
FIGURE 1. Morphological features in representative samples of erythrodermic CTCL and inflammatory dermatoses.
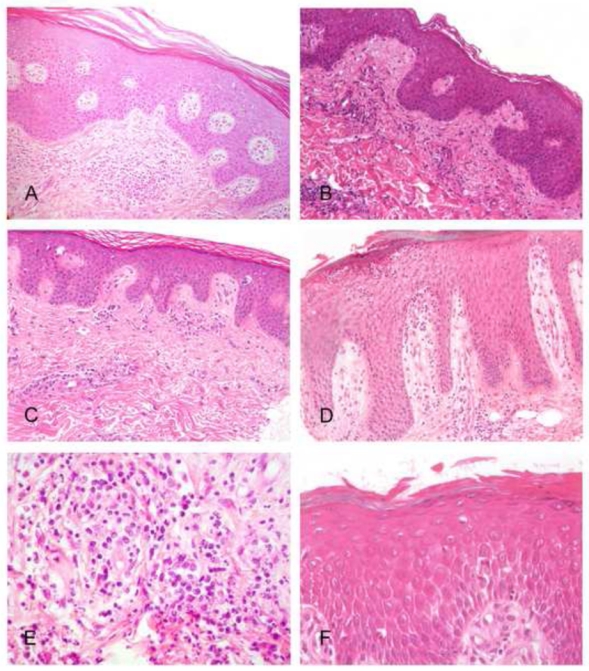
A, C and E show examples of erythrodermic CTCL, while B, D, F are from the EID group. A, In this Sézary syndrome, skin biopsy did not allow a definite diagnosis, only showing a perivascular lymphocytic infiltrate without atypical lymphocyte, with an overlying hyperplastic and parakeratotic epidermis with slight spongiosis. B, In this erythrodermic drug reaction sample, a common perivascular lymphocytic infiltrate is seen, while no interface dermatitis and no apoptotic keratinocytes are identified. C, This Sézary syndrome sample show a very discrete infiltrate in the dermis, but atypical lymphocytes and Pautrier’s microabcesses can be identified in the epidermis, constiting of aggregates of atypical lymphocytes showing enlarged circonvoluted hyperchromatic nuclei (arrow), allowing histopathological diagnosis. D, This sample from a psoriatic erythrodermic patient shows an irregular epidermal hyperplasia with a multilocular subcorneal pustule. E, Atypical lymphocytes admixed with neutrophils are present within the infiltrate of this erythrodermic CTCL sample. F, Confluent spongiosis (pre-vesicles) is seen in this skin biopsy from an erythrodermic allergic contact dermatitis.