrae, scapula pelvis, and small bones of hands and feet were involved.[6–9]
The other less common benign tumors were enchondroma and osteoid osteoma, eight and five cases, respectively. Both of these tumors occur in patients with a wide age range spanning from 11 to 60 years. One classical case of osteoma was observed in femur and two classical cases of enchondroma occurred in the hand bones. We have observed a wider anatomical distribution of Osteoid osteoma in our study, which can be co-related to literature reports.[7–9]
Osteosarcoma is the most common primary bone tumor in young and adolescents. It occurs most frequently in the second decade, occurring in the metaphysis, mostly in lower end of femur followed by upper end of tibia.[7–10] In the present study, we observed a similar finding except that we have seen more cases in upper end of tibia.
Ewing sarcoma is a highly malignant, undifferentiated, peripheral primitive neuro-ectodermal tumor occurring most commonly at the diaphysis of long bones, in the 0-20 years age group, with male predominance.[7–9] Our study has matched with the available literature except for the female predominance with a male to female ratio 2:1.
Chondrosarcoma is the most common primary malignant bone tumor in the age group of 40-60 years. It commonly involves pelvis, femur, ribs, shoulder girdle, and vertebra with male predilection.[7–9] Among the six cases in our study, three cases had their usual anatomical site involvement, whereas three cases had hand and foot bones affected with female predominance, male to female ratio 2:1.
Multiple myeloma is the most common primary malignant bone tumor occurring most commonly in sixth and seventh decade of life with multiple site involvement.[7–10] We also observed that most of the myeloma cases had multiple sites involvement with predilection to the central skeleton including skull and spine with male to female ratio of 8:1.
Metastatic bone tumors most frequently occur in patients older than 50 years and commonly originate from lung, gastrointestinal system, prostate, breast, and liver. Femur, pelvis, vertebrae, humerus, and rib are the most common sites of metastases.[7–10] The clinical manifestation is extensive and nonspecific. Most lesions present with osteolytic patterns. Metastases with an unknown origin account for 15.38%. These observations are similar to the findings of Xu et al.[11] In spite of complexity, the clinical features should be mastered for early diagnosis and treatment.
In conclusion, this study showed that primary bone tumors were mainly benign, occurred predominantly in the second decade of life with a male preponderance. Osteochondroma and osteosarcoma were the most common benign and primary malignant bone tumors, respectively. The most common primary foci for metastatic bone tumor were from the respiratory tract.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared.
REFERENCES
- 1.Mohammed A, Sani MA, Hezekiah IA, Enoch AA. Primary bone tumours and tumour-like lesions in children in Zaria, Nigeria. Afr J Paediatr Surg. 2010;7:16–8. doi: 10.4103/0189-6725.59353. [DOI] [PubMed] [Google Scholar]
- 2.Fletches CD, Unni KK, Mertens F, editors. Lyon: ARC Press; 2002. World Health Organisation Classification of Tumors. Pathology and Genetics of Tumours of Soft Tissue and Bone. [Google Scholar]
- 3.Omololu AB, Ogunbiyi JO, Ogunlade SO, Alonge TO, Adebisi A, Akang EE. Primary malignant bone tumours in Ibadan. West Afr J Med. 2002;21:201–3. doi: 10.4314/wajm.v21i4.28001. [DOI] [PubMed] [Google Scholar]
- 4.Mohammed A, Isa HA. Patterns of primary tumours and tumour like lesions of bone in Zaria.Northern Nigeria: A review of 127 cases. West Afr J med. 2007;26:37–41. doi: 10.4314/wajm.v26i1.28301. [DOI] [PubMed] [Google Scholar]
- 5.Senac MO, Jr, Isaacs H, Gwinn JL. Primary Lesions of bone in 1st decade of life: Retrospective survey of biopsy result. Radiology. 1986;160:491–5. doi: 10.1148/radiology.160.2.3487812. [DOI] [PubMed] [Google Scholar]
- 6.Rai KM, Venkateswarlu S. Osteoclastoma. Indian J Radiol Imaging. 2008;18:4–11. [Google Scholar]
- 7.Bone RJ. Ackerman's Surgical Pathology. In: Rosai J, editor. St. Louis: Mosby; 1996. pp. 1917–2020. [Google Scholar]
- 8.Aston W, Briggs T, Solomon L. Tumors. In: Solomon L, Warwick D, Nayagam S, editors. Apley's System of Orthopaedics and Fractures. 9th ed. London: Hodder Arnold Hodder education; 2010. pp. 187–224. [Google Scholar]
- 9.Rosenberg AE. Bones, joints and soft tissue tumors. In: Kumar V, Abbas AK, Fausto N, Aster JC, editors. Robbins and cotran; Pathologic Basis of disease. 8th ed. Gurgaon: Elsevier Reed Elsevier India private limited; 2010. pp. 1205–56. [Google Scholar]
- 10.Bahebeck J, Atangana R, Eyenga V, Pisoh A, Sando Z, Hoffmeyer P. Bone tumours in Cameroon: Incidence, demography and histopathology. Int Orthop. 2003;27:315–7. doi: 10.1007/s00264-003-0480-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Xu DL, Zhang XT, Wang GH, Li FB, Hu JY. Clinical features of pathologically confirmed metastatic bone tumors--a report of 390 cases.[Article in Chinese] Ai Zheng. 2005;11:1404–7. [PubMed] [Google Scholar]