

Abstract
AIM: To investigate the efficacy and safety of combined antiviral and immunosuppressant therapy in adult hepatitis B virus-associated glomerulonephritis (HBV-GN) patients.
METHODS: A computerized literature search was carried out in the PubMed database, Embase, the Cochrane Library, Chinese BioMedical Literature on disc, Chinese Medical Current Contents, Chinese National Knowledge Infrastructure, Wanfang and VIP (Chinese Technological Journal of Database) to collect articles between June 1980 and December 2010 on therapy with immunosuppressants, e.g., glucorticosteroids, mycophenolate mofetil and leflunomide, combined with antivirals, e.g., interferon, lamivudine, entecavir and adefovir dipivoxil, in adult HBV-GN patients. The primary outcomes were remission of proteinuria, clearance of HBV e-antigen, and elevation of serum albumin. The secondary outcomes were blood levels of alanine aminotransferase, serum creatinine, and HBV-DNA titer. Meta-analysis was performed using Review Manager 5.1. Fixed or random effect models were employed to combine the results after a heterogeneity test. The effects of the combined therapy were analyzed for different doses of glucorticosteroid and different types of HBV-GN.
RESULTS: Twelve clinical trials with 317 patients were included. A significantly higher incidence of HBV-GN was found in male patients (relative risk = 2.40, 95% CI: 1.98-2.93). Combined therapy reduced the proteinuria significantly with a mean difference of 4.19 (95% CI: 3.86-4.53) and increased the serum albumin concentration significantly with a mean difference of -11.95 (95% CI: -12.97-10.93) without significant alterations of liver function (mean difference: 4.62, 95% CI: -2.55-11.79) and renal function (mean difference: 10.29, 95% CI: 0.14-20.45). No significant activation of HBV-DNA replication occurred (mean difference: 0.12, 95% CI: -0.37-0.62). There was no significant difference between the high dose glucorticosteroid group and the low dose glucorticosteroid group in terms of proteinuria remission (P = 0.76) and between different pathological types of HBV-GN [membranous glomerulonephritis (MN) vs mesangial proliferative glomerulonephritis, P = 0.68; MN vs membranoproliferative glomerulonephritis, P = 0.27].
CONCLUSION: Combined antiviral and immunosuppressant therapy can improve the proteinuria in HBV-GN patients without altering HBV replication or damaging liver and renal functions.
Keywords: Meta-analysis, Hepatitis B virus-associated glomerulonephritis, Glucocorticoids, Immunosuppressant, Antiviral drug
INTRODUCTION
Hepatitis B virus (HBV) infection is an important public health problem worldwide and especially in developing countries such as China. It is estimated that there are up to 112 million chronic HBV carriers in China, and hepatitis B virus-associated glomerulonephritis (HBV-GN) remains one of the most common secondary glomerular diseases among the Chinese population[1]. Most HBV-GN patients present with the nephrotic syndrome and some show mild to moderate proteinuria with hematuria. The most common histological type of HBV-GN is membranous nephropathy[2,3]. Although spontaneous remission of HBV-GN has been reported in pediatric patients, it is not as successful for adult HBV-GN patients as for children[3]. There is still considerable morbidity and significant mortality in the world; about 30% of adult patients may progress to renal failure, and as many as 10% of these will require maintenance dialysis[2].
HBV-GN treatment includes antiviral drugs, e.g., interferon (IFN), lamivudine (LAM), entecavir (ETV) and adefovir dipivoxil (ADV), or immunosuppressants, e.g., glucocorticosteroids, mycophenolate mofetil (MMF) and leflunomide (LEF). Although antivirals have proven to be effective in clearing the viral antigens and abrogating the proteinuria[2,4], the safety and efficacy of immunosuppressants are still controversial. It has been argued that immunosuppressants are not appropriate for HBV-GN because of concerns such as induction of HBV replication, liver damage, and even deterioration of renal lesions[5-7].
In a recent meta-analysis study, Zhang et al[8] showed that treatment of HBV-GN with corticosteroids only (monotherapy) was not effective with regard to proteinuria remission. However, this conclusion was drawn by analyses of data from both adult and pediatric patients, and because spontaneous remission can occur in children, this could have confounded the effectiveness of corticosteroid treatment in adult patients. In addition, the number of adult patients treated with glucorticosteroids in that study was only thirteen. The efficacy of combined therapy was not evaluated[8].
On the other hand, treatment of HBV-GN without immunosuppressants has been reported to lead to progressive kidney disease[9]. In fact, along with antivirals, glucorticosteroids are being widely and empirically used for patients with HBV-GN, especially those in the Asia-Pacific regions[10]. However, to date, there has not been a meta-analysis on the efficacy and safety of this combined therapy in adults.
Thus the purpose of this study was to analyze the published data on the efficacy and safety of combined therapy with antivirals and immunosuppressants for adult patients with HBV-GN. To accomplish this, we performed a systematic review and meta-analysis of all published clinical trials that met our entry criteria.
MATERIALS AND METHODS
Search strategy and data extraction
We searched MEDLINE, EMBASE, Cochrane Library, and the Chinese BioMedical Literature on disc (CBM), Chinese Medical Current Contents (CMCC), Chinese National Knowledge Infrastructure (CNKI), Wanfang and VIP (Chinese Technological Journal of Database). The key words were; “hepatitis B virus”, “glomerulonephritis”, “prednisolone”, “nephrotic syndrome”, “mycophenolate mofetil”, “immunosuppressants”, “drug therapy”, and their synonyms and related terms. All articles were identified by searching from June 1980 to December 2010. In addition, manual searches of selected specialty journals were performed to identify all pertinent literature. Qualitative reviews and published clinical trials were also searched.
Criteria for inclusion
Eligible patients had to be adults (age > 18 years) with renal biopsy-proven HBV-GN. We included randomized controlled trials (RCTs), controlled clinical trials (CCTs), prospective and retrospective self-controlled studies, and cohort studies that used immunosuppressants and antivirals to treat HBV-GN. The data had to be published in a full length paper, and all had a follow-up period of at least 6 mo. The primary and secondary outcomes were a decrease of proteinuria, levels of serum albumin and alanine aminotransferase (ALT), renal function, and HBV-DNA titer.
Criteria for exclusion
Studies were excluded if the data on the measurements of the responses were incomplete or the HBV-GN was treated with Chinese herbal drugs. Trials published as abstracts or as interim reports were excluded, but letters and review articles were not excluded. For serial reports of the same patients, only those articles that provided the most comprehensive information were included. Trials with immunosuppressants only were also excluded.
Definitions of outcome measures
The primary outcome measures were proteinuria remission and HBV reactivation. Secondary outcome measures were elevations of ALT, serum creatinine (Scr), serum albumin, and other adverse effects such as a transient increase in transaminases, dizziness, fatigue, and gastrointestinal symptoms. A complete remission (CR) was defined as disappearance of proteinuria after treatment, and partial remission was defined as a 24 h urinary protein decreased more than 50% of the previous value[11]. Cases that had no improvement of symptoms and laboratory tests were classified as non-responsive.
HBV reactivation was defined as the presence of detectable serum HBV DNA, and an ALT elevation was defined as an increase to > 50 U/L[12]. A relapse was defined as the reappearance of > 1+ albuminuria on urinalysis. A low-dose glucorticosteroid (prednisone or prednisolone) was defined as ≤ 0.5 mg/kg per day, and high-dose glucorticosteroid was defined as ≥ 1.0 mg/kg per day.
Data extraction and quality assessment
Two reviewers (Zheng XY and Wei RB) independently selected the studies and extracted the data and outcomes according to the inclusion criteria. In cases of disagreement between the two reviewers, a third reviewer (Tang L) examined the data and discussed the choices with the two initial reviewers. The data were incorporated only when the three reviewers reached a consensus.
Statistical analysis
For dichotomous outcomes, the results are expressed as relative risk (RR) with 95% confidence intervals (CI) for individual studies. When the outcomes were measured on a continuous scale, the mean difference (MD) was used to evaluate the difference in the change from the beginning to the end of treatment. The meta-analysis was performed using the fixed-effect or random-effect methods depending on the absence or presence of significant heterogeneity. Heterogeneity was measured using Chi-square (χ2) and I² tests, and statistical significance was considered to be present when P < 0.05. In the absence of heterogeneity, the Mantel-Haenszel method of the fixed-effect model was used for the meta-analysis. Otherwise, the DerSimonian and Laird method for the random-effect model was selected[13]. The RR with 95% CI was used to assess the treatment efficacy. The combined results were the average RR and 95% CI weighted according to the standard error of the RR of the trial. A P < 0.05 was considered statistically significant. Funnel plots were used to assess the publication bias, and funnel plot asymmetry was tested using the Egger’s test and Begg’s test[14,15]. All analyses were performed with the Review Manager version 5.1 (RevMan, Cochrane Collaboration, Oxford, England).
RESULTS
Description of trials included in meta-analysis
Our electronic and manual searches identified 774 studies. After a review of the titles and abstracts or full text, 762 articles were excluded and 12 articles[9,16-26] with 317 patients were included based on the criteria mentioned (Cheng CL 2005, Dang YM 2004, Fang YQ 2009, He LS 2007, Liu J 2010, Liu ZH 2008, Sun LL 2005, Sun XP 2010, Tang L 2005, Tang Y 2005, Wu SB 2008 and Xia DQ 2009; Figure 1 and Tables 1-3). The numbers of patients studied in each trial were 20, 24, 58, 13, 25, 30, 11, 29, 9, 21, 35 and 42, respectively. One of these studies was a RCT[23], three were CCT[9,18,24], and the others were prospective and retrospective self-controlled studies[16,17,19-22,25,26]. The characteristics of the 12 clinical trials included are shown in Table 1, and detailed information of the interventions such as dose and duration of medication, main outcomes, and follow-up periods are summarized and tabulated in Tables 2 and 3.
Figure 1.
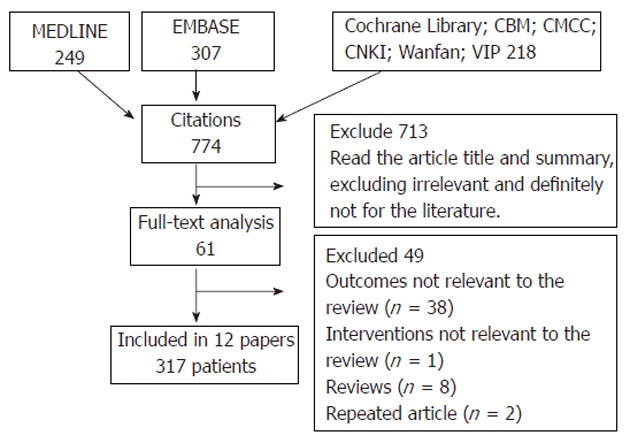
Flowchart showing the abstract screening and study selection process. CBM: Chinese BioMedical Literature on disc; CMCC: Chinese Medical Current Contents; CNKI: Chinese National Knowledge Infrastructure.
Table 1.
Characteristics of 12 included studies
| Ref. | Region | Patients | Study design | |
| Gender | Mean age (yr) | |||
| Fang et al[9] | Zhejiang | NA | > 18 | CCT study |
| Cheng et al[16] | Guangzhou | 21 M, 3 F | 29.3 ± 10.3 | Self-control study |
| Dang et al[17] | Shandong | 38 M, 20 F | 41 | Self-control study |
| He et al[18] | Beijing | NA | > 18 | CCT study |
| Liu et al[19] | Shandong | 17 M, 8 F | 39.6 ± 11.2 | Self-control study |
| Liu et al[20] | Hunan | 20 M, 10 F | 31.4 ± 13.8 | Self-control study |
| Sun et al[21] | Shanghai | 9 M, 4 F | 34.4 ± 10.4 | Self-control study |
| Sun et al[22] | Shandong | 22 M, 7 F | > 18 | Self-control study |
| Tang et al[23] | Beijing | 8 M, 1 F | 38.2 ± 11.2 | RCT study |
| Tang et al[24] | Guangzhou | 16 M, 5 F | 31 ± 8.9 | CCT study |
| Wu et al[25] | Shanghai | 23 M, 12 F | 40.5 ± 10.4 | Self-control study |
| Xia et al[26] | Shandong | 28 M, 14 F | 35.4 ± 17.1 | Self-control study |
M: Male; F: Female; NA: Not available; RCT: Randomized controlled trial; CCT: Clinical controlled trial.
Table 3.
Various changes of interventions used in individual studies
| Ref. | n | ALT (U/L) | Scr (μmol/L) | Albumin (g/d) | Proteinuria (g/d) | Proteinuria | HBV-DNA titer | ||||||
| Before | After | Before | After | Before | After | Before | After | CR | PR | Before | After | ||
| Fang et al[9] | 20 | NA | NA | NA | NA | NA | NA | NA | NA | 13/20 (12 mo) | 6/20 (12 mo) | NA | NA |
| Cheng et al[16] | 24 | NA | NA | NA | NA | 21.0 ± 4.2 | 35.4 ± 6.5 | 6.3 ± 2.3 | 1.1 ± 1.2 | 9/24 | 11/24 | 5.2 ± 1.6 (12 mo) | 5.1 ± 1.7 (12 mo) |
| Dang et al[17] | 58 | 21.0 ± 10.3 | 21.6 ± 12.5 | 97.3 ± 38.2 | 92.5 ± 38.6 | 26.4 ± 4.9 | 39.0 ± 4.7 | 4.2 ± 2.1 (12 mo) | 1.3 ± 1.5 (12 mo) | 19/58 | 24/58 | NA | NA |
| He et al[18] | 13 | NA | NA | NA | NA | 25.8 ± 6.3 | 34.7 ± 7.0 | 7.3 ± 3.5 | 2.8 ± 1.4 | NA | NA | NA | NA |
| Liu et al[19] | 25 | 72.5 ± 13.7 | 42.1 ± 8.2 | NA | NA | 26.4 ± 8.1 | 37.1 ± 2.1 | 6.0 ± 3.7 | 1.8 ± 0.9 | 5/25 | 15/25 | NA | NA |
| Liu et al[20] | 30 | 65.9 ± 23.6 | 62.6 ± 15.0 | 135.1 ± 83.5 | 86.0 ± 24.5 | 26.9 ± 6.0 | 37.8 ± 2.3 | 5.6 ± 3.4 | 1.9 ± 1.1 | 12/30 (9 mo) | 12/30 (9 mo) | NA | NA |
| Sun et al[21] | 11 | NA | NA | NA | NA | 25.3 ± 2.4 | 33.7 ± 3.1 (12 mo) | 6.7 ± 2.5 | 2.1 ± 1.7 | 4/11 (12 mo) | 5/11 (12 mo) | NA | NA |
| Sun et al[22] | 29 | NA | NA | 105.0 ± 43.5 | 93.5 ± 35.2 | 29.5 ± 7.8 | 38.3 ± 6.9 | 85.8 ± 39.0 (mg/kg per day) | 15.6 ± 8.4 (mg/kg per day) | NA | NA | NA | NA |
| Tang et al[23] | 9 | 27.4 ± 25.2 | 22.9 ± 4.3 | 95.3 ± 33.8 | 89.6 ± 34.3 | 26.0 ± 6.2 | 35.1 ± 5.6 | 4.9 ± 2.9 | 1.4 ± 0.7 | 4/9 | 4/9 | NA | NA |
| Tang et al[24] | 21 | 27.0 ± 17 | NA | NA | NA | 22.4 ± 4.5 | 36.8 ± 5.6 | 5.0 ± 2.1 | 1.0 ± 1.33 | 15/21 | 3/21 | 5.3 ± 1.7 (12 mo) | 5.1 ± 1.7 (12 mo) |
| Wu et al[25] | 35 | NA | NA | 135.3 ± 15.2 | 78.2 ± 11.5 (12 mo) | 20.3 ± 4.9 | 41.6 ± 4.3 (12 mo) | 5.2 ± 1.3 | 1.1 ± 0.1 | 20/35 | 10/35 | 4.8 ± 1.4 (12 mo) | 4.7 ± 1.6 (12 mo) |
| Xia et al[26] | 42 | 63.2 ± 22.9 | 43 ± 10.2 (12 mo) | 126.6 ± 73.9 | 81.5 ± 13.9 (12 mo) | 26.9 ± 6.5 | 37.8 ± 2 (12 mo) | 3.5 ± 2.1 | 0.7 ± 0.4 (12 mo) | 7/42 (12 mo) | 29/42 (12 mo) | NA | NA |
Unless specified data are shown at 6 mo examination after treatment; ALT: Alanine aminotransferase; Scr: Serum creatinine; NA: Not available; CR: Complete remission; PR: Partly remission; HBV: Hepatitis B virus.
Table 2.
Categories of interventions used in individual studies and duration of follow-up
| Ref. | Intervention | Duration | Follow-up | Dropout (n) |
| Fang et al[9] | Prednisone 0.8-1.0 mg/kg per day + LAM/ETV/ADV | 12 mo | 40 mo | 0 |
| Cheng et al[16] | Prednisolone 0.4 mg/kg per day + MMF + LAM | 6 mo | 6 mo | 0 |
| Dang et al[17] | Prednisone 0.8-1.0 mg/kg per day + MMF + LAM | 6 mo | 6 mo | 0 |
| He et al[18] | Prednisone 40-60 mg/d + MMF | 18 mo | 12 mo | 0 |
| Liu et al[19] | prednisolone 0.5-1.0 mg/kg per day + MMF + LAM | 12 mo | 12 mo | 0 |
| Liu et al[20] | Prednisone 1.0 mg/kg per day + ETV | 9 mo | 9 mo | 0 |
| Sun et al[21] | Prednisone 0.5 mg/kgper two days + MMF + LAM | 12 mo | 12 mo | 2 |
| Sun et al[22] | Prednisone 1.0 mg/kg per day + ADV | 6 mo | 12 mo | 0 |
| Tang et al[23] | Prednisone 0.5-0.8 mg/kg per day + MMF | 6 mo | 12 mo | 0 |
| Tang et al[24] | Prednisolone 0.4 mg/kg per day + MMF + LAM | 6 mo | NA | 0 |
| Wu et al[25] | Prednisolone 0.4 mg/kg per two days + MMF + LAM | 6 mo | 12 mo | 0 |
| Xia et al[26] | Prednisone 0.5 mg/kg per day + LEF +LAM | 6 mo | 12 mo | 0 |
MMF: Mycophenolate mofetil; LAM: Lamivudine; ETV: Entecavir; ADV: Adefovir dipivoxil; LEF: Leflunomide; IFNα: Interferon α; NA: Not available.
Clinical characteristics of gender differences
Gender differences in the incidence of HBV-GN were assessed from the results of 10 trials[16,17,19-26] including 1 RCT[23], 1 CCT[24], and 8 self-controlled studies[16,17,19-22,25,26]. The total number of patients was 286, including 202 male patients and 84 female patients. The χ2 test of heterogeneity was not significant (P = 0.37), therefore the fixed-effect model was selected. A significantly larger number of male patients than female patients had HBV-GN (RR = 2.40, 95% CI: 1.98-2.93; Figure 2).
Figure 2.

Gender difference in trials. M-H: Mantel-Haenszel.
Efficacy of combined therapy for proteinuria
The efficacy of combined therapy for proteinuria of six months duration was assessed from the results of 8 trials[16,18-21,23-25] including 1 RCT[23], 2 CCT[18,24], and 5 self-controlled studies[16,19-21,25]. The total number of patients was 170, and the χ2 test of heterogeneity was not significant (P = 0.62). Therefore, the fixed-effect model was used. There was a significant decrease in the level of proteinuria after the treatments (mean difference: 4.19, 95% CI: 3.86-4.53, Figure 3).
Figure 3.

Proteinuria change in steroid combination therapy. IV: Inverse variance.
Efficacy of combined therapy on serum albumin concentration
The efficacy of combined therapy on serum albumin concentration was assessed from the results of 8 trials[16-20,22-24] of 209 patients including 1 RCT[23], 2 CCT[18,24], and 5 self-controlled studies[16,17,19,20,22]. The χ2 test of heterogeneity was not significant (P = 0.11), therefore the fixed-effect model was selected. A significant increase in the level of serum albumin was found after the treatments (mean difference: -11.95, 95% CI: -12.97-10.93, Figure 4).
Figure 4.

Serum albumin change in combination therapy group. IV: Inverse variance.
Safety of combined therapy regarding liver function
Liver function was evaluated by assessing the level of ALT. The change in the ALT level after steroid combined therapy for HBV-GN was assessed from the results of 4 trials[17,19,20,23] including 1 RCT[23] and 3 self-controlled studies[17,19,20]. The total number of patients was 122. The χ2 test of heterogeneity was significant (P = 0.03), therefore the random-effect model was selected. There was no significant difference after the treatment (P = 0.21, Figure 5); a transient elevation of ALT was noted in 14 patients during the treatment but the treatment was not stopped. Elevation of ALT was the most common side effect of combined therapy and accounted for 4.4% (14/317) of all the participants. These findings demonstrate the necessity of monitoring liver function during the treatment.
Figure 5.

Alanine aminotransferase change in combination therapy group. IV: Inverse variance.
Safety of combined therapy regarding renal function
Renal function was assessed by evaluating the change in the serum creatinine (Scr) level. The level of Scr after combined therapy for HBV-GN was assessed from the results of 4 trials[17,20,22,23], including 1 RCT[23] and 3 self-controlled studies[17,20,22]. The total number of patients was 126, and the χ2 test of heterogeneity was not significant (P = 0.13). Therefore, the fixed-effect model was used. There was no significant increase in the level of Scr after the treatments (P = 0.05, Figure 6).
Figure 6.

Scr change in combination therapy group. IV: Inverse variance.
HBV-DNA titer
A change in the HBV-DNA titer after combined therapy for HBV-GN was assessed from the results of 3 trials[16,24,25] including 1 CCT[24] and 2 self-controlled studies[16,25]. The total number of patients was 80. The χ2 test of heterogeneity was not significant (P = 0.99), and the fixed-effect model was used. There was no significant difference in the HBV-DNA titer before and after the treatments (P = 0.63, Figure 7). However, in one of the 12 articles included in this meta-analysis, one patient was reported to have an increase in the HBV-DNA titer after 5 mo of treatment, but the titer was stabilized following treatment with ADV[9].
Figure 7.

Hepatitis B virus-DNA titer change in combination therapy group. IV: Inverse variance.
Proteinuria in high-dose steroid subgroup vs low-dose steroid subgroup
The change in the proteinuria level in the high-dose steroid therapy group was assessed from the results of 3 trials[18,19,23] including 1 RCT[23], 1 CCT[18], and 1 self-controlled study[19]. The total number of patients was 47, and the χ2 test of heterogeneity was not significant (P = 0.77). Therefore, the fixed-effect model was used. High-dose steroid was found to reduce the proteinuria significantly (mean difference: 4.08, 95% CI: 3.06-5.11, Figure 8). Low-dose steroid therapy was assessed from the results of 4 trials[16,21,24,25] including 1 CCT[24] and 3 self-controlled studies[16,21,25]. The total number of patients was 93, and the χ2 test of heterogeneity was not significant (P = 0.25). Therefore, the fixed-effect model was used. Low-dose steroid was also found to significantly reduce proteinuria (mean difference: 4.25, 95% CI: 3.88-4.61, Figure 8).
Figure 8.

Proteinuria remission rate in different dose glucorticosteroids subgroups. IV: Inverse variance.
The two subgroups were merged for analysis, and the χ2 test of heterogeneity of the two subgroups was not significant (P = 0.58). Therefore, the fixed-effect model was used. The combined therapy reduced proteinuria significantly after treatment (mean difference: 4.23, 95% CI: 3.89-4.57, Figure 8), and there was no significant difference between the two subgroups (P = 0.76, Figure 8).
Proteinuria changes in membranous glomerulonephritis subgroup vs mesangial proliferative glomerulonephritis subgroup
Comparisons of the rate of remission or the rate of complete remission in proteinuria between the membranous glomerulonephritis (MN) and mesangial proliferative glomerulonephritis (MsPGN) subgroups were assessed from the results of 6 trials[16,19,21,22,24,26] including 1 CCT[24] and 5 self-controlled studies[16,19,21,22,26]. The total number of patients was 73 for the MN group and 35 for the MsPGN group (Table 4). The χ2 test of heterogeneity was not significant (P = 0.79 and P = 0.62, respectively), therefore the fixed-effect model was selected. The proteinuria remission rate did not differ between the two subgroups (RR = 0.94, 95% CI: 0.78-1.12, Figure 9). Also the complete remission rate of proteinuria did not differ between the two subgroups (RR = 0.84, 95% CI: 0.51-1.37, Figure 9).
Table 4.
Pathological type and proteinuria remission rate
| Ref. | Proteinuria remission rate | Pathological type and proteinuria remission rate | ||||||||
| MN | MPGN | MsPGN | ||||||||
| R | CR | PR | R | CR | PR | R | CR | PR | ||
| Cheng et al[16] | 20/24 | 3/5 | 1/5 | 2/5 | 6/7 | 1/7 | 5/7 | 5/6 | 2/6 | 3/6 |
| Liu et al[19] | 20/25 | 11/15 | 2/15 | 9/15 | 0 | 0 | 0 | 6/7 | 3/7 | 3/7 |
| Sun et al[21] | 9/11 | 3/4 | 1/4 | 2/4 | 1/2 | 0/2 | 1/2 | 3/3 | 1/3 | 2/3 |
| Sun et al[22] | 26/29 | 11/12 | 7/12 | 4/12 | 7/9 | 3/9 | 4/9 | 5/6 | 2/6 | 3/6 |
| Tang et al[24] | 18/21 | 6/7 | 5/7 | 1/7 | 1/2 | 0/2 | 1/2 | 6/6 | 6/6 | 0/6 |
| Xia et al[26] | 36/42 | 28/30 | 6/30 | 22/30 | 1/1 | 0/1 | 1/1 | 6/7 | 1/7 | 5/7 |
MN: Membranous glomerulonephritis; MPGN: Membranoproliferative glomerulonephritis; MsPGN: Mesangial proliferative glomemlonephrits; R: Remission; CR: Complete remission; PR: Partly remission.
Figure 9.

Proteinuria remission rate in membranous glomerulonephritis and mesangial proliferative glomerulonephritis subgroups. M-H: Mantel-Haenszel; MN: Membranous glomerulonephritis; MsPGN: Mesangial proliferative glomemlonephrits; CR: Complete remission; R: Remission.
Change in level of proteinuria in MN subgroup vs membranoproliferative glomerulonephritis subgroup
Comparisons of the remission rate and the complete remission rate of proteinuria between MN and membranoproliferative glomerulonephritis (MPGN) subgroups were assessed from the results of 5 trials[16,21,22,24,26] including 1 CCT[24] and 4 self-controlled studies[16,21,22,26]. The total number of patients was 79; 58 in the MN subgroup and 21 in the MPGN subgroup (Table 4). The χ2 test of heterogeneity was not significant (P = 0.73 and 0.94, respectively), and therefore the fixed-effect model was used. The proteinuria remission rate did not differ between the two subgroups (RR = 1.13, 95% CI: 0.81-1.56, Figure 10), and also the complete remission rate did not differ between the two subgroups (RR = 1.84, 95% CI: 0.81-4.19, Figure 10).
Figure 10.

Proteinuria remission rate in membranous glomerulonephritis and membranoproliferative glomerulonephritis subgroups. M-H: Mantel-Haenszel; MN: Membranous glomerulonephritis; MPGN: Membranoproliferative glomerulonephritis; CR: Complete remission; R: Remission.
Other adverse events
None of the studies assessed any other serious adverse events associated with the combined treatments. Almost all patients showed good tolerance although some patients had a transient increase in transaminases (4.4%), diarrhea (1.9%), loss of appetite (1.26%), influenza-like illness (0.3%), dizziness (0.3%), and anemia (1.26%). These side effects did not affect the completion and follow-up of the treatments.
Risk of bias in included studies
The overall quality of the studies included in this meta-analysis was suboptimal. Three studies had adequate allocation concealment and in all the rest the allocation concealment method was unclear. No study masked the participants or investigators to the intervention. Masking of the outcome assessors was done in only two studies and almost all the studies included did not analyze the results on an intention-to-treat basis. Because different outcomes and different comparisons were reported, and often without full statistical details, it was not possible to meta-analyze all the data. Risk of bias graph and summary are shown in Figures 11 and 12.
Figure 11.

Risk of bias graph: Review authors' judgments about each risk of bias item presented as percentages across all included studies.
Figure 12.

Risk of bias graph: Review authors' judgments about each risk of bias item for each included study.
Publication bias
The funnel plots of the study results against precision are shown in Figure 13 with the 95% confidence limits. No obvious publication bias was found in our meta-analysis.
Figure 13.

Publication bias analysis. A: Funnel plots of proteinuria treatment with steroid combination therapy; B: Funnel plots of serum albumin change with steroid combination therapy; C: Funnel plots of proteinuria change under different combined glucorticosteroids drugs; D: Funnel plots of remission rate vs complete remission rate of MN and MsPGN groups; E: Funnel plots of remission rate vs complete remission rate of MN and MsPGN groups. MN: Membranous glomerulonephritis; MsPGN: Mesangial proliferative glomemlonephrits; R: Remission; CR: Complete remission; RR: Relative risk; MD: Mean difference.
DISCUSSION
HBV-GN is an uncommon but a well-described complication of chronic hepatitis B. There is a high incidence of morbidity and mortality although remission with preservation of renal function has been reported[2]. HBV-GN has been reported from all over the world[10,27-31], but China is known to be the most endemic area with a high incidence of progressive HBV-GN and poor prognosis in adults[32]. Case reports and small scale reports have been published, but unfortunately a standardized treatment protocol and justification for the current therapeutic regimen are lacking.
Antiviral drugs have been recommended for treatment of HBV-GN because they can inhibit HBV replication and reduce proteinuria[31,33-35]. The mechanisms by which antivirals including IFN and the nucleoside analogues, e.g., lamivudine and entecavir, reduce the nephrotic syndrome and decrease the proteinuria are known to be by their viral suppression and HBeAg seroconversion, reduction of serum HBV DNA, normalization of serum alanine transaminase[36]. On the other hand, the virological features of HBV, i.e., the genotype or viral load, genetic barrier, drug potency, patient adherence, and the duration of HBV infection, could play important roles in viral resistance even with nucleoside analogues that target the HBV DNA polymerase[37]. For patients who do not respond well to the antiviral therapy or/and have little signs of proteinuria remission, immunosuppressants, especially the glucorticosteroids, are often empirically used in clinics. This is even true for cases treated in developing countries such as China[38]. In fact, immune complexes have been identified in the kidney indicating that the pathogenesis of HBV-GN may be associated with an immune reaction. This could be supportive for the use of immunosuppressants. However, the use of steroids is still controversial because of the risk of activating viral infections[3]. In addition, the efficacy of steroids has not been definitively determined.
It has been claimed that HBV-GN occurs predominantly in children and mainly in male patients[39]. The incidence of male patients has been reported to be about 1.5 to 2 times that of female patients[40]. Our meta-analysis of 286 adult patients from 10 studies showed that there were 2.4 times more male patients than female patients. Because all of the trials in this study were from China and considering the fact that China has a relatively larger population of men than women (Census Bureau released in 2011: Chinese male to female population ratio = 120:100), our analysis showed a still higher incidence of male patients.
The use of prednisone has been reported to cause a significant increase in the levels of HBeAg and HBV-DNA[5]. One recent meta-analysis also claimed that glucocorticoid monotherapy did not significantly improve proteinuria[8]. However, favorable effects of glucocorticoids have also been reported in reduction of proteinuria in MsPGN/MN cases following HBV infection[10]. In addition, the proteinuria remission rate of HBV-GN after glucocorticoid treatment in adults has been reported to be 75% which is much higher than that for antiviral treatment (28.6%)[10].
Our analysis showed that most patients with HBV-GN were successfully treated with combined antiviral and immunosuppressant therapy with an overall estimated rate for proteinuria remission of 83%. Only 2 patients in the treated group dropped out but both were due to economic reasons. Our analyses also demonstrated that the combined therapy can effectively elevate the level of serum albumin. To the best of our knowledge, few reports exist in literature regarding the comparison of combined therapy with monotherapy of either antivirals or immunosuppressants. Thus, it could be an overstatement to conclude that the combined therapy is superior to antivirals or steroids. However, at least our meta-analysis provides evidence showing the efficacy and safety of this combined therapy of antivirals and immunosuppressants, which is actually a widespread practice in China.
Low-dose steroid therapy is aimed at reducing HBV replication while minimizing the risk of HBV activation. Both high-dose and low-dose groups showed similar efficacy of proteinuria reduction following treatment, indicating that low-dose steroid is effective and should be recommended for its safety. In addition, all of the reviewed patients tolerated steroid therapy well without occurrence of liver dysfunction or renal insufficiency.
Our analysis also revealed that no significant increase in the viral titers was observed after combined therapy. However, because the observation time was relatively short, long term effects of the combined therapy should be evaluated in the future.
The most common pathological type of HBV-GN is membranous nephropathy (MN; 50%), followed by MPGN and MsPGN[3]. Our study of 6 trials (152 patients) showed that MN accounted for 48% and MPGN + MsPGN for 36.8% of the phenotypes of HBV-GN. To determine the efficacy of combined therapy for the different pathological types, the trials were divided into three subgroups: MN, MsPGN, and MPGN. The proteinuria remission rate and complete remission rate were compared between the MN group and the MPGN group. There was no significant difference between the two groups. Comparisons of other pathological types could not be included in this analysis because the number of patients was small. Further studies of larger sample sizes are needed to solve this question.
As with all meta-analyses, our study had some biases. Firstly, negative trials are sometimes less likely to be published. To overcome this, we tried to obtain data from as many sources as possible. We used Funnel plots to test our review for publication bias. The risk of having missed trials was acceptably low. Secondly, the number of high quality clinical trials and number of studied patients were limited. Thirdly, we found that randomization and masking were not satisfactory and the allocation concealment of many studies was not available. Therefore, selection bias cannot be completely ruled out. More adequately powered RCTs with sufficient follow-up periods are definitely needed in future studies. Such RCTs should assess clinically important outcomes such as mortality, long-term relapse rate, and long-term HBV-DNA titer. Furthermore, the antiviral therapy should also be in a standard format in conformity with the APASL guidelines (Seoul 2008)[41], which would be beneficial for future analysis.
In summary, our meta-analysis of 12 clinical trials showed that combined therapy with antivirals and immunosuppressants is an effective and safe regimen for adult patients diagnosed with HBV-GN. Low-dose steroid is effective and can be recommended.
COMMENTS
Background
Hepatitis B virus-associated glomerulonephritis (HBV-GN) is one of the most common secondary glomerular diseases in developing countries such as China. To clear the viral antigen and abrogate the proteinuria is crucial for liver and renal function preservation and for decreasing the morbidity and mortality of this disease.
Research frontiers
HBV-GN treatment includes antiviral drugs, e.g., interferon and lamivudine, or immunosuppressants, e.g., glucocorticosteroids and mycophenolate mofetil. Although antivirals have been proven to be effective in clearing the viral antigens and attenuating the proteinuria, the safety and efficacy of immunosuppressants are still controversial.
Innovations and breakthroughs
A recent meta-analysis study showed that treatment of HBV-GN with corticosteroids only was not effective in proteinuria remission. However, this conclusion was drawn by analysis of data from both adult and pediatric patients, and because spontaneous remission can occur in children, this could have confounded the effectiveness of corticosteroid treatment in adult patients. To date, the current meta-analysis is the first to study the efficacy and safety of combined therapy with antivirals and immunosuppressants in adult HBV-GN patients.
Applications
The results of this meta-analysis should be beneficial for investigators and clinicians for obtaining information for the therapy of HBV-GN. Antivirals combined with immunosuppressants are effective and safe for adult patients and low-dose steroid can be recommended. All of the evidence in this paper supports the use of immunosuppressants which are being empirically used in the Asia-Pacific regions.
Terminology
HBV-GN is a clinical entity in which viral antigen and immune complexes have been identified in kidney, indicating that the pathogenesis of this disease may be associated with immune reaction. HBV-GN can be mainly separated into membranous glomerulonephritis, mesangial proliferative glomerulonephritis and membranoproliferative glomerulonephritis subgroups.
Peer review
This paper has major clinical implications and may change clinical policy.
Footnotes
Supported by National Natural Science Foundation, No. 81072914; Major Project Foundation of National Science and Technology, No. 2010ZX9102-204; Traditional Chinese Medicine Research Grant for Military Organization, No. 10ZYZ255
Peer reviewers: Assy Nimer, MD, Assistant Professor, Liver Unit, Ziv Medical Centre, BOX 1008, Safed 13100, Israel; Filip Braet, Associate Professor, Australian Key Centre for Microscopy and Microanalysis, Madsen Building (F09), The University of Sydney, Sydney NSW 2006, Australia
S- Editor Tian L L- Editor Logan S E- Editor Zhang DN
References
- 1.Zhiqiang G, Zhaohui D, Qinhuan W, Dexian C, Yunyun F, Hongtao L, Iloeje UH. Cost of chronic hepatitis B infection in China. J Clin Gastroenterol. 2004;38:S175–S178. doi: 10.1097/00004836-200411003-00010. [DOI] [PubMed] [Google Scholar]
- 2.Bhimma R, Coovadia HM. Hepatitis B virus-associated nephropathy. Am J Nephrol. 2004;24:198–211. doi: 10.1159/000077065. [DOI] [PubMed] [Google Scholar]
- 3.Lai KN, Li PK, Lui SF, Au TC, Tam JS, Tong KL, Lai FM. Membranous nephropathy related to hepatitis B virus in adults. N Engl J Med. 1991;324:1457–1463. doi: 10.1056/NEJM199105233242103. [DOI] [PubMed] [Google Scholar]
- 4.Fabrizi F, Dixit V, Martin P. Meta-analysis: anti-viral therapy of hepatitis B virus-associated glomerulonephritis. Aliment Pharmacol Ther. 2006;24:781–788. doi: 10.1111/j.1365-2036.2006.03041.x. [DOI] [PubMed] [Google Scholar]
- 5.Lai KN, Tam JS, Lin HJ, Lai FM. The therapeutic dilemma of the usage of corticosteroid in patients with membranous nephropathy and persistent hepatitis B virus surface antigenaemia. Nephron. 1990;54:12–17. doi: 10.1159/000185802. [DOI] [PubMed] [Google Scholar]
- 6.Taskapan H, Oymak O, Dogukan A, Ozbakir O, Utas C. Transformation of hepatitis B virus-related membranous glomerulonephritis to crescentic form. Clin Nephrol. 2000;54:161–163. [PubMed] [Google Scholar]
- 7.Lai FM, Tam JS, Li PK, Lai KN. Replication of hepatitis B virus with corticosteroid therapy in hepatitis B virus related membranous nephropathy. Virchows Arch A Pathol Anat Histopathol. 1989;414:279–284. doi: 10.1007/BF00822033. [DOI] [PubMed] [Google Scholar]
- 8.Zhang Y, Zhou JH, Yin XL, Wang FY. Treatment of hepatitis B virus-associated glomerulonephritis: a meta-analysis. World J Gastroenterol. 2010;16:770–777. doi: 10.3748/wjg.v16.i6.770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fang YQ, Wu P, Li Y, Mao LC, Hu YQ, Tang XL. Antivirus combined with immunosuppressive therapy hepatitis B virus-associated membranous glomerulonephritis those with HBsAg positive and HBV replication. CJITWN. 2009;10:784–787. [Google Scholar]
- 10.Panomsak S, Lewsuwan S, Eiam-Ong S, Kanjanabuch T. Hepatitis-B virus-associated nephropathies in adults: a clinical study in Thailand. J Med Assoc Thai. 2006;89 Suppl 2:S151–S156. [PubMed] [Google Scholar]
- 11.Wang HY. Diagnosis, mechanism and treatment of hepatitis B virus associated glomerulonephritis. Shijie Yixue Zazhi. 2002;6:28–31. [Google Scholar]
- 12.Li X, Tian J, Wu J, He Q, Li H, Han F, Li Q, Chen Y, Ni Q, Chen J. A comparison of a standard-dose prednisone regimen and mycophenolate mofetil combined with a lower prednisone dose in Chinese adults with idiopathic nephrotic syndrome who were carriers of hepatitis B surface antigen: a prospective cohort study. Clin Ther. 2009;31:741–750. doi: 10.1016/j.clinthera.2009.04.011. [DOI] [PubMed] [Google Scholar]
- 13.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–188. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 14.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–1101. [PubMed] [Google Scholar]
- 16.Cheng CL, Lou TQ, Zheng ZD, Shi CG, Liu X. Mycophenolate mofetil combined with steroid hormone and lamivudine on the treatment of hepatitis B virus associated glomerulonephritis. Zhongguo Shiyong Neike Zazhi. 2005;25:1083–1085. [Google Scholar]
- 17.Dang YM, Jiang LN, Li GP, Hu JQ, Zhao XR. Efficacy of Mycophenolate mofetil on hepatitis B virus associated nephritis. J Clin Nephrol. 2004;4:270–271. [Google Scholar]
- 18.He LS, Shen YP. Clinical investigation of combined treatment of mycophenolate mofetil and corticosteroid for membranous nephropathy. J Clin Nephrol. 2007;7:1–4. [Google Scholar]
- 19.Liu J, Xin KM, Wang XT, Wang Y. The application of Bailing capsule combined with MMF, prednisone and lamivudine on hepatitis B virus associated nephritis. Chin Tradit Patent Med. 2010;32:1480–1482. [Google Scholar]
- 20.Liu ZH, Yuan F. Entecavir combined steroid therapy of clinical manifestations of nephrotic syndrome in HBV-GN. J Clin Res. 2008;25:2264–2266. [Google Scholar]
- 21.Sun LL, Wu J, Xu CG, Zhang LM, Zhang YQ, Mei CL. Clinical Study of Mycophenolate Mofetil and Lamivudine in the Treatment of Hepatitis B Virus Associated Nephritis. CJITWN. 2005;6:584–587. [Google Scholar]
- 22.Sun XP, Yang Q, Cao XG. Adefovir Dipivoxil combined Sugar Corticosteroid Treated 29 Cases of Hepatitis B Virus Associated Glomerulonephritis. Zhongguo Yiyao Zhinan. 2010;8:8–11. [Google Scholar]
- 23.Tang L, Chen XM, Zhao W, Cui Y. A randomized controlled trial of mycophenolate mofetil treatment in HBV-associated glomerulonephritis. Beijing Yixue. 2005;27:166–169. [Google Scholar]
- 24.Tang Y, Lou TQ, Cheng CL, Wang C, Shi CG, Deng B. Treatment of hepatitis B virus associated glomerulonephritis according to different pathology patterns. Zhongguo Xiandai Yixue Zazhi. 2005;15:869–872. [Google Scholar]
- 25.Wu SB, Wang YD, Xu Y. Study of mycophenolate mofetil and lamivudine in treatment of hepatitis B virus associated glomerulonephritis. Xiandai Zhongxiyi Jiehe Zazhi. 2008;17:4674–4676. [Google Scholar]
- 26.Xia DQ, Cai SF, Yang HR, Sun XP, Wu WB. Clinical analysis of Hepatitis B associated glomerulonephritis (HBV-GN) and intervention effect of lamivudine combined with leflunomide and prednisone. Zhongguo Yixue Chuangxin. 2009;6:6–8. [Google Scholar]
- 27.Tang S, Lai FM, Lui YH, Tang CS, Kung NN, Ho YW, Chan KW, Leung JC, Lai KN. Lamivudine in hepatitis B-associated membranous nephropathy. Kidney Int. 2005;68:1750–1758. doi: 10.1111/j.1523-1755.2005.00591.x. [DOI] [PubMed] [Google Scholar]
- 28.Kusakabe A, Tanaka Y, Kurbanov F, Goto K, Tajiri H, Murakami J, Okuse C, Yotsuyanagi H, Joh T, Mizokami M. Virological features of hepatitis B virus-associated nephropathy in Japan. J Med Virol. 2007;79:1305–1311. doi: 10.1002/jmv.20941. [DOI] [PubMed] [Google Scholar]
- 29.Izzedine H, Massard J, Poynard T, Deray G. Lamivudine and HBV-associated nephropathy. Nephrol Dial Transplant. 2006;21:828–829. doi: 10.1093/ndt/gfi239. [DOI] [PubMed] [Google Scholar]
- 30.Gonzalo A, Mampaso F, Bárcena R, Gallego N, Ortuño J. Membranous nephropathy associated with hepatitis B virus infection: long-term clinical and histological outcome. Nephrol Dial Transplant. 1999;14:416–418. doi: 10.1093/ndt/14.2.416. [DOI] [PubMed] [Google Scholar]
- 31.Connor FL, Rosenberg AR, Kennedy SE, Bohane TD. HBV associated nephrotic syndrome: resolution with oral lamivudine. Arch Dis Child. 2003;88:446–449. doi: 10.1136/adc.88.5.446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Du J, Ding GH. Diagnosis and treatment of hepatitis B virus associated glomerulonephritis. J Clin Intern Med. 2010;27:588–589. [Google Scholar]
- 33.Kanaan N, Horsmans Y, Goffin E. Lamivudine for nephrotic syndrome related to hepatitis B virus (HBV) infection. Clin Nephrol. 2006;65:208–210. doi: 10.5414/cnp65208. [DOI] [PubMed] [Google Scholar]
- 34.Okuse C, Yotsuyanagi H, Yamada N, Ikeda H, Takahashi H, Suzuki M, Kondo S, Kimura K, Koike J, Itoh F. Successful treatment of hepatitis B virus-associated membranous nephropathy with lamivudine. Clin Nephrol. 2006;65:53–56. doi: 10.5414/cnp65053. [DOI] [PubMed] [Google Scholar]
- 35.Wen YK, Chen ML. Remission of hepatitis B virus-associated membranoproliferative glomerulonephritis in a cirrhotic patient after lamivudine therapy. Clin Nephrol. 2006;65:211–215. doi: 10.5414/cnp65211. [DOI] [PubMed] [Google Scholar]
- 36.Leung N. Treatment of HBeAg-positive chronic hepatitis B with nucleos(t)ide analogues. Liver Int. 2011;31 Suppl 1:85–89. doi: 10.1111/j.1478-3231.2010.02387.x. [DOI] [PubMed] [Google Scholar]
- 37.Zoulim F. Hepatitis B virus resistance to antiviral drugs: where are we going? Liver Int. 2011;31 Suppl 1:111–116. doi: 10.1111/j.1478-3231.2010.02399.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Cui TG. The problem worthy of attention in the treatment of hepatitis B virus associated glomerulonephritis. J Clin Nephrol. 2009;9:103–105. [Google Scholar]
- 39.Levy M, Gagnadoux MF. Membranous nephropathy following perinatal transmission of hepatitis B virus infection--long-term follow-up study. Pediatr Nephrol. 1996;10:76–78. doi: 10.1007/BF00863453. [DOI] [PubMed] [Google Scholar]
- 40.Yang PM, Sung JL, Chen DS. HLA-A, B, C and DR antigens in chronic hepatitis B viral infection. Hepatogastroenterology. 1989;36:363–366. [PubMed] [Google Scholar]
- 41.Liaw YF, Leung N, Kao JH, Piratvisuth T, Gane E, Han KH, Guan R, Lau GK, Locarnini S. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int. 2008;2:263–283. doi: 10.1007/s12072-008-9080-3. [DOI] [PMC free article] [PubMed] [Google Scholar]