
Figure 1.
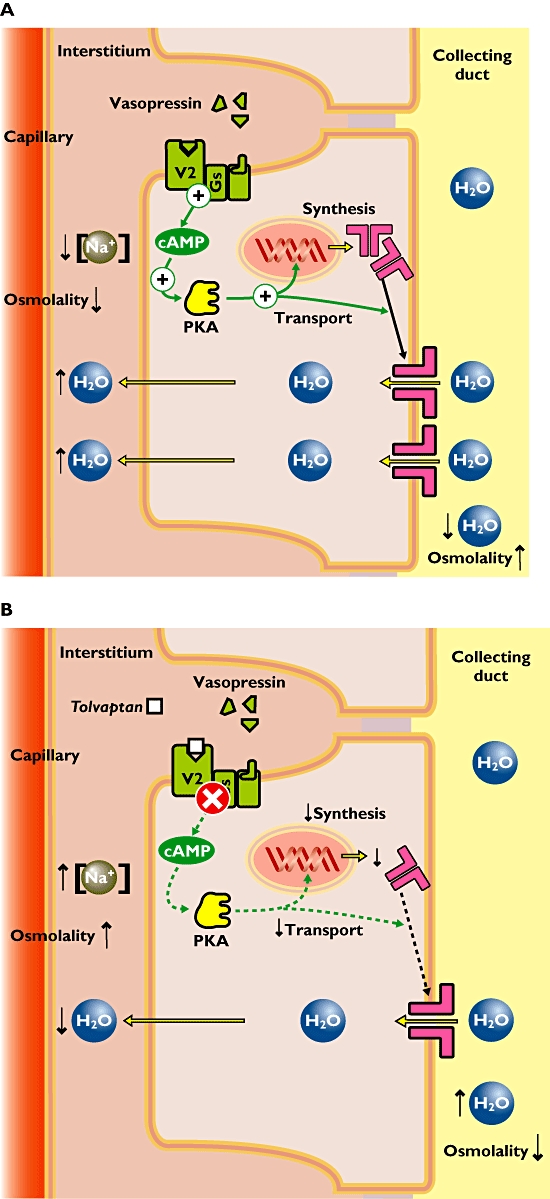
(A) Pathophysiology of hyponatremia. Increased concentrations of vasopressin (or antidiuretic hormone) evoke high activity of the vasopressin-2 (V2) receptors in the kidney. The signal transduction involves activation of the adenylate cyclase (not shown), increased cAMP and activation of protein kinase A (PKA). This results in enhanced expression of aquaporin channels and their transport towards the membrane. These channels transport water molecules from the collecting duct back into the circulation achieving both decreased plasma osmolality and decreased urine production. (B) Mechanism of action of tolvaptan in hyponatremia. The V2 receptor antagonist tolvaptan blocks the vasopressin effect in the kidney. This results in decreased expression of aquaporin channels and lower amounts of aquaporin channels in the apical membrane. Fewer water molecules are retained and more water is excreted in the urine. Eventually the plasma osmolality increases and normal plasma sodium concentrations are achieved