

Abstract
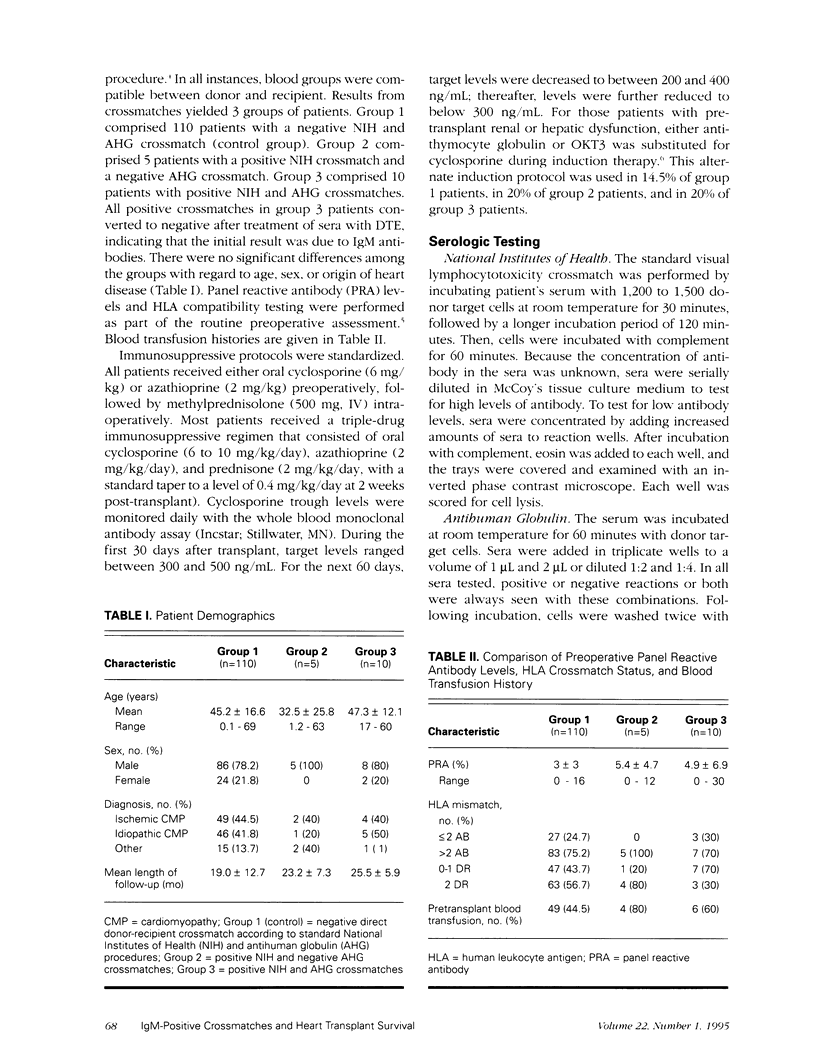
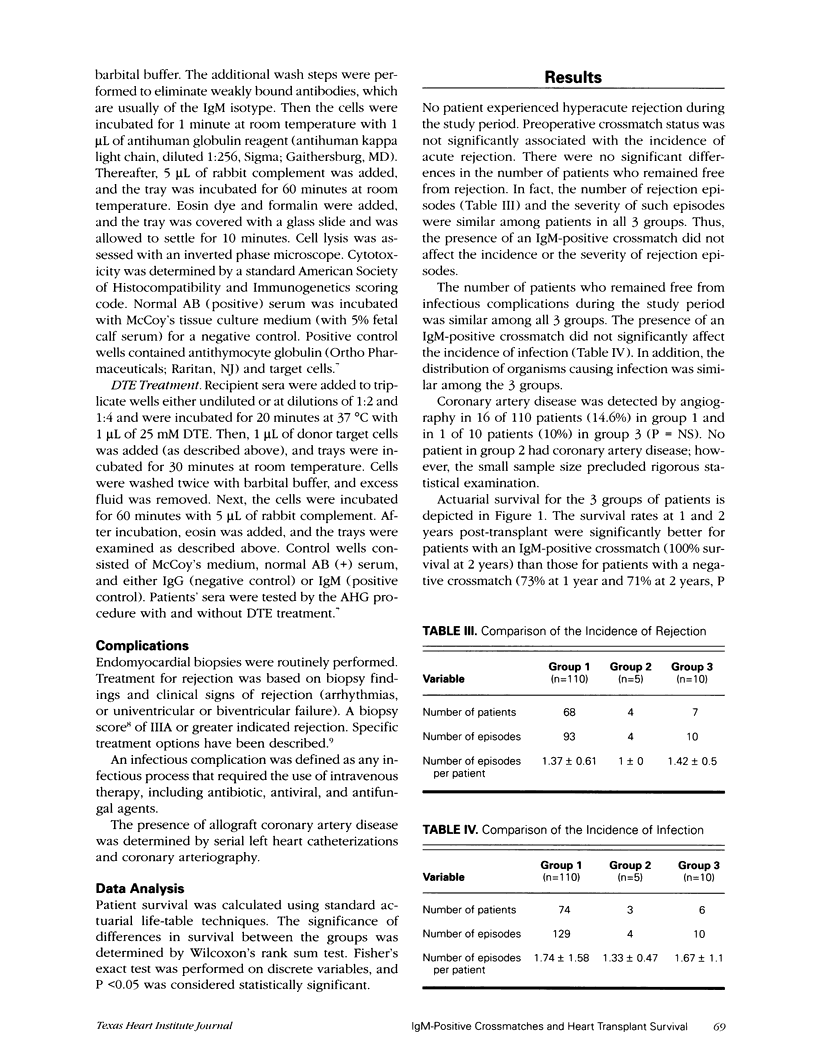
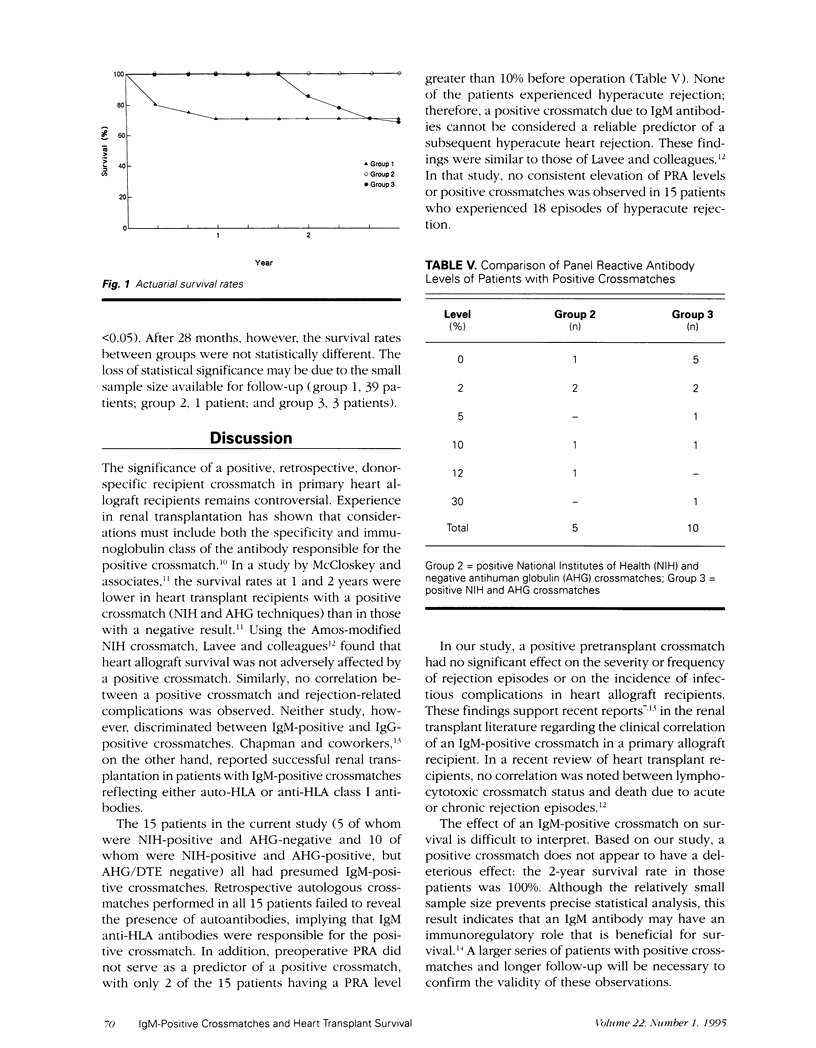
To determine whether an IgM-positive crossmatch adversely affects the results of heart transplantation, we conducted a retrospective study of 125 orthotopic heart transplant recipients. A direct donor-recipient crossmatch was performed retrospectively on sera from all patients by the standard National Institutes of Health (NIH) method and the antihuman globulin (AHG) procedure. The patients were then divided into 3 groups as follows. Group 1 comprised 110 patients with a negative NIH and AHG crossmatch (control group). Group 2 comprised 5 patients with a positive NIH crossmatch and a negative AHG crossmatch. Group 3 comprised 10 patients with positive NIH and AHG crossmatches. All positive crossmatches in group 3 patients converted to negative after treatment of sera with dithioerythritol, indicating that the initial result was due to IgM antibodies. All patients received standard immunosuppressive treatment. An IgM-positive crossmatch did not affect the number or severity of rejection episodes among the 3 groups, nor did it have an effect on the incidence of infection. Whereas coronary artery disease was detected by angiography in 16 of 110 patients (14.6%) in group 1 and in 1 of 10 patients (10%) in group 3 (P = NS), no patient in group 2 was affected. Actuarial survival at 1 and 2 years post-transplant was significantly better for patients with an IgM-positive crossmatch (group 2) (100% survival at 2 years) than for patients with a negative crossmatch (group 1) (73% at 1 year and 71% at 2 years, P < 0.05). Based on our study, the effect of an IgM-positive crossmatch on survival is difficult to interpret because of the small sample size. An IgM-positive crossmatch, however;did not appear to have a deleterious effect on survival. It may be that the IgM antibody has an immunoregulatory role. A larger series of patients with positive crossmatches and longer follow-up will be necessary to evaluate the importance of these results.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Billingham M. E., Cary N. R., Hammond M. E., Kemnitz J., Marboe C., McCallister H. A., Snovar D. C., Winters G. L., Zerbe A. A working formulation for the standardization of nomenclature in the diagnosis of heart and lung rejection: Heart Rejection Study Group. The International Society for Heart Transplantation. J Heart Transplant. 1990 Nov-Dec;9(6):587–593. [PubMed] [Google Scholar]
- Chapman J. R., Taylor C. J., Ting A., Morris P. J. Immunoglobulin class and specificity of antibodies causing positive T cell crossmatches. Relationship to renal transplant outcome. Transplantation. 1986 Dec;42(6):608–613. doi: 10.1097/00007890-198612000-00007. [DOI] [PubMed] [Google Scholar]
- Fuller T. C., Phelan D., Gebel H. M., Rodey G. E. Antigenic specificity of antibody reactive in the antiglobulin-augmented lymphocytotoxicity test. Transplantation. 1982 Jul;34(1):24–29. doi: 10.1097/00007890-198207000-00005. [DOI] [PubMed] [Google Scholar]
- Iwaki Y., Terasaki P. I., Park M. S., Billing R. Enhancement of human kidney allografts by cold B-lymphocyte cytotoxins. Lancet. 1978 Jun 10;1(8076):1228–1229. doi: 10.1016/s0140-6736(78)92464-9. [DOI] [PubMed] [Google Scholar]
- Kerman R. H., Kimball P. M., Van Buren C. T., Lewis R. M., DeVera V., Baghdahsarian V., Heydari A., Kahan B. D. AHG and DTE/AHG procedure identification of crossmatch-appropriate donor-recipient pairings that result in improved graft survival. Transplantation. 1991 Feb;51(2):316–320. doi: 10.1097/00007890-199102000-00008. [DOI] [PubMed] [Google Scholar]
- Kerman R. H. The role of crossmatching in organ transplantation. Arch Pathol Lab Med. 1991 Mar;115(3):255–259. [PubMed] [Google Scholar]
- Lavee J., Kormos R. L., Duquesnoy R. J., Zerbe T. R., Armitage J. M., Vanek M., Hardesty R. L., Griffith B. P. Influence of panel-reactive antibody and lymphocytotoxic crossmatch on survival after heart transplantation. J Heart Lung Transplant. 1991 Nov-Dec;10(6):921–930. [PubMed] [Google Scholar]
- McCloskey D., Festenstein H., Banner N., Hawes R., Holmes J., Khaghani A., Smith J., Yacoub M. The effect of HLA lymphocytotoxic antibody status and crossmatch result on cardiac transplant survival. Transplant Proc. 1989 Feb;21(1 Pt 1):804–806. [PubMed] [Google Scholar]
- McIntyre J. A., Boldt H. D., Faulk W. P., Halbrook H. Conversion of IgG-mediated complement-dependent cytotoxicity by reducing reagents. J Heart Lung Transplant. 1991 Jan-Feb;10(1 Pt 1):117–124. [PubMed] [Google Scholar]
- Radovancevic B., Birovljev S., Frazier O. H. Treating cardiac allograft rejection: present approach--analysis of 100 consecutive patients. J Heart Transplant. 1990 May-Jun;9(3 Pt 2):288–291. [PubMed] [Google Scholar]
- Radovancevic B., Birovljev S., Vega J. D., Lonquist J. L., Sweeney M. S., Vasiljevic J. D., Van Buren C. T., Kerman R. H., Frazier O. H. Inverse relationship between human leukocyte antigen match and development of coronary artery disease. Transplant Proc. 1991 Feb;23(1 Pt 2):1144–1145. [PubMed] [Google Scholar]
- Taylor C. J., Chapman J. R., Ting A., Morris P. J. Characterization of lymphocytotoxic antibodies causing a positive crossmatch in renal transplantation. Relationship to primary and regraft outcome. Transplantation. 1989 Dec;48(6):953–958. doi: 10.1097/00007890-198912000-00011. [DOI] [PubMed] [Google Scholar]
- Vaidya S., Ruth J. Contributions and clinical significance of IgM and autoantibodies in highly sensitized renal allograft recipients. Transplantation. 1989 Jun;47(6):956–958. doi: 10.1097/00007890-198906000-00008. [DOI] [PubMed] [Google Scholar]