
Fig. 11.
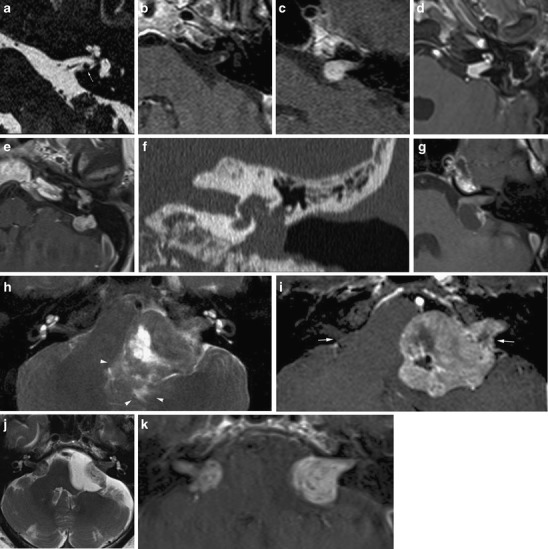
Imaging features of vestibular schwannomas. A nodular lesion is seen along the inferior vestibular nerve (a) with strong enhancement (b). This is the typical site of origin of a schwannoma. c The typical growth pattern of a schwannoma is towards and extending into the CPA resembling an “ice-cream cone”. d Less frequently, involvement of the inner ear is seen: in this case transmodiolar extension causes enhancement of the cochlea. e-f In rare cases extensive transotic growth may occur. In this patient, tumour involvement of the inner ear, endolymphatic duct and sac and the middle ear is present. Coronal CT (f) shows widening of the oval window, caused by the tumour extension to the middle ear cleft. g The extracanalicular portion of a schwannoma may show cystic degeneration. In this patient the cyst formation is located posterior to the IAC, resulting in a somewhat atypical appearance eccentric to the porus. Such cyst formation seems to be associated with rapid growth. h, i Further growth of a schwannoma will result in compression of the brain stem and cerebellum and eventually other cranial nerves such as the trigeminal nerve. In this patient compression of the fourth ventricle caused hydrocephalus (not shown). Note also the edema in the surrounding parenchyma (arrowheads on T2) and erosion of the porus (arrows on contrast enhanced T1). j, k Bilateral schwannomas are a hallmark of neurofibromatosis type 2. On the left, an arachnoid cyst has occured secondary to the mass lesion. Depending on the patient history, metastases should be considered as a differential diagnosis