

Abstract
Background
this study investigated the phagocytic function of peripheral granulocytes and monocytes from adult individuals with Down syndrome (DS) and assessed the relation between phagocytic function and periodontal status.
Methods
55 DS individuals (18–56 years old), 74 mentally retarded (MR) individuals and 88 medically healthy controls (HC) participated in the study. Gingival inflammation index, plaque index, probing depth, periodontal attachment level (AL) and bleeding on probing were taken for each subject. Whole blood was collected for granulocyte/monocyte phagocytosis tests. Phagocytic function was determined by flow cytometry in terms of percentage of cells actively involved in phagocytosis, and phagocytic intensity (magnitude of the bacterial staining per cell).
Results
phagocytic intensity of both granulocytes and monocytes was comparable in HC and DS subjects. While AL was directly related to phagocytic intensity of both granulocytes (r=0.14, p=0.03) and monocytes (r=0.2, p=0.003) in all subjects, this relationship was stronger in DS than other subjects, even after controlling for known risk factors for periodontitis (p<0.05). Monocyte phagocytic intensity was the only necessary predictor of AL (p=0.003), indicating a similar relationship between AL and phagocytic activity in either cell type.
Conclusions
While granulocyte and monocyte phagocytic intensities are similar in Down and non-DS individuals, phagocytic intensity was associated with more AL in DS than non-DS individuals.
Keywords: Down syndrome, periodontitis, granulocytes, monocytes, phagocytosis
Introduction
Down syndrome (DS) is the most common of all genetic disorders with incidence estimated at 1 per 800 births (Sherman et al., 2007, Shin et al., 2009). It is characterized by the presence of an extra copy of the 21st chromosome. The most common manifestations of the syndrome include characteristic physical appearance and varied mental and physical disorders (Megarbane et al., 2009). Several physical disorders described in DS individuals include congenital heart disease, thyroid dysfunction, Alzheimer disease and alteration of the immune system including granulocyte/monocyte cell dysfunction (Bloemers et al., 2010, Kusters et al., 2009, Megarbane et al., 2009).
Periodontal disease is highly prevalent among DS individuals (Sakellari et al., 2005, Reuland-Bosma & van Dijk, 1986). Among the factors that may contribute to periodontal disease in DS individuals are impairments in phagocytic cell function (Novo et al., 1993, Rascon Trincado et al., 1988, Wysocki et al., 1987). Granulocytes (polymorphonuclear leukocytes, PMNs) and monocytes play an important role in the defense against microbial plaque and in the pathogenesis of periodontitis (Buchmann et al., 2002, Figueredo et al., 2005, Gronert et al., 2004, Johnstone et al., 2007, Page, 1991). Only a few studies have examined the relation between phagocytic cell function and periodontal disease in DS individuals (Izumi et al., 1989, Reuland-Bosma et al., 1988, Sreedevi & Munshi, 1998, Yavuzyilmaz et al., 1993). These studies focused mainly on granulocyte chemotaxis in DS children with gingivitis. Almost no data exist regarding granulocyte/monocyte phagocytic function and periodontitis in DS individuals.
We hypothesized that functional impairment of the peripheral blood phagocytic cells of DS individuals may increase their susceptibility to periodontal disease. Thus, the aims of this study were to investigate phagocytic function of both granulocytes and monocytes from adult individuals with DS and non-DS, and to determine if deficits in these functions are associated with periodontitis.
Materials and Methods
Subject recruitment and clinical evaluations were previously described (Khocht et al., 2010).
Study sites
The study was done in cooperation with the Georgia Department of Human Resources (GRH)/Georgia Regional Hospitals in Atlanta, Savannah and Augusta. The study protocol and consent forms were approved by the Georgia Regional Hospital Institutional Review Board and the Georgia Health Sciences University Human Assurance Committee. The study included three subject groups, Down Syndrome group (DS), mental retardation (disability) non-Down group (MR) and a mentally normal control group (HC). Both the DS and MR subjects were recruited from the GRH healthcare systems in Atlanta, Savannah and Augusta, Georgia. All DS and MR subjects were patients of record at the three hospital locations; some were institutionalized while others were outpatients living in group-homes or with their families. All DS and MR subjects were receiving periodic dental care at one of the three GRH locations.
Inclusion criteria
The study inclusion criteria implemented for DS subjects were: confirmed diagnosis of Trisomy 21, receiving periodic dental care, age 18 years or older, a minimum of 10 teeth present, no other medical conditions known to affect periodontal status (e.g. diabetes mellitus), no antibiotic treatment in the past 3 months prior to entry in the study, no history of cigarette smoking and being able to cooperate with the study examiners. Study inclusion criteria for the MR subjects were similar to the DS subjects except for a confirmed diagnosis of mental retardation without Trisomy 21. Study inclusion criteria for the HC subjects were also similar to the DS subjects except for absence of mental retardation.
Subject recruitment
The attending dentist in charge of the dental clinic at each of the three GRH sites reviewed the available records and identified dentulous DS patients who would meet the study criteria and would be able to participate in a dental examination. Then MR patients matched to the previously identified DS patients on age, race and gender were identified from the same hospital records. The matched MR patients were selected based on their ability to cooperate and sit for the dental examination without need for sedation. Their mental retardation was secondary to head trauma at birth. The HC subjects were recruited from the general population living in the vicinity of the GRH locations used. All HC subjects were under care of private dentists and they also were matched on gender, race and age to the DS subjects.
Subject screening and enrollment
A total of 289 subjects were screened for the study, 26 were disqualified for medical reasons, 46 completed portions of the study evaluations and were not able to return to complete the remaining portions, and 217 completed most of the study evaluations. This report will focus on the 217 subjects who completed most of the study evaluations, including immunological testing. None of the subjects smoked cigarettes, had diabetes, or was on a medication known to influence periodontal status.
Ethical issues
The GRH dentist contacted the family or caretaker of each potential DS or MR subject, explained the study protocol and obtained their consent to enroll the subject in the study. All subjects (including DS and MR) signed the consent form.
Oral/periodontal Assessments
As previously described (Khocht et al., 2010), two experienced dental hygienists blinded to the objectives of the study performed all exams. The examiners were calibrated and standardized in the use of the clinical evaluation measures employed in the study (Khocht et al., 2010). The examiners enumerated missing teeth and teeth with carious lesions then recorded the Loe and Silness gingival index (GI) (Loe, 1967), the Quigley Hein plaque index (Quigley & Hein, 1962), probing depth (PD), clinical periodontal attachment levels (AL) and bleeding on probing (BOP) on six sites per tooth. Third molars were excluded. Periodontitis was defined as present when 5% or higher of teeth scored exhibited attachment loss =>5 mm.
Blood sampling
Whole blood was collected from the subjects for granulocyte/monocyte phagocytosis and other tests. All blood draws were done in the morning. A heparinized tube of blood was drawn, and immediately placed in a cooler box for transportation to the laboratory. Upon arrival at the laboratory, samples were stored at room temperature for processing the following morning. All samples were processed within a range of 16–20 hours from collection. An EDTA blood sample was also collected and processed for complete blood cell count and differential.
Phagocytosis Tests
The test for phagocytosis was carried out by using the Phagotest kit (Orpegen, Heidelberg, Germany). This flow cytometry-based method quantifies phagocytosis of fluorescently-labeled bacteria in terms of the percentage of phagocytically-active cells (ingestion of at least one bacteria) as well as individual cell phagocytic intensity (total fluorescence intensity per cell). One hundred microliters of heparinized whole blood was added to two test tubes (sample and control). The whole blood was mixed with 20 μl of precooled opsonized fluorescein (FITC)-labeled E coli, resulting in a bacteria/leukocyte ratio of ~25:1. Both tubes were gently vortexed and the control tube was incubated on ice and the sample was incubated at 37°C in a water bath for 10 min. At the end of the incubation period, the sample tubes were removed from the water bath and placed on ice to stop phagocytosis. Both the control and sample were quenched with cold quenching solution and then washed with washing solutions two times. The samples were then lysed, fixed and incubated for an additional 20 minutes at room temperature. The cells were then washed and a DNA staining solution (propidium iodide) was added. The cells with staining solution were incubated for 10 minutes and then analyzed by flow cytometry.
Flow cytometry
Between 10,000 and 15,000 leukocytes were collected from each sample on a FACSCalibur (Beckton Dickinson) flow cytometer. The instrument was calibrated and standardized by using Calibrite beads (Becton Dickinson, Erembodegen- Aalst, Belgium). All sample analyses were performed with Cellquest software (Becton Dickinson). The granulocyte and monocyte populations were gated by using their forward- and side-scatter dot plots (Figure 1). During fluorescence-activated cell sorter analysis, free bacteria and aggregates of bacteria were separated from leukocytes based on their much lower DNA content compared to that of eukaryotic cells. Phagocytosis was monitored by determining both the proportion of cells fluorescing and the relative fluorescence intensities (RFI) of the gated granulocytes (Figure 2).
Figure 1.
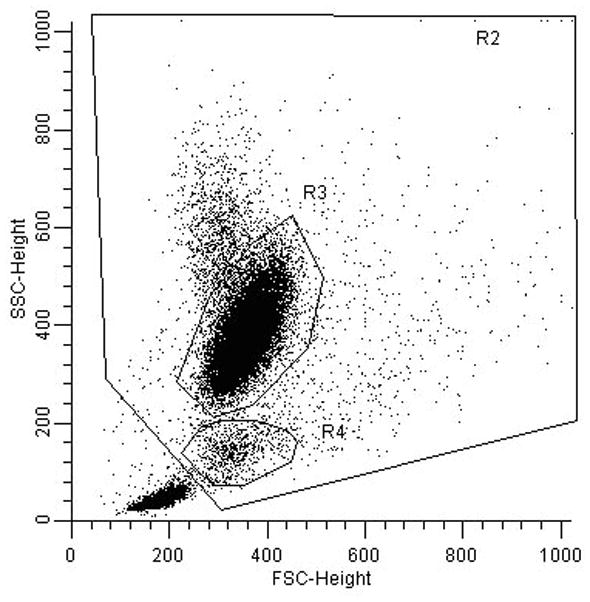
Discrimination of white blood cell populations based on forward scatter vs. side scatter. The R3 gate is the neutrophil population. The R4 gate is the monocyte population.
Figure 2.
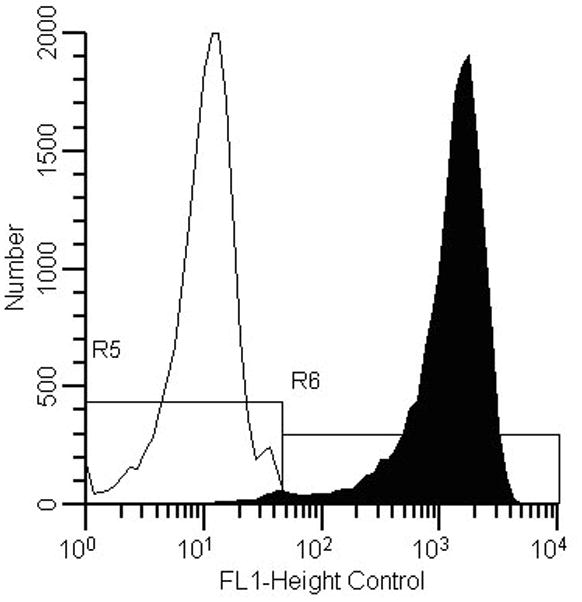
Fluorescent intensity distribution curve of the control incubated at 0°C (left curve, R5) and the phagocytically active sample incubated at 37°C (right curve, R6).
Statistical analysis
Analysis of variance (ANOVA) or chi-square test was used for means or proportions respectively to examine the differences between the three groups on demographics, clinical data, white cell counts and granulocyte/monocyte phagocytic activity. Tukey HSD (Honestly Significant Difference) test was used for post hoc mean comparisons. Pearson correlation analysis was used to examine the associations between phagocytic cell function measures and periodontal measures. Multiple regression analysis was used to examine the association between phagocytic cell function and periodontal measures while controlling for known demographic risk factors for periodontitis.
Results
Demographic and clinical data of the entire subject population was previously reported (Khocht et al., 2010). Demographic, clinical and white blood cell count data of the subset of subjects included in this report are summarized in Table 1. All three groups were matched on race and gender. ANOVA showed differences between the three groups on age (p=0.0001) and institution living (p=0.001). Follow-up analysis with Tukey HSD test showed that the MR group was older than the DS and HC groups (p = 0.05) and number of institutionalized subjects in the MR group was higher than the DS group (p=0.05). Clinically, the percentage of subjects with periodontitis (as defined previously) was similarly distributed among the three groups, DS 72%, HC 71% and MR 79%. ANOVA showed significant differences between the three groups on all clinical parameters (p<0.001). Follow-up analysis with Tukey HSD showed that subjects in both DS and MR groups had higher levels of GI (p = 0.05), PI (p = 0.05), BOP (p = 0.05) and missing teeth (p = 0.05) than the HC group. The DS subjects showed greater loss of clinical periodontal attachment than HC and MR subjects (p = 0.05). ANOVA also showed no differences in the counts of total white blood cells and granulocytes between the three groups, however monocyte counts differed (p=0.03). Follow-up analysis with Tukey HSD showed that MR subjects evidenced higher counts of monocytes than HC subjects (p = 0.03).
Table 1.
summary of demographic, clinical and white cell count data of the subset of subjects with immunological data presented in this report.
| Variable | HC N = 88 |
DS N = 55 |
MR N = 74 |
p-value |
|---|---|---|---|---|
| Demographics: | ||||
| Age | 40.79 (1.28) | 36.18 (1.63) | 45.87 (1.40) | 0.0001* |
| White Percent | 70.45% | 78.18% | 81.08% | 0.26 |
| Male Percent | 42.05% | 52.73% | 58.11% | 0.11 |
| Institution | NA | 41.82% | 82.43% | 0.001** |
| Clinical: | ||||
| Plaque Index | 1.25 (0.08) | 1.56 (0.01) | 1.78 (0.08) | 0.0001# |
| Gingival Index | 0.68 (0.03) | 0.92 (0.04) | 1 (0.03) | 0.0001# |
| Bleeding on probing | 24.81 (2.98) | 40.60 (3.78) | 43.79 (3.25) | 0.0001# |
| Attachment Level | 2.24 (0.08) | 2.70 (0.10) | 2.24 (0.08) | 0.0006¶ |
| Missing teeth | 1.80 (0.41) | 4.61 (0.52) | 4.56 (0.45) | 0.0001# |
| Cell Counts: | ||||
| WBC | 6.3 (0.19) | 5.7 (0.24) | 6.3 (0.20) | 0.12 |
| % Granulocytes | 56.9 (1.08) | 58.5 (1.36) | 57.5 (1.18) | 0.65 |
| % Monocytes | 8.6 (0.31) | 9.4 (0.39) | 9.8 (0.34) | 0.03§ |
Data presented as mean (SE) or percentage. P-value gives the probability that the groups differ in either an ANOVA test or chi-square test for means or proportions respectively.
MR>DS and HC;
MR>DS;
HC<MR and DS;
DS> MR and HC;
MR>HC.
Demographic and clinical data of entire subject population were previously reported (Khocht et al., 2010).
ANOVA showed significant differences between the three groups on the percentage of phagocytically-active granulocytes (p=0.001). Follow-up analysis with the Tukey HSD test showed the MR group had significantly lower percentages of phagocytically-active granulocytes than the HC and DS groups (p=0.05) (Figure 3A). ANOVA also showed significant differences between the three groups for phagocytic intensity per granulocytes (p=0.005). Follow-up analysis with the Tukey HSD test also showed that granulocytes from the MR group had significantly less phagocytic intensity than granulocytes from the HC and DS groups (p=0.05) (Figure 3B).
Figure 3.

Phagocytic characteristics of granulocytes (PMN). The left panel (A) illustrates the percentage of granulocytes engaged in phagocytosis. The right panel (B) illustrates the phagocytic intensity per granulocyte (RFI). ‡: MR < HC and DS, P < 0.001; †: MR < HC and DS, P = 0.005.
ANOVA showed significant differences between the three groups on the percentage of phagocytically-active monocytes (p=0.02). Follow-up analysis with the Tukey HSD test showed the HC group to have a significantly higher percentage than the MR and DS groups (p=0.05) (Figure 4A). ANOVA also showed significant differences between the three groups on the phagocytic intensity of monocytes (p=0.001). Follow-up analysis with the Tukey HSD test showed that monocytes from the MR group had significantly less phagocytic intensity than monocytes from the HC and DS groups (p=0.05) (Figure 4B). Thus even though the percentage of phagocytically-active monocytes was diminished in DS individuals, their phagocytic intensity was undiminished.
Figure 4.

Phagocytic characteristics of monocytes. The left panel (A) illustrates the percentage of monocytes engaged in phagocytosis. The right panel (B) illustrates the phagocytic intensity per monocyte (RFI). *: DS and MR < HC, P < 0.02; †: MR < DS only, P < 0.001.
Analysis of covariance controlling for age, gender and race confirmed the univariate comparisons of phagocytic cell functions between groups.
Pearson correlation analysis investigating the association between phagocytic function measures and periodontal measures in all subjects combined showed weak albeit significant associations between AL with percentage of phagocytically-active granulocytes (r=0.17, p =0.01), with phagocytic intensity of granulocytes (r=0.14, p=0.03) and with phagocytic intensity of monocytes (r=0.2, p=0.003).
Stepwise regression analysis indicated that monocyte phagocytic intensity was the only necessary predictor of AL (p=0.003) in all subjects combined. No associations were noted between phagocytic function measures and other periodontal measures (GI, BOP and PI).
The association between monocyte phagocytic intensity and AL was further investigated in a sequential series of regression models (table 2). In model (1) risk factors for periodontitis (age, gender, race and plaque levels) were introduced and the analysis upheld the association between monocyte phagocytic intensity and AL (beta-weight = 0.20, p<0.05). In model (2) MR and DS status were added to the model to investigate their association with AL. Introducing DS and MR into the model slightly lowered the strength of association between AL and monocyte phagocytic intensity (beta-weight = 0.13, p<0.05). It also showed that DS status was independently associated with AL (beta-weight = 0.32. p<0.05), however MR showed no association with AL. Model 3 attempted to investigate if the association between AL and monocyte phagocytic intensity differed between DS and non-DS subjects by introducing a DS-monocyte phagocytic intensity interaction. The interaction was significant (beta-weight=0.23, p<0.05) and showed that the association between monocyte phagocytic intensity and AL is stronger in Down individuals than non-Down individuals.
Table 2.
Linear regression models relating AL to monocyte phagocytosis while controlling for demographic variables, DS status, MR status and the interaction of DS with monocyte phagocytic intensity. Data presented as beta weights.
| Model 1 N=217 |
Model 2 N=217 |
Model 3 N=217 |
|
|---|---|---|---|
| Monocyte phagocytic intensity | 0.20** | 0.13* | 0.31** |
| Age | 0.25** | 0.33** | 0.32** |
| Sex (male=1, female=0) | 0.18** | 0.18** | 0.20** |
| Race (non-white=1, white=0) | 0.16** | 0.18** | 0.20** |
| Plaque levels | −0.07 | −0.08 | −0.07 |
| DS (yes=1, no=0) | 0.32** | 0.25** | |
| MR (yes=1, no=0) | 0.01 | 0.02 | |
| DS* Monocyte phagocytic intensity | 0.23** | ||
| R square | 0.14 | 0.23 | 0.26 |
p < 0.01
p < 0.05
Discussion
Results from this study showed that in DS individuals both granulocyte and monocyte phagocytic intensities were undiminished, although the percentage of monocytes actively involved in phagocytosis was significantly less than that for controls. In all subjects phagocytic intensity of both granulocytes and monocytes significantly associated with loss of periodontal attachment. In all subjects monocyte phagocytic intensity was a stronger predictor of AL than granulocyte phagocytic activity and the association was stronger in DS individuals than non-DS individuals.
Granulocytes involved in periodontal infections tend to accumulate outside of the periodontal tissues in proximity to the microbial plaque in the dentogingival region (Iacono et al., 1985). Thus the damaging byproducts they release in association with their phagocytic activity may minimally affect the deeper structures of the periodontium. On the other hand, monocytes tend to infiltrate inflamed gingival tissues as tissue macrophages and play various important roles including phagocytosis of cellular debris and pathogens, production of oxygen radicals, production of inflammatory cytokines and tissue degrading enzymes (Berglundh & Donati, 2005, Pussinen et al., 2004, Younes et al., 2009, Page, 1991). Thus due to their deeper location inside the periodontal tissues and their multiple damaging products their activity may inflect greater damage on the periodontium. This may explain why monocyte phagocytic intensity is a more reliable predictor of AL than granulocyte phagocytic intensity.
Why the relation between monocyte phagocytic intensity and AL is stronger in DS individuals than non-DS individuals may be related to a gene dose effect associated with trisomy of chromosome 21. Chromosome 21 encodes several proteins that are associated with production of oxygen radicals such as nicotinamide adenine dinucleotide phosphate (NADPH) and superoxide dismutase (SOD) (Akinci et al., 2010, Lemieux et al., 1993, Strydom et al., 2009). Increased amounts of these products would lead to oxidative stress. The resulting reactive oxygen species (ROS) would enhance tissue damage and inflammation. Thus the extra chromosome 21 in monocytes of DS individuals would result in greater periodontal tissue loss.
Previous studies investigating phagocytic cell function in relation to periodontal disease in DS individuals mainly focused on chemotactic activity of granulocytes (Izumi et al., 1989, Reuland-Bosma et al., 1988, Sreedevi & Munshi, 1998). All studies agreed that DS individuals show diminished granulocyte chemotactic activity. Thus granulocytes in DS individuals may fail to reach the dentogingival region and form a barrier between microbial plaque and the periodontium leaving the macrophages within the gingival tissues to provide the primary defense against the infection. Gingival tissue macrophages are predominantly present in inflamed gingival tissues obtained from DS individuals (Sohoel et al., 1992). They seem to be active in immune interactions and expression of HLA Class II antigens (Sohoel et al., 1995). Their predominant presence and activity within the gingival tissues of DS individuals may further explain why their phagocytic activity is more strongly associated with AL in DS individuals than non-DS individuals.
In conclusion the findings from this study suggest that in DS individuals periodontal tissue damage is partially associated with host microbial interactions involving phagocytosis. Reducing microbial load would minimize host-microbial interactions and decrease the potential of periodontal tissue damage in this susceptible group.
Acknowledgments
This study was supported by the National Institute of Dental and Craniofacial Research, Bethesda, Maryland (NIDCR: DE15012-02). There are no perceived or actual conflicts of interest to be reported.
References
- Akinci O, Mihci E, Tacoy S, Kardelen F, Keser I, Aslan M. Neutrophil oxidative metabolism in Down syndrome patients with congenital heart defects. Environmental & Molecular Mutagenesis. 2010;51:57–63. doi: 10.1002/em.20511. [DOI] [PubMed] [Google Scholar]
- Berglundh T, Donati M. Aspects of adaptive host response in periodontitis. [Review] [83 refs] J Clin Periodontol. 2005;6:87–107. doi: 10.1111/j.1600-051X.2005.00820.x. [DOI] [PubMed] [Google Scholar]
- Bloemers BL, van Bleek GM, Kimpen JL, Bont L. Distinct abnormalities in the innate immune system of children with Down syndrome. Journal of Pediatrics. 2010;156:804–9. doi: 10.1016/j.jpeds.2009.12.006. [DOI] [PubMed] [Google Scholar]
- Buchmann R, Hasilik A, Nunn ME, Van Dyke TE, Lange DE. PMN responses in chronic periodontal disease: evaluation by gingival crevicular fluid enzymes and elastase-alpha-1-proteinase inhibitor complex. J Clin Periodontol. 2002;29:563–72. doi: 10.1034/j.1600-051x.2002.290613.x. [DOI] [PubMed] [Google Scholar]
- Figueredo CMS, Fischer RG, Gustafsson A. Aberrant neutrophil reactions in periodontitis. J Periodontol. 2005;76:951–5. doi: 10.1902/jop.2005.76.6.951. [DOI] [PubMed] [Google Scholar]
- Gronert K, Kantarci A, Levy BD, Clish CB, Odparlik S, Hasturk H, Badwey JA, Colgan SP, Van Dyke TE, Serhan CN. A molecular defect in intracellular lipid signaling in human neutrophils in localized aggressive periodontal tissue damage. J Immunol. 2004;172:1856–61. doi: 10.4049/jimmunol.172.3.1856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iacono VJ, Singh S, Golub LM, Ramamurthy NS, Kaslick R. In vivo assay of crevicular leukocyte migration. Its development and potential applications. J Periodontol. 1985;56:56–62. doi: 10.1902/jop.1985.56.11s.56. [DOI] [PubMed] [Google Scholar]
- Izumi Y, Sugiyama S, Shinozuka O, Yamazaki T, Ohyama T, Ishikawa I. Defective neutrophil chemotaxis in Down’s syndrome patients and its relationship to periodontal destruction. J Periodontol. 1989;60:238–42. doi: 10.1902/jop.1989.60.5.238. [DOI] [PubMed] [Google Scholar]
- Johnstone AM, Koh A, Goldberg MB, Glogauer M. A hyperactive neutrophil phenotype in patients with refractory periodontitis. J Periodontol. 2007;78:1788–94. doi: 10.1902/jop.2007.070107. [DOI] [PubMed] [Google Scholar]
- Khocht A, Janal M, Turner B. Periodontal health in Down syndrome: contributions of mental challenge, personal and professional dental care. Spec Care Dentist. 2010;30:118–123. doi: 10.1111/j.1754-4505.2010.00134.x. [DOI] [PubMed] [Google Scholar]
- Kusters MA, Verstegen RH, Gemen EF, de Vries E. Intrinsic defect of the immune system in children with Down syndrome: a review. [Review] [74 refs] Clin Exp Immunol. 2009;156:189–93. doi: 10.1111/j.1365-2249.2009.03890.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lemieux N, Malfoy B, Forrest GL. Human carbonyl reductase (CBR) localized to band 21q22.1 by high-resolution fluorescence in situ hybridization displays gene dosage effects in trisomy 21 cells. Genomics. 1993;15:169–72. doi: 10.1006/geno.1993.1024. [DOI] [PubMed] [Google Scholar]
- Loe H. The Gingival Index, the Plaque Index and the Retention Index Systems. J Periodontol. 1967;38(Suppl):610–6. doi: 10.1902/jop.1967.38.6.610. [DOI] [PubMed] [Google Scholar]
- Megarbane A, Ravel A, Mircher C, Sturtz F, Grattau Y, Rethore MO, Delabar JM, Mobley WC. The 50th anniversary of the discovery of trisomy 21: the past, present, and future of research and treatment of Down syndrome. [Review] [58 refs] Genetics in Medicine. 2009;11:611–6. doi: 10.1097/GIM.0b013e3181b2e34c. [DOI] [PubMed] [Google Scholar]
- Novo E, Garcia MI, Lavergne J. Nonspecific immunity in Down syndrome: a study of chemotaxis, phagocytosis, oxidative metabolism, and cell surface marker expression of polymorphonuclear cells. Am J Med Genet. 1993;46:384–91. doi: 10.1002/ajmg.1320460408. [DOI] [PubMed] [Google Scholar]
- Page RC. The role of inflammatory mediators in the pathogenesis of periodontal disease. J Periodontal Res. 1991;26:230–42. doi: 10.1111/j.1600-0765.1991.tb01649.x. [DOI] [PubMed] [Google Scholar]
- Pussinen PJ, Vilkuna-Rautiainen T, Alfthan G, Palosuo T, Jauhiainen M, Sundvall J, Vesanen M, Mattila K, Asikainen S. Severe periodontitis enhances macrophage activation via increased serum lipopolysaccharide. Arteriosclerosis, Thrombosis & Vascular Biology. 2004;24:2174–80. doi: 10.1161/01.ATV.0000145979.82184.9f. [DOI] [PubMed] [Google Scholar]
- Quigley GA, Hein JW. Comparative cleansing efficiency of manual and power brushing. J Am Dent Assoc. 1962;65:26–9. doi: 10.14219/jada.archive.1962.0184. [DOI] [PubMed] [Google Scholar]
- Rascon Trincado MV, Lorente Toledano F, Villalobos VS. A study of the functions of polymorphonuclear neutrophil in patients with Down’s syndrome. Allergol Immunopathol (Madr) 1988;16:339–45. [PubMed] [Google Scholar]
- Reuland-Bosma W, van den Barselaar MT, van de Gevel JS, Leijh PC, de Vries-Huiges H, The HT. Nonspecific and specific immune responses in a child with Down’s syndrome and her sibling. A case report. J Periodontol. 1988;59:249–53. doi: 10.1902/jop.1988.59.4.249. [DOI] [PubMed] [Google Scholar]
- Reuland-Bosma W, van Dijk J. Periodontal disease in Down’s syndrome: a review. J Clin Periodontol. 1986;13:64–73. doi: 10.1111/j.1600-051x.1986.tb01416.x. [DOI] [PubMed] [Google Scholar]
- Sakellari D, Arapostathis KN, Konstantinidis A. Periodontal conditions and subgingival microflora in Down syndrome patients. A case-control study.[see comment] J Clin Periodontol. 2005;32:684–90. doi: 10.1111/j.1600-051X.2005.00737.x. [DOI] [PubMed] [Google Scholar]
- Sherman SL, Allen EG, Bean LH, Freeman SB. Epidemiology of Down syndrome. [Review] [93 refs] Ment Retard Dev Disabil Res Rev. 2007;13:221–7. doi: 10.1002/mrdd.20157. [DOI] [PubMed] [Google Scholar]
- Shin M, Besser LM, Kucik JE, Lu C, Siffel C, Correa A Congenital Anomaly Multistate P and Survival C. Prevalence of Down syndrome among children and adolescents in 10 regions of the United States. Pediatrics. 2009;124:1565–71. doi: 10.1542/peds.2009-0745. [DOI] [PubMed] [Google Scholar]
- Sohoel DC, Johannessen AC, Kristoffersen T, Nilsen R. Expression of HLA class II antigens in marginal periodontitis of patients with Down’s syndrome. Eur J Oral Sci. 1995;103:207–13. doi: 10.1111/j.1600-0722.1995.tb00161.x. [DOI] [PubMed] [Google Scholar]
- Sohoel PD, Johannessen AC, Kristoffersen T, Haugstvedt Y, Nilsen R. In situ characterization of mononuclear cells in marginal periodontitis of patients with Down’s syndrome. Acta Odontol Scand. 1992;50:141–9. doi: 10.3109/00016359209012757. [DOI] [PubMed] [Google Scholar]
- Sreedevi H, Munshi AK. Neutrophil chemotaxis in Down syndrome and normal children to Actinobacillus actinomycetemcomitans. J Clin Pediatr Dent. 1998;22:141–6. [PubMed] [Google Scholar]
- Strydom A, Dickinson MJ, Shende S, Pratico D, Walker Z. Oxidative stress and cognitive ability in adults with Down syndrome. Prog Neuropsychopharmacol Biol Psychiatry. 2009;33:76–80. doi: 10.1016/j.pnpbp.2008.10.006. [DOI] [PubMed] [Google Scholar]
- Wysocki H, Wysocki J, Wierusz-Wysocka B. The influence of thymus extract on the phagocytosis and the bactericidal capacity of polymorphonuclear neutrophils from children with Down’s syndrome. Ann N Y Acad Sci. 1987;496:740–2. doi: 10.1111/j.1749-6632.1987.tb35839.x. [DOI] [PubMed] [Google Scholar]
- Yavuzyilmaz E, Ersoy F, Sanal O, Tezcan I, Ercal D. Neutrophil chemotaxis and periodontal status in Down’s syndrome patients. J Nihon Univ Sch Dent. 1993;35:91–5. doi: 10.2334/josnusd1959.35.91. [DOI] [PubMed] [Google Scholar]
- Younes R, Ghorra C, Khalife S, Igondjo-Tchen-Changotade S, Yousfi M, Willig C, Senni K, Godeau G, Naaman N. Pertinent cell population to characterize periodontal disease. Tissue & Cell. 2009;41:141–50. doi: 10.1016/j.tice.2008.09.003. [DOI] [PubMed] [Google Scholar]