
Figure 2. Strategies for coupling therapeutic agents to RBC and ECs.
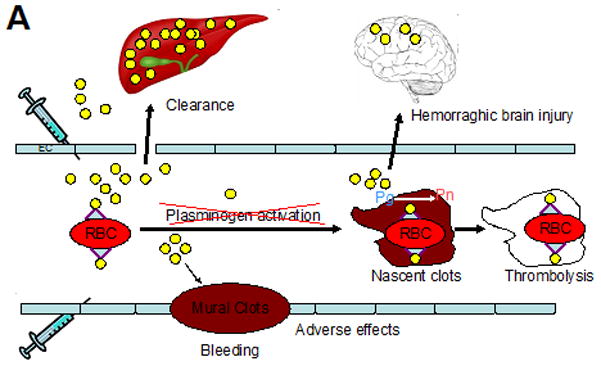
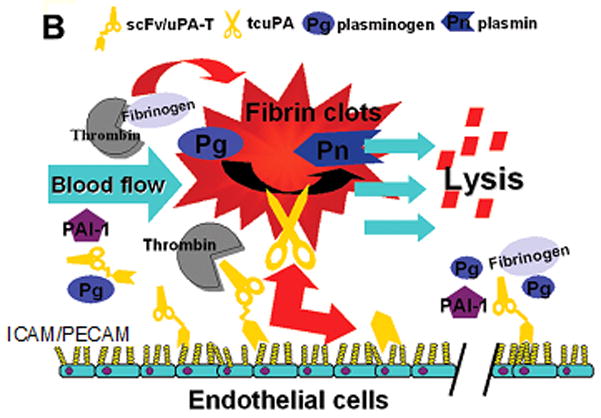
(A) Plasminogen activators (yellow dots) are relatively ineffective, in part due to rapid uptake by liver, and unsafe due to bleeding (indiscriminate lysis of hemostatic mural clots), vascular side effects (e.g. activation of receptors on endothelial cells, EC) and injurious effects of tPA diffusing into the CNS. Coupling to RBC will dramatically prolong the longevity of the scFv/tPA variant. RBC will restrain scFv/tPA binding to cellular receptors, and restrict its access into mural hemostatic clots and the CNS. Propulsion of RBC towards the mainstream will further offset interactions of the pro-drug with hemostatic clots and vascular walls. RBC-bound scFv/tPA will have virtually unlimited access to the interior of nascent pathological thrombi and thereby will dissolve pathological intravascular clots and prevent vascular occlusion. (B) As with RBC/tPA, ICAM or PECAM targeting enables one to target more locally in this case the pulmonary vasculature versus more systemically in the case of RBCs. By diversifying targeting, we can improve specificity and limit adverse effects. Abbreviations found within the figure-ICAM-1, Intercellular adhesion molecule, 1; PAI-1, Plasminogen activator inhibitor-1; PECAM-1, Platelet endothelial cell adhesion molecule-1; Pg, Plasminogen; Pn, Plasmin; RBC, red blood cell; tPA, tissue plasminogen activator; uPA-T, urokinase plasminogen activator-thrombin.