

Abstract
We use data from the Whitehall II Study to examine the joint evolution of health status and economic status over the life course. We study the links between health and socioeconomic status in childhood and health and employment status at older ages. We find early life socioeconomic status is significantly associated with health over the life course, even though selection into Whitehall mutes the effects of childhood. In addition, we find that current position in the civil service is not associated with future self-assessed health, but current self-assessed health is significantly associated with promotion in the civil service.
That early-life health and environment can have life-long effects on cognitive function, health and wellbeing has been documented by researchers from many disciplines, using data from many countries collected over the last century. In a series of papers, David Barker and colleagues underscore the importance of nutrition in utero for health at older ages, reporting that early-life deprivation is associated with the onset of a number of chronic conditions in late-middle age, including coronary heart disease and diabetes.1 They argue that different physical systems and organs may not be able to recover fully from lack of adequate nutrition at critical periods in fetal life and infancy.
Recent research has also highlighted the associations between infant and childhood health and cognitive function, and between cognitive function in childhood and choice of occupation and earnings in adulthood. (Currie 2009 provides an excellent survey.). In work related to our analysis here, Case and Paxson (2008a) document that, in the United Kingdom, every inch of height is associated on average with a 1.5 to 2% increase in earnings for both men and women, and that this labour market height premium can be explained by the higher cognitive test scores taller adults attained as children. Case and Paxson hypothesize that early life environment – nutrition and health in utero and childhood – affects children’s ability to reach both their physical (height) potential and their cognitive potential.
Height, as a marker for health and nutrition in childhood, has been shown to be highly correlated with many outcomes of interest, including later-life cognitive function, health, and depression in the US Health and Retirement Study (Case and Paxson, 2008b); earnings among adults of all ages in the British Household Panel Survey (Case, Paxson and Islam, 2009); and reports of life satisfaction and wellbeing in the US Gallup-Healthways Well-Being Index (Deaton and Arora, 2009).
Some social epidemiologists, while recognizing that early-life health and circumstance may play a role in later-life outcomes, argue that their effects are dwarfed by the impact of adult socioeconomic status on adult health. In a series of influential papers, Michael Marmot and colleagues use longitudinal data collected on a cohort of British civil servants to argue that the impact of social position on changes in health status (the social causation of health) is more important, measured using a number of metrics, than is the impact of health on social position (the health selection hypothesis). (See, for example, discussion in Chandola et al. 2003.) In their analysis of the relative importance of childhood and adult circumstance in predicting cardiovascular disease among civil servants, the Whitehall II team concludes that “whatever the salient features of the adult socioeconomic environment may be, it seems they are equally or more important than circumstances in childhood” in determining cardiovascular risk in British civil servants (Brunner et al. 1999, p. 762). Early life is important, these researchers argue, because “childhood circumstances determine adult circumstances and these, in turn, affect disease risk” (Marmot et al. 2001, p. 305).
For many analyses, the Whitehall II Study of British civil servants is well designed. All individuals in the study work for the same employer; they all have access to Britain’s National Health Service; and, at the beginning of the study period, they were all employed in London. Marmot and colleagues appeal to the relative homogeneity of their sample to suggest that differences in health outcomes between civil servants cannot be due to differences in access to (or quality of) medical care. Instead, they argue, differences in health outcomes between civil servants of higher and lower rank are due primarily to working conditions: seniority in the employment hierarchy predicts longer life, and “high demands and low control at work” predict poor health.2 The contribution of the Whitehall II study in documenting the links between adult health status and social status has been large indeed.
In this paper, using data from the Whitehall II study, we concentrate on the potential role played by early-life health and socioeconomic status as determinants of cohort members’ health and employment status at Whitehall. We find that, because the population from which this cohort was drawn consisted almost exclusively of white collar civil servants,3 the Whitehall II sample will in general provide inconsistent estimates of the association between childhood conditions and adult outcomes for the population as a whole. In a standard model of selection, under assumptions we make precise below, the observed associations between childhood characteristics and adult health will be biased downward in absolute value in the Whitehall II sample: children from poor backgrounds who find white collar positions must have systematically stronger unobservable attributes than do other poor children. Comparing our findings for Whitehall with those from two nationally representative data sets in which we can mimic selection into white collar positions, we find evidence consistent with a downward bias in coefficient estimates for Whitehall.
Even with such a bias, we find Whitehall cohort members’ early life health and circumstances are significantly associated with entry grade and promotion to higher grade in Whitehall. In addition, childhood circumstances are significantly associated with health status in middle age and older age.
Entry grade and current occupational grade at Whitehall are significantly related to self-assessed health in later years of the Study. However, their significance is eliminated by the addition of controls for members’ future occupational grades, suggesting that occupational grade may be more of a marker of poorer health than a cause of poorer health. We examine this further by estimating fixed effect first-difference models of self-assessed health status and occupational grade, where we quantify the extent to which change in health status predicts change in civil service grade, and the extent to which change in civil service grade predicts change in health status. We find no association between current civil service grade and future self-assessed health. In contrast, we find a significant association between current self-assessed health and future civil service grade. These findings support the health selection hypothesis, and do not support the hypothesis that social position in adulthood influences changes in health status.
We begin with an introduction to the Whitehall II data and a comparison of the Whitehall II cohort to two nationally representative British birth cohorts – the National Child Development Study of 1958 (NCDS) and the British Cohort Study of 1970 (BCS). Section 3 presents estimates of the association between family background and own-health in childhood and placement at Whitehall, and promotion to higher grades. Section 4 investigates the association between civil service grade and family background on self-assessed health in later phases of Whitehall II, before turning to first difference estimates of the association between current civil service grade and future self-assessed health, and that between current health status and future civil service grade.
1. The Whitehall II Study
Since its inception in 1985, the Whitehall II Study has followed a cohort of British civil servants, 10308 men and women who, at the beginning of the study, were aged 35 to 55 and employed in 20 London-based white collar civil service departments. The Study currently allows researchers to request data from the first six waves (phases) of data collection on health, mental health, working conditions, and health-related behaviors. Phases 1 (1985-88), 3 (1991-94) and 5 (1997-99) had both a self-administered questionnaire and a medical examination, and phases 2 (1989-90), 4 (1995-96) and 6 (2001) had mail-in questionnaires. At different phases, cohort members were also asked retrospective questions about their childhoods. An introduction to these data, and a link to a comprehensive list of Whitehall II publications, is available at http://www.ucl.ac.uk/whitehallII. A description of the variables we use, and the phases from which they are drawn, is presented in Appendix Table 1.
Summary statistics about this cohort are presented in Table 1, together with information about the two birth cohorts we will use in comparison. The NCDS has followed all children born in England, Scotland and Wales in the week of March 3, 1958 from birth through to middle-age. In a similar fashion, the BCS has been following all individuals living in Great Britain born in the week of April 5, 1970.4
Table 1.
Summary statistics for Whitehall II, BCS and NCDS
| Whitehall II
|
BCS (1970)
|
NCDS (1958)
|
|
|---|---|---|---|
| European/Caucasian | 0.891 | 0.958 | 0.965 |
| Male | 0.669 | 0.520 | 0.517 |
| Registrar General Occupation Classification: | age 30 | age 42 | |
| Professional | -- | 0.063 | 0.053 |
| Managerial | -- | 0.347 | 0.376 |
| Skilled, non-manual | -- | 0.247 | 0.213 |
| Skilled, manual | -- | 0.207 | 0.202 |
| Semi-skilled | -- | 0.110 | 0.123 |
| Unskilled | -- | 0.028 | 0.033 |
| Civil Service Grade: | Phase 1 (mean age 44) | ||
| Administrative | 0.294 | -- | -- |
| Professional/Executive | 0.480 | -- | -- |
| Clerical/Office Support | 0.227 | -- | -- |
| Father’s social class: | |||
| Professional | 0.094 | 0.068 | 0.045 |
| Managerial | 0.305 | 0.229 | 0.130 |
| Skilled, non-manual | 0.155 | 0.086 | 0.097 |
| Skilled, manual | 0.332 | 0.456 | 0.509 |
| Semi-skilled | 0.073 | 0.122 | 0.121 |
| Unskilled | 0.042 | 0.038 | 0.098 |
| Height in cm (males) | 176.2 | 177.1 | 176.7 |
| Height in cm (females) | 161.9 | 162.9 | 162.9 |
| Self-assessed health, reported at | phases 3-6 (mean age 54) | age 30 | age 42 |
| Excellent (BCS,NCDS) or Excellent/Very Good (WII) | 0.491 | 0.319 | 0.182 |
| Childhood conditions: | |||
| Spent 4+ weeks in hospital | 0.133 | ||
| Family owned a car | 0.415 | ||
| Number observations (measured at) | 10308 (phase 1) | 11261 (age 30) | 11384 (age 42) |
Comparison between the Whitehall II cohort and the British birth cohorts is complicated by the fact that employment class in the Whitehall II study is categorized by civil service grade, which is based on salary, while employment class in the birth cohort studies is based on the British Registrar General’s occupation classifications. In describing the Whitehall II data, Marmot et al. (1991) write:
On the basis of salary the civil service identifies twelve non-industrial grades which, in order of decreasing salary, comprise seven “unified grades”, and senior executive officer (SEO), higher executive officer (HEO), executive officer (EO), clerical officer, and clerical assistant. Other professional and technical staff are assigned by the civil service to one of these grades on the basis of salary. For analysis, we have combined unified grades 1-6 into one group and the bottom two clerical grades into another, thus producing six categories. (p.1388)
The Whitehall II team then combines these six categories to create three grades, which they use in most of their analyses: unified grades 1-6 and unified grade 7 define the (highest) “Administrative” grade; the SEO, HEO, and EO define the (second-highest) “Professional and Executive” grade; and the clerical category (which they note includes a small number of office-support staff) defines the “Clerical/Office Support” grade.
Although these civil service grades do not align with the British Registrar General’s occupation scale, it is clear that all but a handful of Whitehall II cohort members would be classified in the Registrar General’s top three occupational categories: professional occupations (Class I); managerial and lower professional occupations (Class II); and skilled non-manual occupations (Class III-N). (The example often used to characterize skilled non-manual occupations is “office workers.”) In belonging to one of the top three occupational classes, the Whitehall II cohort is different from the population at large. Approximately a third of NCDS and BCS cohort members, for example, report that they are employed in the lower three occupational classes (skilled manual (Class III-M), semi-skilled (Class IV) or unskilled (Class V)).
The distribution of fathers’ occupational status in the Whitehall II study is also significantly different from the distributions in the NCDS and BCS, despite the fact that fathers’ occupation status is defined the same way across the studies. There has been a shift toward higher status occupations in the United Kingdom, which can be seen in the difference in reports of fathers’ status between the 1958 and 1970 cohorts. Seventy three % of fathers were reported to be in the lowest three classes in the 1958 cohort – true for 62% of the 1970 cohort. However, in the Whitehall cohort, which contains individuals who are older than members of either of these birth cohorts, only 45% of fathers were reported in the lowest three classes. As the Whitehall II team notes, although the fathers of cohort members are disproportionately drawn from upper classes, there are still many fathers from lower status occupations (Marmot et al. 2001, p. 305). In Section 2 we argue that the absolute number of fathers from lower status occupations is less important than the fact that, in order to be selected for a position at Whitehall, cohort members whose fathers come from lower status occupations must have had higher draws on unobservable variables that influence occupational grade and health outcomes. We write down a standard selection model to highlight the effect of selection into Whitehall, and we use the British birth cohorts to investigate the empirical importance of the concentration of the Whitehall II cohort in the top three occupational grades.
2. Selection into Whitehall
To examine the effect of selection into Whitehall on coefficients estimated on childhood health and circumstance, we turn to a standard model of sample selection.5 Our interest is in the association between a vector of variables measuring childhood health and circumstance, x, and an outcome of interest in adulthood, y1. Such outcomes may include health status, measured using self-assessed health or adult height, or initial grade or promotion in the civil service. We assume a linear relationship between childhood characteristics and outcomes in adulthood:
| (1) |
We only observe individuals in the Whitehall II study if they were selected for the civil service. Let y2 be a binary indicator that an individual is a white collar Whitehall employee. Selection may depend on the same variables that determine outcomes of interest:
| (2) |
We make the following assumptions: (i) y1 is only observed when y2 is equal to 1; (ii) (u,ν) is independent of x with zero mean; (iii) ν ~Normal(0,1); and (iv) E(u ∣ ν) = γv, γ > 0.
With these assumptions, we can write
| (3) |
Using iterated expectations on equation (3) we find
Noting that in our sample y2 is equal to one, we can write
| (4) |
where λ(xδ) is the inverse Mills ratio: λ(xδ) = ϕ(·) / Φ(·). In our select sample, the expected change in an outcome of interest with change in right side variable xi can be written:
| (5) |
The second term in this derivative contains the derivative of the inverse Mills ratio with respect to its index (λ’(xδ)), which is negative throughout its range. If variables that appear in both (1) and (2) influence outcomes of interest (y1) and selection into Whitehall in the same direction (so that for a given xi, βi and δi are of the same sign), then OLS estimates in equation (1) will be biased downward in absolute value for the Whitehall II sample.6
With data from two nationally representative birth cohorts, we can test whether truncation by occupational status leads to significantly lower estimates of the relation between family background and outcomes of interest. Table 2 presents results of OLS regressions in which cohort members’ adult height is regressed on indicators for father’s occupational status, with the benchmark (omitted category) being that for unskilled work. For the NCDS and BCS cohorts, we control for whether cohort members were white, and male. For the Whitehall II cohort, we also control for age and age squared.
Table 2.
Height in adulthood and father’s social class
| BCS 70: Height at age 30 OLS Regression
|
NCDS 58: Height at age 33 OLS Regression
|
Whitehall II Mean height OLS Regression
|
|||
|---|---|---|---|---|---|
| All | Own grade is Prof, Managerial, Skilled non-manual | All | Own grade is Prof, Managerial, Skilled non-manual | Own grade is Administrative; Prof/Exec; Clerical | |
| Indicator: Father’s Class was | |||||
| Professional | 1.764*** (0.547) | 0.958 (0.803) | 3.286*** (0.401) | 3.145*** (0.543) | 2.056*** (0.456) |
| Managerial | 1.806*** (0.486) | 1.257* (0.757) | 2.370*** (0.305) | 1.789*** (0.449) | 1.799*** (0.405) |
| Skilled, non-manual | 1.460*** (0.533) | 0.948 (0.804) | 1.467*** (0.324) | 1.241*** (0.474) | 1.845*** (0.427) |
| Skilled, manual | −0.006 (0.472) | −0.571 (0.751) | 1.044*** (0.261) | 1.091*** (0.411) | 1.085*** (0.401) |
| Semi-skilled | 0.127 (0.515) | −0.012 (0.812) | 0.616** (0.312) | 0.230 (0.491) | 0.878* (0.473) |
| F-test (p-value) Sig of father classes | 21.45 (0.0000) | 11.39 (0.0000) | 23.98 (0.0000) | 10.59 (0.0000) | 8.27 (0.0000) |
| Chi-square test (p-value), equality of coefficients | 6.58 (0.2541) | 14.03 (0.0154) | |||
| Number obs | 7347 | 4040 | 9256 | 4528 | 6919 |
Notes. OLS regression coefficients reported, with standard errors presented in parentheses. All regressions include indicators for ethnicity and sex. Whitehall II regressions also include controls for age and age squared at phase 1. In all regressions, the benchmark for father’s social class is unskilled. The chi-square tests for equality of coefficients test the null hypothesis that the coefficients on the father’s class indicators are equal across columns 1 and 2 (BCS) and across columns 3 and 4 (NCDS).
The NCDS and BCS allow us to run regressions for the whole cohort, and for the cohort restricted to the three highest occupational classes, which are the classes to which almost all of the Whitehall II cohort belong. When we use the full samples, we find that cohort members with fathers whose positions were of higher status are taller in adulthood. Relative to cohort members whose fathers were unskilled in the BCS, members whose fathers were in the highest class are on average 1.8 centimeters taller (3.3 centimeters taller in the NCDS).
Turning to the subsample of birth cohort members working in the top three occupational classes, we find that the coefficients for father’s occupational grade are smaller than those for the cohort as a whole. When we restrict the BCS sample to cohort members who report that they work in the top three classes, we find that coefficients for father’s class become smaller and, for almost all grades, insignificantly different from zero. For the NCDS, when we use the restricted sample we find that the coefficients on the indicators for fathers’ social class are generally smaller than the coefficients obtained with the full sample. For both the BCS and the NCDS, we present chi-square tests of the hypothesis that the coefficients on the indicators of fathers’ social class are identical across the full and restricted samples. For the BCS, the hypothesis of equal coefficients cannot be rejected. This is not surprising, given the large standard errors that are obtained using the restricted sample. For the NCDS, the hypothesis that the coefficients are equal can be rejected. Consistent with equation (5) above, this suggests that selection on white collar status can have a significant effect on the estimated association between childhood SES and outcomes of interest.
Table 3 presents results for educational attainment in the NCDS birth cohort and the Whitehall II cohort. (Educational categories for the BCS cohort were quite different from the other two surveys, and so we restrict our attention in Table 3 to the NCDS and Whitehall II cohorts.) The NCDS asked cohort members in Stage 5 about their highest educational qualification at age 23. Whitehall II, in phase 5, asked cohort members about their level of academic qualification when they first left full-time education. The answers are scored in a similar fashion in the two surveys. In Whitehall II, these are ranked from “no qualification” (equal to 1), “school certificate” (2), matriculation (3), “O levels” (4) through to “masters degree or higher” (8). We run ordered probit regressions for the two cohorts, since these academic qualifications can be ordered, but the progression from one qualification to the next cannot be easily quantified.
Table 3.
Educational Attainment and Father’s Social Class
| NCDS 1958 cohort: Educational Qualification Ordered Probit
|
Whitehall II Educational Qualification Ordered Probit
|
||
|---|---|---|---|
| All | Own grade is Prof; Managerial; Skilled non-manual | Own grade is Administrative; Prof/Executive; Clerical | |
| Indicator: Father’s Class was | |||
| Professional | 1.649*** (0.062) | 1.363*** (0.089) | 1.224*** (0.101) |
| Managerial | 1.252*** (0.047) | 0.998*** (0.073) | 0.842*** (0.091) |
| Skilled, non-manual | 0.881*** (0.049) | 0.676*** (0.076) | 0.589*** (0.095) |
| Skilled, manual | 0.561*** (0.040) | 0.457*** (0.066) | 0.248*** (0.091) |
| Semi-skilled | 0.304*** (0.048) | 0.220*** (0.079) | 0.243** (0.105) |
| Chi-square test (p-value) Significance of father classes | 1366.90 (0.0000) | 443.58 (0.0000) | 439.48 (0.0000) |
| Chi-square test (p-value), equality of coefficients | 46.66 (0.0000 | ||
| Number obs | 10217 | 4450 | 4370 |
Notes. Ordered probit regression coefficients reported, with standard errors presented in parentheses. All regressions include indicators for ethnicity and sex. Whitehall II regressions also include controls for age and age squared at phase 1. The NCDS asked about the highest qualification a cohort member had obtained by age 23. The Whitehall II asked about the level of qualification when the individual first left full-time education. In all regressions, the benchmark for father’s social class is unskilled. The chi-square test for equality of coefficients tests the null hypothesis that the coefficients on the father’s class indicators are equal across columns 1 and 2.
For the full NCDS cohort, we find a highly significant set of coefficients for father’s social class, with a monotonic increase in cohort member’s educational attainment by father’s occupational status. Moving from the full NCDS cohort to the sub-sample in the top 3 classes leads to uniformly and significantly lower coefficients on father’s occupational status that are similar to those observed for the Whitehall II cohort. A chi-square test rejects the hypothesis that the coefficients in the unrestricted and restricted NCDS samples are identical. Again consistent with equation (5), this suggests that selection on white collar status can have a significant effect on the estimated association between childhood SES and outcomes of interest (here, educational attainment).
We can also test whether the associations between family background and outcomes of interest are the same for the Whitehall II cohort and the two nationally representative birth cohorts when the latter are restricted to their white collar members. To do so, we run regressions of height, self-assessed health, and educational qualifications on a linear measure of father’s occupational status, with higher status occupations given a higher number (6 = father was of professional status, 1= father was an unskilled labourer). The top panel of Table 4 presents results for the BCS and NCDS samples as a whole, and tests whether estimates of father’s status are significantly different for these cohorts than for the Whitehall II cohort. Height in adulthood and educational qualification are as discussed above. Self-assessed health in the Whitehall II study was asked using a five point scale (excellent, very good, good, fair and poor), while the birth cohort studies used four point scales (excellent, good, fair and poor). For Whitehall II, we combine “excellent” and “very good” and compare reports of health between the highest category and reports of “good, fair, or poor” health using an indicator variable.
Table 4.
Tests of equality between restricted BCS, NCDS and Whitehall II coefficients
| Height in centimeters | Self-assessed health Excellent or Excellent/Very Good | Educational Qualification | ||||||
|---|---|---|---|---|---|---|---|---|
| BCS (all) | NCDS (all) | W II (3civil service grades) | BCS (all) | NCDS (all) | W II (3civil service grades) | NCDS (all) | W II (3civil service grades) | |
| Father’s social class | 0.596*** (0.065) | 0.614*** (0.057) | 0.363*** (0.060) | 0.032*** (0.004) | 0.037*** (0.004) | 0.017*** (0.004) | 0.324*** (0.009) | 0.261*** (0.013) |
| Number obs | 7347 | 9256 | 6919 | 7370 | 9362 | 20528 | 10217 | 4370 |
| Test: coefficient BCS, NCDS = coeff WII (p-val) | 2.66 (0.008) | 3.03 (0.003) | -- | 2.65 (0.008) | 3.54 (0.000) | -- | 3.98 (0.000) | -- |
|
| ||||||||
| BCS (top 3 classes) | NCDS (top 3 classes) | W II (3civil service grades) | BCS (top 3 classes) | NCDS (top 3 classes) | W II (3civil service grades) | NCDS (top 3 classes) | W II (3civil service grades) | |
|
|
|
|
||||||
| Father’s social class | 0.510*** (0.084) | 0.531*** (0.077) | 0.363*** (0.060) | 0.022*** (0. 006) | 0.026*** (0.005) | 0.017*** (0.004) | 0.266*** (0.013) | 0.261*** (0.013) |
| Number obs | 4040 | 4528 | 6919 | 4048 | 5125 | 20258 | 4450 | 4370 |
| Test: coefficient BCS, NCDS = coeff WII (p-val) | 1.42 (0.155) | 1.72 (0.086) | -- | 0.69 (0.487) | 1.41 (0.159) | -- | 0.27 (0.789) | -- |
Notes. Height regressions and self-assessed health status regressions present OLS coefficients, with standard errors in parentheses. Educational attainment regressions present ordererd probit coefficients with standard errors in parenthesis. In all regressions, father’s social class is entered linearly (6=professional; 5=managerial; 4= skilled, non-manual; 3= skilled, manual; 2=semi-skilled; 1=unskilled). Self-assessed health is reported at age 30 in the BCS, age 42 in the NCDS, and is reported between phases 3 and 6 for the Whitehall II data. Whitehall II health is an indicator of “Excellent or very good health” on a five-point scale. NCDS and BCS health is an indicator of “Excellent” health on a 4-point scale. All regressions include indicators for ethnicity and sex. Whitehall II regressions also include controls for age and age squared. Whitehall II regressions for self-assessed health also include indicators for the phase in which the response was given, and cluster the standard errors by individual.
Consistent with the estimates presented in Tables 2 and 3 we find, for all three outcomes, that cohort members whose fathers were in higher status occupations report significantly better outcomes: cohort members whose fathers were of higher status are taller, they report better health, and their educational qualifications are higher.
For all three outcomes, we find in panel 1 that coefficients on father’s social class are significantly larger in the BCS and the NCDS than in the Whitehall II cohort. However, when we restrict the sample to BCS and NCDS cohort members in professional, managerial and skilled non-manual classes, we find no significant difference between coefficients on father’s status in the birth cohorts and in Whitehall II. We conclude from this that the selection into white collar positions in Whitehall diminishes the observed association childhood economic status and these adult outcomes.
The problem identified here – that analyses based on a select group may not provide unbiased information for the population as a whole – affects many more analyses than just those based on the Whitehall data. For example, Davey Smith et al. (1998) use longitudinal data on a sample of adults originally selected from 27 workplaces in the west of Scotland to examine the relative importance of education and adult occupational (social) class as determinants of mortality. To investigate this issue, they stratify their data on occupational status, and measure the strength of the relationships between education and mortality. They also stratify their data on education, and measure the strength of the relationships between occupational status and mortality. They observe “the … association between social class and all cause mortality remains strong within education strata, whereas within social class strata the relation between education and mortality is less clear” (p. 153). From this they conclude that although both education and social class are important determinants of morbidity and mortality, “occupational class is more strongly associated with overall … mortality than is the education measure” (p. 158). In turn, this evidence is cited by Singh-Manoux et al. (2004) that “research clearly shows adult measures of SEP [socioeconomic position] to be more powerful predictors of health than SEP measures from earlier in the life course” (p. 1073).
For reasons outlined above, because this analysis does not account for selection into occupational status, the estimated associations between education and health within social strata will be biased downward in absolute value, and the estimated associations between occupational status and health within education strata will be biased upward in absolute value. That is, for school leavers at age 16 (say), those who are stronger on dimensions not measured will be selected into higher classes and will be healthier, so that an analysis of the association between occupational class and health within an educational stratum will overestimate the association between class and health. Within an occupational class, for those with lower educational attainment to reach any given occupational stratum, they must have been strong in dimensions that are not measured in our data. This will lead to an underestimate of the association between education and health.
In summary, selection into Whitehall II provides an explanation for why researchers have found a weaker association between childhood circumstances and health outcomes in adulthood for this cohort than has been found in other cohorts. Marmot et al. (2001) recognize that the association between childhood socioeconomic status (SES) and adult morbidity is weaker in the Whitehall II Study than in some cohort studies. They suggest that this may be due to measurement error in the Whitehall II’s retrospective reports of childhood conditions (p. 305). Our comparisons between Whitehall II and the NCDS and BCS cohorts—in which childhood SES was measured at regular intervals from birth—suggest that selection into white collar occupations, rather than measurement error, may be the cause of the difference.
We turn next to examine the association between childhood background and economic wellbeing in adulthood, measured using initial occupational grade and promotion at Whitehall II.
3. The economic consequences of childhood health and circumstance
We investigate the extent to which family background is associated with cohort members’ first occupational grade in Whitehall, and promotion to a higher grade over time. Several elements of family background may be associated with initial grade assignment, including father’s social class; the cohort member’s report on whether his or her family owned a car when the member was less than 16; reports on whether the cohort member spent 4 or more weeks in the hospital when less than 16; and the member’s adult height. Together with father’s social class, car ownership gives us a window onto the cohort member’s socioeconomic status in childhood. Reports on hospitalisation tell us something about health in childhood, as does the member’s height.7
That height is associated with cohort members’ initial placement at Whitehall can be seen in Fig. 1, which presents non-parametric regression results of initial grade (1=clerical, 2=professional/executive, 3=administrative) regressed on height, separately for men and women. Women are more likely to start in a lower grade than are men, but throughout the distribution of women’s heights, we find a linear positive relationship between height and initial placement. For men, the relationship is positive up to heights of approximately 180 centimeters (the 75th percentile of height for men). The slopes for women and men (through 180 centimeters for men) are remarkably similar. We examine this association further in Table 5.
Fig. 1.

Height and first occupational grade at Whitehall
(Grade 1=Clerical, 2=Professional/Executive, 3=Administrative)
Table 5.
Placement and promotion at Whitehall
| Dependent variable: | ||||
|---|---|---|---|---|
| Entry | Promotion | Entry | Promotion | |
| without controls for education
|
with controls for education
|
|||
| Satisfied with health at phase 1 | -- | 0.036** (0.015) | -- | 0.032** (0.014) |
| Height (cm) | 0.005*** (0.001) | 0.005*** (0.001) | 0.004*** (0.001) | 0.005*** (0.001) |
| Father’s occupational class: | ||||
| Professional | 0.425*** (0.054) | 0.179*** (0.046) | 0.141*** (0.046) | 0.080* (0.044) |
| Managerial | 0.276*** (0.048) | 0.133*** (0.041) | 0.074* (0.041) | 0.057 (0.039) |
| Skilled, non-manual | 0.164*** (0.050) | 0.128*** (0.042) | 0.032 (0.043) | 0.065 (0.040) |
| Skilled, manual | 0.131*** (0.047) | 0.067* (0.040) | 0.059 (0.040) | 0.047 (0.038) |
| Semi-skilled | 0.074 (0.054) | 0.085* (0.046) | 0.007 (0.046) | 0.045 (0.044) |
| Family owned a car when <16 years old | 0.088*** (0.019) | 0.001 (0.016) | 0.052*** (0.016) | −0.005 (0.015) |
| Member spent 4+ weeks in hospital when <16 years old | −0.063** (0.026) | −0.047** (0.022) | −0.029 (0.022) | −0.037* (0.021) |
| F-test Father’s class variables (p-value) | 27.38 (0.000) | 5.95 (0.000) | 3.98 (0.001) | 0.80 (0.550) |
| F-test Family background variables (p-value) | 14.59 (0.000) | 2.37 (0.094) | 6.45 (0.002) | 1.65 (0.192) |
| F-test Educational qualification vars (p-value) | -- | -- | 150.73 (0.000) | 37.91 (0.000) |
| Number of observations | 3914 | 3746 | 3914 | 3746 |
Notes. OLS regression coefficients are presented, with standard errors in parentheses. A complete set of educational qualification indicators are included in columns 3 and 4. All regressions include indicators for ethnicity, sex, age and age squared at phase 1. Regressions for promotion also include an indicator for first grade at Whitehall. The sample for promotion is restricted to cohort members who enter in a grade lower than “administrative,” the highest grade.
Columns 1 and 3 of Table 5 present OLS regression results on the association between family and cohort member’s characteristics and initial placement at Whitehall. Column 1 reports results without educational qualifications included as controls. Results in column 3 include indicators of academic qualifications. Father’s occupational status is strongly correlated with a cohort member’s starting grade. Members whose fathers were in the highest occupational class were on average almost half an occupational grade (0.425) higher at entry than were cohort members whose fathers were unskilled labourers (the omitted occupational category). There is a monotonic relationship between father’s occupational class and starting grade. Jointly, these variables are significant (F-test= 27.4, p-value=0.000). Coming from a family that owned a car also predicts higher entry grade, while reporting that one spent more than 4 weeks in the hospital as a child predicts lower entry grade. These two background variables are also jointly significant (F-test=14.6, p-value=0.000).
Much of the association between family background and initial placement appears to work through educational attainment. Column 3 of Table 5 adds a complete set of indicators for highest academic qualification when first leaving full-time education. Jointly, these variables are highly significant in the initial placement regression (F-test=150.7, p-value=0.000), and their inclusion reduces the estimated association between entry grade and father’s occupational class, and between entry grade and other childhood variables. We know from Table 3 that father’s occupational class is highly correlated with a cohort member’s educational qualification. Spending time in the hospital as a child is negatively associated with educational attainment, while car ownership is positively associated with educational qualification. Even with controls for educational attainment, height continues to predict grade at entry.
We present the regression coefficients on our education qualification variables in Fig. 2. Additional qualifications strongly predict higher entry grade into Whitehall, with those entering with a Bachelor’s degree on average reporting more than 0.6 grades higher than those entering with no academic qualifications (the benchmark group), and those with a Master’s degree or PhD reporting more than 0.8 grades higher.
Fig. 2.
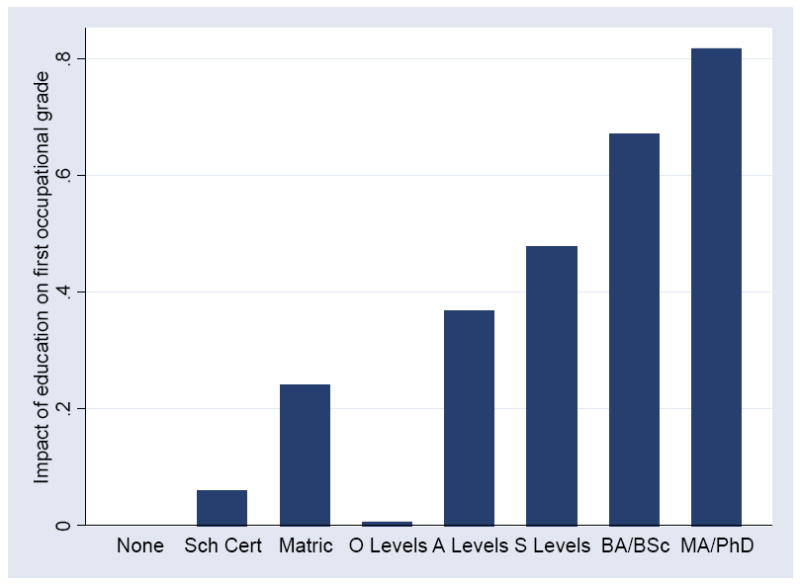
Education and first occupational grade
The second set of regressions in Table 5 investigates the relationship between reporting promotion to a higher grade at Whitehall, and family and individual characteristics. We define promotion as a member reporting a higher occupational grade the last time this member is observed than the grade he or she reported as their starting grade. Each cohort member appears once in these regressions, even if he or she had more than one promotion. Column 2 reports results without educational qualifications added as controls, and column 4 with indicators of academic qualifications included. We restrict the sample here to individuals who entered Whitehall at a grade lower than the top grade (it is rare for people to be demoted at Whitehall), and we control for starting grade (allowing a level difference in the probability of moving from a ‘clerical’ to a ‘professional’ grade from that of moving from a ‘professional’ to an ‘administrative’ grade).8
We also include a control for self-assessed health in phase 1 of the Study. Specifically, we include an indicator that the individual reports they were “moderately” or “very” satisfied with their health at phase 1 (true for two-thirds of respondents). These respondents are significantly more likely to report promotion. Three variables that are associated with health – self-assessment of health at the beginning of the Study, an individual’s height, and his or her report of having spent time in the hospital as a child – are all significantly associated with promotion at Whitehall. This is true with or without controls for educational attainment.
Fig. 3 examines whether height matters for promotion throughout the distribution, or is only important for especially short or especially tall cohort members. We find for both men and women, throughout the distribution of heights, an additional centimeter of height is associated with an increased probability of promotion. In the NCDS, BCS and Whitehall II studies, taller people report significantly better health than do shorter people. In the all three studies, taller people score significantly higher on cognitive tests (Case and Paxson 2008a, Case and Paxson 2010). The association between height and initial placement at Whitehall (Fig. 1) and between height and promotion (Fig. 3) may be due to the correlation between height and health, and between height and cognitive function.
Fig. 3.
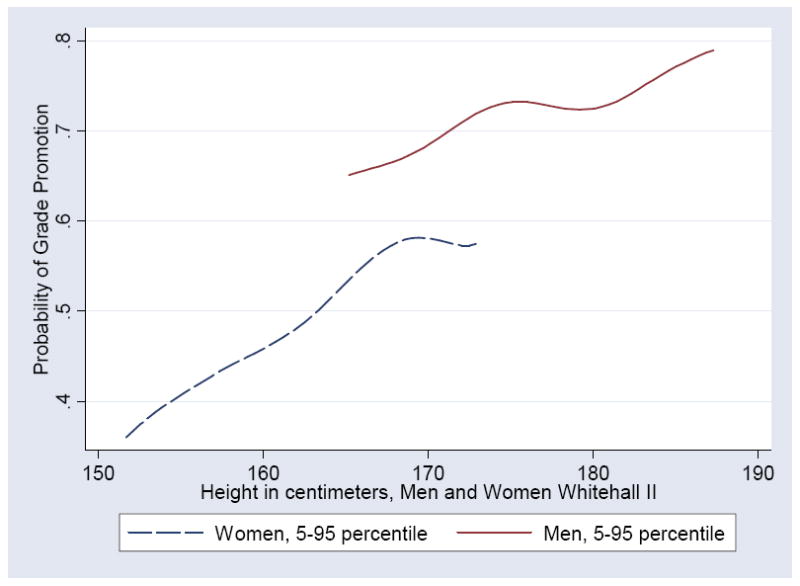
Height and the probability of reporting a grade promotion at Whitehall
Father’s occupational status is highly associated with grade promotion. This relation appears to work through cohort members’ educational attainment. The association between education and the probability of promotion is presented in Fig. 4, where regression coefficients are presented for educational qualifications relative to no academic qualification (the benchmark group). Members with a Bachelor’s degree are fifty % more likely to report a promotion than are those who lack educational qualifications. Those with a Master’s or PhD are nearly sixty % more likely to report promotion.
Fig. 4.
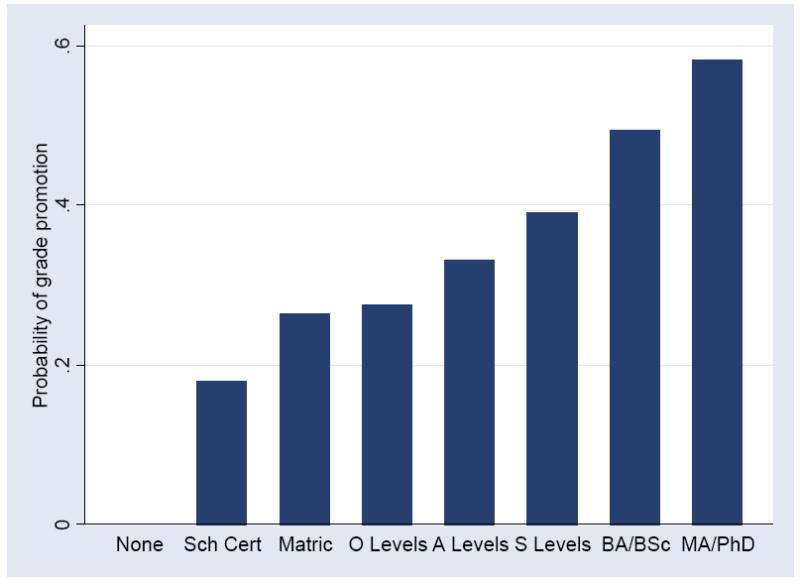
Education and promotion to a higher occupational grade
Results in Table 5 demonstrate that, even in this selected sample of white collar workers, childhood socioeconomic status, measured using father’s occupational status, and family car ownership during childhood, are strongly associated with entry grade and with promotion. Their effects appear to work through cohort members’ education, which is strongly associated with both initial grade and promotion. Results in Table 5 also demonstrate that childhood health, as measured using height and reports of hospitalisation before age 16, are also associated with entry grade and promotion in Whitehall. Part of the association between childhood health and entry grade appears to work through education. However, childhood health continues to be significantly related to promotion, even with controls for educational attainment, and for satisfaction with health at phase 1.9
In summary, in this selected sample of white collar workers, not only are poorer health and worse social circumstances in childhood associated with lower initial employment grade, but they are also associated with a widening in earnings gaps over time: those who were healthy in childhood, and those from higher SES backgrounds, are significantly more likely to be promoted. Because of the sample selection issues discussed above, it is likely that the associations would be even larger in a sample that is representative of the entire population.
4. Childhood circumstances and adult health
Cohort members were asked to assess their health in phase 3 (1991-1994), phase 4 (1995-1996), phase 5 (1997-1999) and phase 6 (2001). Specifically, they were to answer “in general would you say your health is … excellent, very good, good, fair or poor.” A poor self-report of health is a powerful predictor of mortality, even when controlling for physician assessed health status and health-related behaviors. Poor self-reports of health are also a significant predictor of future changes in functioning among the elderly.10 We code self-assessed health so that a higher number corresponds to better self-reported health (1=poor, 5=excellent). In phase 3, 12% of respondents reported their health was ‘excellent;’ 36% ‘very good;’ 40% ‘good;’ 10% ‘fair;’ and 1% ‘poor.’ We run ordered probit regressions to examine the associations between childhood circumstances, economic status in adulthood, and self-assessed health. The results presented are robust to estimating the models using ordinary least squares, using an indicator that health is reported to be ‘excellent’ or ‘very good’ as the dependent variable.
Table 6 presents results on the correlates of self-assessed health, including measures of occupational status at different points in time, cohort members’ heights, an indicator for whether the member reports having spent more than 4 weeks in the hospital as a child; and an indicator for whether the member reports the family owned a car when he or she was less than 16. Case and Paxson (2001) find that mother’s characteristics are associated with health-related behaviors, and for this reason we include controls for members’ reports that their mothers gave them ‘a great deal of time’ when growing up, and controls for mothers’ school leaving age and that age squared. We include members’ reports that a parent suffered from high blood pressure, stroke, angina, and diabetes. We continue to include a complete set of indicators for highest academic qualification when first leaving full-time education, and members’ ethnicity, sex, age and age squared. For ease of exposition, Table 6 displays only some of the ordered probit coefficients, and at the bottom of the table we show chi-square test statistics for the joint significance of subsets of coefficients.
Table 6.
Civil service grades and self-assessed health
| Dependent variable: Self-reported health status (5=Excellent, 4=Very Good, 3=Good, 2=Fair, 1=Poor) | ||||
|---|---|---|---|---|
| First grade at Whitehall | 0.104*** (0.034) | 0.024 (0.041) | −0.021 (0.053) | 0.016 (0.064) |
| Current grade at Whitehall | -- | 0.125*** (0.032) | −0.005 (0.058) | −0.006 (0.075) |
| Grade at next phase [current phase + 1] | -- | -- | 0.141*** (0.055) | -- |
| Grade at [current phase + 2] | -- | -- | -- | 0.136*** (0.070) |
| Height (cm) | 0.004 (0.002) | 0.005* (0.003) | 0.006* (0.003) | 0.004 (0.004) |
| Member spent 4+ weeks in hospital when <16 years old | −0.202*** (0.046) | −0.205*** (0.055) | −0.195*** (0.068) | −0.228*** (0.079) |
| Mother gave ‘a great deal of time’ while growing up | 0.209*** (0.031) | 0.187*** (0.036) | 0.176*** (0.044) | 0.185*** (0.051) |
| Chi-square test: Education qualification (p-value) | 28.96 (0.001) | 18.86 (0.042) | 17.32 (0.068) | 21.07 (0.021) |
| Chi-square test: family had a car, member hospitalized | 24.35 (0.000) | 17.65 (0.000) | 10.26 (0.006) | 8.83 (0.012) |
| Chi-square test: Mother gave time, mother’s education | 51.73 (0.000) | 32.14 (0.000) | 20.91 (0.000) | 20.14 (0.000) |
| Chi-square test: Parents’ illness | 27.78 (0.000) | 27.89 (0.000) | 16.10 (0.003) | 12.26 (0.016) |
| Number obs | 13557 | 8664 | 5199 | 2902 |
Notes. Ordered probit regression coefficients are presented, with standard errors in parentheses. Standard errors are clustered at the individual level. All regressions include controls for ethnicity, sex, age and age squared; a complete set of educational qualification indicators; members’ reports that their family had a car when less than 16; mother’s school-leaving age and school-leaving age squared; and indicators for members’ reports that either parent had had high blood pressure, diabetes, angina and stroke. Civil service grades are recorded: 1= clerical or office support; 2=professional or executive; 3= administrative.
Table 6 shows that self-assessed health is strongly related to occupational status at Whitehall. Column 1 shows that cohort members’ initial grades are significantly related to their current health. In addition, even with a control for starting grade, conditions of childhood are significantly associated with self-assessed health. Children who report having spent time in the hospital as a child are 7 percentage points less likely to report ‘excellent’ or ‘very good’ health. Mother’s variables, parental illness, and academic qualifications are all strongly associated with cohort members’ health.11
To examine whether childhood circumstances may act through their effects on promotion in Whitehall, we include current grade at Whitehall in our ordered probit regression in column 2. Current grade is strongly related to current health status, and its inclusion eliminates the association between starting grade and health status. Moving up one grade is associated with a 7 percentage point increase in the probability of reporting excellent or very good health. However, its inclusion does little to dampen the association between childhood circumstances and current health: coefficients change little, and the subsets continue to be highly jointly significant.
These results lead us back to the stubborn question of whether occupational grade is high because health is good, or whether health is good because occupational grade is high. Results in Table 5 suggest that promotion is related to health: promotion is predicted by better health in phase 1; by not reporting childhood hospitalisations; and by adult height. To get some purchase on this question, in Table 6 we add to our probit regressions measures of future occupational status. Specifically, column 3 adds occupational grade at the next phase of the Study. Future grade is highly and significantly correlated with current health, and its inclusion eliminates the association between current grade and health status. These results hold whether we include grade at the next phase of Whitehall (column 3), or the phase after that (column 4). It is difficult to make a case for future grade having a direct effect on current health. One might anticipate not being eligible for promotion, and this may lead to poorer health today, but it seems unlikely that one will anticipate equally well promotion in the next 3 years (occupational grade next phase) and in the next 6 years (occupational grade two phases into the future). An alternative explanation is that those in better health today are more likely to be promoted between the phases of the study.
One way to investigate these alternative explanations is to regress a measure of health on lags of civil service grade, to see if civil service grade predicts future health, and regress civil service grade on lags of health, to see if health predicts future civil service grade. Letting H denote health status and G denote civil service grade for cohort member i observed at time t, we express these regressions as:
| (6) |
| (7) |
Equation (6) regresses an indicator that the cohort member currently reports ‘excellent’ or ‘very good’ health on lags of civil service grade, age a at time t, and individual fixed effects, while equation (7) regresses current civil service grade on lags in health status (indicators of reporting ‘excellent’ or ‘very good’ health), age at time t, and individual fixed effects. The inclusion of individual fixed effects is important, as they will absorb aspects about individuals’ backgrounds that may determine both health status and economic status in adulthood, such as parents’ educations, occupations and health status; health and economic status in childhood; and educational attainment.
Fixed effect estimation requires the stringent assumption that all explanatory variables are strictly exogenous, an assumption that is unlikely to be true for our model of health and occupational status. For this reason, we estimate equations (6) and (7) using first difference models of the form:
| (8) |
and
| (9) |
and present results in Table 7. Here, we rely only on the second lag of employment grade (for equation 8) and health status (for equation 9), to minimize the odds that these right side variables are correlated with the first-differenced error term. We find no effect of civil service grade on future health. However, consistent with the results presented in Tables 5 and 6, we find a significant effect of health on future civil service grade. These results indicate that those who fall into worse health are less likely to be promoted, but that those who fail to be promoted are not more likely to fall into worse health. Overall, our findings are consistent with the “health selection” hypothesis and are not consistent with the “social causation” hypothesis.
Table 7.
Fixed effect first-difference models of occupational grade and health
| Dependent variable: | ||
|---|---|---|
| Change in health status for the indicator: Health is excellent or very good
|
Change in current civil service grade
|
|
| Explanatory variables: | ||
| Change in civil service grade (t − 2) − (t − 3) | 0.004 (0.015) | -- |
| Change in health (t − 2) − (t − 3) | -- | 0.028* (0.016) |
| Age | −0.006 (0.005) | −0.013 (0.017) |
| Number of observations | 17,069 | 2151 |
5. Conclusions
The results in this paper highlight three important issues for research on health and economic status over the life-course. The first finding is cautionary: samples of individuals who have been selected into certain occupational groups are not adequate to draw inference about the effects of childhood circumstance on adult outcomes for the population as a whole. Whitehall II is a remarkable study that has generated important insights about the evolution of health in adulthood. However, it is important to keep in mind that the Study is not representative of the population. Instead, it consists of people who entered white collar jobs in the British civil service in London. Our results from the NCDS and BCS indicate that estimated associations between childhood factors and adult health and economic outcomes are likely to be biased downward in absolute value in the Whitehall II study.
Our second major finding is that, despite the downward biases that are likely to result from selection into Whitehall II, we still find evidence that health and socioeconomic status in childhood influences occupational status in adulthood. Adults who had better childhood health—as measured by childhood hospitalisations and adult height—start at higher grades in the civil service on average, and are promoted to higher grades after they enter Whitehall. The association between height and occupational status in adulthood is robust to controls for education, implying that childhood health does not operate solely through its effects on educational attainment.
Finally, we present evidence that changes in self-assessed health are related to future changes in employment grade, and that changes in employment grade are not related to changes in future health. These findings are consistent with the hypothesis that the strong correlation between health and employment grade reflects the effects of health on success in the workplace. Our results stand in stark contrast to other studies based on Whitehall II, which downplay the role of health selection in employment. It should be noted that this finding, although striking, is based on only one measure of health—self-assessed health status. Although self-assessed health status is highly predictive of future mortality and is strongly correlated with a range of health conditions, different results may be obtained using different measures of health. In the future, it would be useful to examine whether similar results are obtained when different measures of health, such as cardiovascular disease or depression, are used in place of self-assessed health.
Acknowledgments
This paper has been written for Professor Angus Deaton’s festschrift, celebrating his presidency of the American Economic Association. We thank Dr. Aida Sanchez and the Whitehall II team for help accessing the Whitehall II data and Kimberly Bryan for expert research assistance. We thank all participating men and women in the Whitehall II Study; all participating Civil Service departments and their welfare, personnel, and establishment officers; the Occupational Health and Safety Agency; and the Council of Civil Service Unions. The Whitehall II Study team comprises research scientists, statisticians, study coordinators, nurses, data managers, administrative assistants and data entry staff, who make the study possible. Continuing data collection on this study is funded by the Medical Research Council, the National Institute on Aging (AG13196), National Heart Lung and Blood Institute (HL36310) and the British Heart Foundation. We gratefully acknowledge funding from the National Institutes of Health under the Demography of Aging Center grant P30 AG024361, and we thank referees and Scott Kostyshak for many useful suggestions.
Appendix Table 1.
Data used in our analysis from Whitehall II
| Phase 1 | Phase 2 | Phase 3 | Phase 4 | Phase 5 | Phase 6 | |
|---|---|---|---|---|---|---|
| Collection Dates: | 1985-88 | 1989-90 | 1991-94 | 1995-96 | 1997-99 | 2001 |
| Age | X | X | X | X | X | X |
| Sex | X | X | X | |||
| Ethnicity | X | |||||
| Father’s social class | X | |||||
| Mother’s school-leaving age | X | |||||
| Family owned a car < age 16 | X | |||||
| Spent 4+ weeks in hospital < age 16 | X | |||||
| Parent suffered from diabetes | X | |||||
| Parent suffered high blood pressure | X | |||||
| Parent suffered angina | X | |||||
| Parent suffered stroke | X | |||||
| Mother gave ‘a great deal of time’ when needed growing up | X | |||||
| Height in adulthood (mean) | X | X | X | |||
| Academic qualification when first left full-time education | X | |||||
| Health satisfaction at phase 1 | X | |||||
| First civil service grade | X | |||||
| Current civil service grade | X | X | X | X | X | X |
| Self-assessed health status | X | X | X | X |
Footnotes
Reviews of the growing literature on the fetal origins hypothesis are presented in Rasmussen (2001), McMillen and Robinson (2005), and Case and Paxson (2006). Barker (2004) and Black et al. (2007) provide recent studies.
Findings from the Whitehall II study are available at http://www.ucl.ac.uk/whitehallII/research/findings.
Virtanen et al. (2009) note that “participants in the Whitehall II study are almost exclusively white-collar civil servants” (p. 597). Similarly, Singh-Manoux et al. (2004) refer to the Whitehall II cohort as “white collar employees” (p. 1073).
Whitehall II cohort members were born between 1930 and 1950, and as a cohort have a mean and median year of birth of 1941. Until cohorts born in the late 20th Century, successive birth cohorts in Britain were taller on average, which can explain why the NCDS and BCS cohorts are taller on average than the Whitehall II cohort. In a cross-section of adults of all ages measured in the British Household Panel Study, each year of age in adulthood was associated with a 0.04 inch reduction in adult height on average (Case, Paxson and Islam 2009). This suggests that the Whitehall II sample is taller than would be expected if it was representative of the entire population of same-aged individuals.
Here we follow closely the treatment presented in Wooldridge (2002), Chapter 17. See also Angrist and Pischke (2009), Section 3.2.3, for discussion and examples.
If unobservables determining adult outcomes and those determining selection into Whitehall are uncorrelated, γ = 0. In this case, there is no selection problem, and OLS estimates from equation (1) will be consistent. If, controlling for other determinants of adult outcomes and selection βi and δi are of opposite signs, then estimated coefficients will be biased upward in absolute value.
Height was measured in phases 1, 3 and 5. We use the mean of the height measures recorded for each member. We have access to very few markers of health in childhood for the Whitehall II cohort. Hospitalisation for four or more weeks before age 16 is an indicator for a significant health issue. Information on additional measures of health in childhood (e.g. chronic conditions) is not available.
Results that do not include controls for entry grade are very similar to those presented in columns 2 and 4.
Results on initial grade and promotion in Table 5 hold when regressions are run separately for men and women.
Idler and Kasl (1995) and Bowling (2005) provide extensive references on studies that have employed self reported health status.
Similar results on the importance of education are presented by Smith (2007), who finds education critical to future health outcomes in the Panel Study of Income Dynamics.
References
- Angrist JD, Pischke J-S. Mostly Harmless Econometrics: An Empiricist’s Companion. Princeton: Princeton University; 2009. [Google Scholar]
- Barker DJP. The developmental origins of well-being. Philosophical Transactions of the Royal Society B. 2004;359(1449):1359–66. doi: 10.1098/rstb.2004.1518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowling A. Just one question: if one question works, why ask several? Journal of Epidemiology and Community Health. 2005;59(5):342–5. doi: 10.1136/jech.2004.021204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Black SE, Devereux PJ, Salvanes KG. From the cradle to the labor market? The effect of birth weight on adult outcomes. Quarterly Journal of Economics. 2007;122(1):409–39. [Google Scholar]
- Brunner E, Shipley MJ, Blane D, Davey Smith G, Marmot MG. When does cardiovascular risk start? Past and present socioeconomic circumstances and risk factors in adulthood. Journal of Epidemiology and Community Health. 1999;53:757–64. doi: 10.1136/jech.53.12.757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Case A, Paxson C. Mothers and others: who invests in children’s health? Journal of Health Economics. 2001;20:301–28. doi: 10.1016/s0167-6296(00)00088-6. [DOI] [PubMed] [Google Scholar]
- Case A, Paxson C. Children’s health and social mobility. The Future of Children. 2006;16(2):151–73. doi: 10.1353/foc.2006.0014. [DOI] [PubMed] [Google Scholar]
- Case A, Paxson C. Stature and status: height, ability, and labor market outcomes. Journal of Political Economy. 2008a;116(3):499–532. doi: 10.1086/589524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Case A, Paxson C. Height, health, and cognitive function at older ages. American Economic Review: Papers and Proceedings. 2008b;98(2):463–7. doi: 10.1257/aer.98.2.463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Case A, Paxson C. Causes and consequences of early life health. Demography. 2010;47(Supplement):S65–S85. doi: 10.1353/dem.2010.0007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Case A, Paxson C, Islam M. Making sense of the labor market height premium: evidence from the British Household Panel Survey. Economic Letters. 2009;102(3):174–6. doi: 10.1016/j.econlet.2008.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chandola T, Bartley M, Sacker A, Jenkinson C, Marmot M. Health selection in the Whitehall II Study, UK. Social Science and Medicine. 2003;56(10):2059–72. doi: 10.1016/s0277-9536(02)00201-0. [DOI] [PubMed] [Google Scholar]
- Currie J. Healthy, wealthy and wise: socioeconomic status, poor health in childhood, and human capital development. Journal of Economic Literature. 2009;47(1):87–122. [Google Scholar]
- Davey Smith G, Hart C, Hole D, MacKinnon P, Gillis C, Watt G, Blane D, Hawthorne V. Education and occupational social class: which is the more important indicator of mortality risk? Journal of Epidemiology and Community Health. 1998;52(3):153–60. doi: 10.1136/jech.52.3.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deaton A, Arora R. Life at the top: the benefits of height. Economics and Human Biology. 2009;7(2):133–6. doi: 10.1016/j.ehb.2009.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Idler EL, Kasl SV. Self-ratings of health: do they also predict change in functional ability? Journal of Gerontology: Social Sciences. 1995;50B(6):S344–S353. doi: 10.1093/geronb/50b.6.s344. [DOI] [PubMed] [Google Scholar]
- Marmot MG, Davey Smith G, Stansfeld S, Patel C, North F, Head J, White I, Brunner E, Feeney A. Health inequalities among British civil servants: The Whitehall II study. Lancet. 1991;337(8754):1387–93. doi: 10.1016/0140-6736(91)93068-k. [DOI] [PubMed] [Google Scholar]
- Marmot M, Shipley M, Brunner E, Hemingway H. Relative contribution of early life and adult socioeconomic factors to adult morbidity in the Whitehall II study. Journal of Epidemiology and Community Health. 2001;55:301–7. doi: 10.1136/jech.55.5.301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMillen IC, Robinson JS. Developmental origins of the metabolic syndrome: prediction, plasticity, and programming. Physiological Reviews. 2005;85:571–633. doi: 10.1152/physrev.00053.2003. [DOI] [PubMed] [Google Scholar]
- Rasmussen KM. The “fetal origins” hypothesis: challenges and opportunities for maternal and child nutrition. Annual Review of Nutrition. 2001;21:73–95. doi: 10.1146/annurev.nutr.21.1.73. [DOI] [PubMed] [Google Scholar]
- Singh-Manoux A, Ferrie JE, Chandola T, Marmot M. Socioeconomic trajectories across the life course and health outcomes in midlife: evidence for the accumulation hypothesis? International Journal of Epidemiology. 2004;33(5):1072–9. doi: 10.1093/ije/dyh224. [DOI] [PubMed] [Google Scholar]
- Smith JP. The impact of socioeconomic status on health over the life-course. Journal of Human Resources. 2007;42(4):739–764. [Google Scholar]
- Virtanen M, Singh-Manoux A, Ferrie JE, Gimeno D, Marmot MG, Elovainio M, Jokela M, Vahtera J, Kivimäki M. Long working hours and cognitive function. American Journal of Epidemiology. 2009;169(5):596–605. doi: 10.1093/aje/kwn382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wooldridge JM. Econometric Analysis of Cross Section and Panel Data. Cambridge, Massachusetts London, England: The MIT Press; 2002. [Google Scholar]