

Abstract
Objective
High tibial osteotomy (HTO) is one treatment option for young and active patients with unicompartmental osteoarthritis. The success of this procedure substantially depends on the degree of correction of the mechanical axis. Computer-assisted navigation systems are believed to improve the precision of axis correction through intraoperative real-time monitoring. This study investigates the accuracy of limb alignment measurements with a navigation system on a cadaver specimen.
Materials and methods
The measurements were performed on a well-preserved cadaver specimen with a mechanical leg axis of 4° varus. Data was collected during the HTO workflow. Repeated serial measurements were undertaken by four different surgeons. After these measurements, different landmarks were deliberately set at the wrong place to examine the influence of mistakes during registration.
Results
There was a high intra-and interobserver reliability with a mean mechanical leg axis of 3.9° ± 0.7° and a mean error of 0.6°. The grossly incorrect placement of landmarks for knee and ankle center resulted in an incorrect mechanical leg axis of 1° valgus up to 10° varus.
Conclusion
The computer-assisted navigation system provided precise information about the mechanical leg axis, irrespective of the observer's experience.
Introduction
High tibial osteotomy (HTO) is an established treatment option for young and active patients with unicompartmental osteoarthritis (OA) of the knee since the 1960s [1,2]. The success of this procedure depends on several factors including degree of OA, loss of articular cartilage, osseous deformity of the tibia, range of motion, age, gender and body mass index [3-7]. One important factor is the degree of correction of the mechanical leg axis [4,7-10]. It was demonstrated that malalignment increases the risk of progression of OA [11]. Under-and overcorrection are the main reasons for clinical failure of this procedure [9]. There are different methods to control the correction intraoperatively: cable-method [12], grids [13] and preoperative planning. But all these methods have limitations and can lead to severe under-or overcorrection.
Computer-assisted navigation systems with a system-determined error within 1° [14] allow to monitor the correction of the leg axis intraoperatively in real-time and may thus improve the efficiency of HTO. Navigation systems were shown to increase the precision of limb alignment in total knee arthroplasty [15]. In cadaver and clinical trials using radiographic or CT measurement of the leg axis as reference [16,17], navigated open-wedge HTO made it possible to correct the mechanical leg axis more precisely than with conventional surgical technique.
It has been observed that radiographic and navigation measurements of limb alignment do not correlate and that the navigation system may be the more precise evaluation tool [18].
This study investigates the accuracy of lower limb alignment measurement with a navigation system on a cadaver specimen and the impact of mistakes during landmark registration.
Materials and methods
The study protocol was approved by the local independent ethics committee on 30.07.2008. Serial measurements were performed on a well preserved cadaver specimen. The mechanical leg axis was calculated with fluoroscopic images of the hip, knee and ankle joint with the knee in full extension and neutral rotation using a grid with lead-impregnated reference lines and controlled through direct measurement on the cadaver.
We used the Aesculap OrthoPilot navigation system (Aesculap, Tuttlingen, Germany) to measure limb alignment. Data were collected with the software HTO 1.4 Open Wedge (Aesculap, Tuttlingen, Germany). Bicortical trackers were fixed at the distal femur und the tibia. The workflow started with palpation of the anatomic knee center with the knee 90° flexed. The acquisition of the hip center was done through movement of the femur around its longitudinal axis. For registering the ankle center, a tracker was fixed at the metatarsal region using a foot plate with elastic strip, the foot being moved from extension to flexion. The knee center was located by movement of the leg from flexion to extension. Then, anatomical landmarks such as the medial and lateral epicondyle, the medial and the lateral malleolus and the anterior ankle center were registered.
Repeated serial measurements were undertaken 5 times by each of the 4 different observers. Two observers (observer 1 and 4) had already experience with the use of this navigation system, one of them also with other navigation systems (observer 1) and two observers no previous experience at all (observer 2 and 3). All data were recorded with the software of the navigation system.
After these measurements with correct data acquisition, different landmarks were moved to obviously wrong places to study the influence of mistakes during landmark registration. The following landmarks were moved: insufficient fixation of the pelvis during hip center acquisition, medialisation and lateralisation of the anatomic knee center of 15 mm, ventralisation of the medial, the lateral and both epicondyles of 10 mm, medialisation and lateralisation of the ankle center of 10 mm. Only one landmark was moved at a time. After each move, the mechanical leg axis was recorded.
Statistical Analysis
Data are expressed as means with a minimum, maximum and 95% confidence interval and shown graphically on box plots. To assess the of reliability of the measurement method, the repeatability coefficient was used [19].
The results of these exploratory significance tests are summarized using p-values, where p < 0.05 indicates significant differences between sub-samples. All analyses were performed with the SPSS® software (SPSS Inc., Chicago, Illinois, USA, release 16.0 for Windows®).
Results
The radiographic and direct measurements on the cadaver leg showed a mechanical leg axis of 4° varus malalignment. Lower limb alignment measurements with the navigation system yielded an overall mean mechanical leg axis of 3.9° ± 0.7° (2.7° to 5.1°) of varus malalignment (Table 1, Figure 1). Calculated relative to 4° of varus malalignment obtained by radiography and controlled by direct measurement, the mean error was 0.6°.
Table 1.
Measurements of the mechanical leg axis of a cadaver leg with 4° of varus malalignment with the navigation system
| Mechanical leg axis | N | Min (°) | Max (°) | Mean (°) | SD (°) | Mean error (°) |
|---|---|---|---|---|---|---|
| All | 20 | 2.7 | 5.1 | 3.9 | 0.7 | 0.6 |
| Observer1 | 5 | 2.7 | 4.5 | 3.9 | 0.8 | 0.7 |
| Observer2 | 5 | 3.3 | 5.1 | 4.4 | 0.7 | 0.7 |
| Observer3 | 5 | 2.7 | 4.4 | 3.5 | 0.6 | 0.7 |
| Observer4 | 5 | 3.1 | 4.8 | 4.0 | 0.7 | 0.5 |
Figure 1.
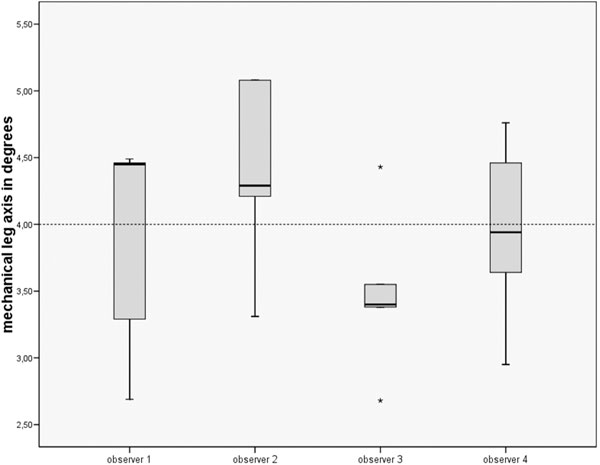
Distribution of the measurements of the mechanical legaxis of a cadaver leg with 4° of varus malalignment.
Intra-and interobserver reliability
Intraobserver error was low with a mean error of 0.5° to 0.7° for each of the four observers with no significant difference between them (p = 0.311). There was also no difference between the two observers with previous experience with navigation systems and the two observers without experience.
The repeatability coefficient [19] was 2.3 which means that 95% of all measurements would be within this range of 2.3°.
Influence of mistakes during landmark registration
Mistakes during landmark registration had a relevant impact on the calculation of the mechanical leg axis (Table 2). Medial or lateral shift of the knee center resulted in an error of up to 6.4° while medial or lateral shift of the ankle center brought about a lower but still relevant error of up to 2.4°. Insufficient pelvic fixation during hip center registration had only low impact, the error being in the vicinity of the variations between the different observers. Shifting of the epicondyles had no impact at all.
Table 2.
Influence of failure during landmark acquisition on a cadaver leg with 4° of varus malalignment
| Parameter | Failure | Mechanical leg axis |
|---|---|---|
| Hip center | Insufficient fixation of the pelvis | 5.5° Varus |
| Knee center | 15 mm medial shift | 0.7° Valgus |
| 15 mm lateral shift | 10.4° Varus | |
| Transepikondylar line | 10 mm ventral shift | 4° Varus |
| 10 mm proximal shift | 4° Varus | |
| Ankle center | 10 mm medial shift | 5.9° Varus |
| 10 mm lateral shift | 1.6° Varus |
Discussion
Despite the frequent use of Computer-assisted navigation systems in orthopaedic surgery, only few studies have assessed the accuracy of these navigation systems. Keppler et al. [20] validated one navigation system using a plastic bone model and found a mean error of 0.4° in the frontal plane. Wang et al. [21] validated another navigation system also using a plastic bone model and demonstrated a mean error of 0.5° in the frontal plane. In an experimental setting using a phantom leg, Pitto et al. [14] tested a third navigation system and reported a mean error of a within 1° generally. These studies were performed with total knee arthroplasty workflow. They expected a lower accuracy in a clinical setting.
Goleski et al. [22] compared navigated measurement of lower limb alignment with HTO workflow on 13 cadaver legs with 3-dimensional computed tomography measurements and found a good correlation in the frontal leg alignment. However, the maximum differences between navigation and CT-measurement were 3.6° preoperatively and 5.6° postoperatively. They were less pronounced in minor deformities. This is still an experimental setting, but closer to clinical reality than a plastic bone model.
On a well-preserved cadaver leg, our study found an overall mean error of navigation measurements of 0.6° from the "real" alignment in the frontal plane, a maximum error of 1.3° and a maximum difference between all measurements of 2.4°. Limitations of our study include that only one cadaver leg was used, that the measurements were done consecutively and that the "real" alignment of the leg was measured using fluoroscopic images and a grid with lead-impregnated reference lines. However, the mechanical axis was measured correctly irrespective of the observer's experience with navigation systems, suggesting that following the instructions of the navigation system will provide an accurate result.
Mistakes during landmark registration (e.g. medial or lateral shift of the knee or ankle center) resulted in a significant error of the mechanical leg axis and should thus be carefully avoided.
In total knee arthroplasty, there is consensus about "good" lower limb alignment of ± 3° from a neutral mechanical axis, but not in HTO. A ± 3° deviation might be too large to achieve good long-term results. In the clinical setting, an accuracy of ± 1° would meet the surgeon's needs. However, the currently used whole-leg standing radiograph as outcome measurement for lower limb alignment is fraught with potential inaccuracies [18,23].
Conclusion
In the calculation of the mechanical leg axis, the computer-assisted navigation system achieved an accuracy of ± 1°. Intra-and interobserver reliability was high, irrespective of the observer's experience. Care must be taken during landmark registration especially for the knee and ankle center, because mistakes during acquisition of these landmarks resulted in a relevant mistake in the calculation of the mechanical leg axis.
Conflict of interests statement
The authors have received no funding for this study.
Acknowledgements
The authors are grateful to Heike Voigt for her valuable assistance in data management and evaluation. This study has been performed within the ORTHO MIT project.
References
- Coventry MB. Osteotomy of the Upper Portion of the Tibia for Degenerative Arthritis of the Knee. A Preliminary Report. J Bone Joint Surg Am. 1965;47:984–90. [PubMed] [Google Scholar]
- Jackson JP, Waugh W. Tibial osteotomy for osteoarthritis of the knee. J Bone Joint Surg Br. 1961;43-B:746–51. doi: 10.1302/0301-620X.43B4.746. [DOI] [PubMed] [Google Scholar]
- van Raaij T, Reijman M, Brouwer RW, Jakma TS, Verhaar JN. Survival of closing-wedge high tibial osteotomy: good outcome in men with low-grade osteoarthritis after 10-16 years. Acta Orthop. 2008;79:230–4. doi: 10.1080/17453670710015021. [DOI] [PubMed] [Google Scholar]
- Coventry MB, Ilstrup DM, Wallrichs SL. Proximal tibial osteotomy. A critical long-term study of eighty-seven cases. J Bone Joint Surg Am. 1993;75:196–201. doi: 10.2106/00004623-199302000-00006. [DOI] [PubMed] [Google Scholar]
- Spahn G, Kirschbaum S, Kahl E. Factors that influence high tibial osteotomy results in patients with medial gonarthritis: a score to predict the results. Osteoarthritis Cartilage. 2006;14:190–5. doi: 10.1016/j.joca.2005.08.013. [DOI] [PubMed] [Google Scholar]
- Bonnin M, Chambat P. [Current status of valgus angle, tibial head closing wedge osteotomy in media gonarthrosis] Orthopade. 2004;33:135–42. doi: 10.1007/s00132-003-0586-z. [DOI] [PubMed] [Google Scholar]
- Matthews LS, Goldstein SA, Malvitz TA, Katz BP, Kaufer H. Proximal tibial osteotomy. Factors that influence the duration of satisfactory function. Clin Orthop Relat Res. 1998. pp. 193–200. [PubMed]
- Fujisawa Y, Masuhara K, Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am. 1979;10:585–608. [PubMed] [Google Scholar]
- Hernigou P, Medevielle D, Debeyre J, Goutallier D. Proximal tibial osteotomy for osteoarthritis with varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am. 1987;69:332–54. [PubMed] [Google Scholar]
- Sprenger TR, Doerzbacher JF. Tibial osteotomy for the treatment of varus gonarthrosis. Survival and failure analysis to twenty-two years. J Bone Joint Surg Am. 2003;85-A:469–74. [PubMed] [Google Scholar]
- Sharma L. et al. The role of knee alignment in disease progression and functional decline in knee osteoarthritis. Jama. 2001;286:, 188–95. doi: 10.1001/jama.286.2.188. [DOI] [PubMed] [Google Scholar]
- Krettek C, Miclau T, Grun O, Schandelmaier P, Tscherne H. Intraoperative control of axes, rotation and length in femoral and tibial fractures. Technical note. Injury. 1998;29(Suppl 3):29–39. doi: 10.1016/s0020-1383(98)95006-9. [DOI] [PubMed] [Google Scholar]
- Saleh M, Harriman P, Edwards DJ. A radiological method for producing precise limb alignment. J Bone Joint Surg Br. 1991;73:515–6. doi: 10.1302/0301-620X.73B3.1670463. [DOI] [PubMed] [Google Scholar]
- Pitto RP. et al. Accuracy of a computer-assisted navigation system for total knee replacement. J Bone Joint Surg Br. 2006;88:601–5. doi: 10.1302/0301-620X.88B5.17431. [DOI] [PubMed] [Google Scholar]
- Bauwens K. et al. Navigated Total Knee Replacement. A Meta-Analysis. J Bone Joint Surg Am. 2007;89:261–269. doi: 10.2106/JBJS.F.00601. [DOI] [PubMed] [Google Scholar]
- Hankemeier S. et al. Navigated open-wedge high tibial osteotomy: advantages and disadvantages compared to the conventional technique in a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2006;14:917–21. doi: 10.1007/s00167-006-0035-8. [DOI] [PubMed] [Google Scholar]
- Kim SJ, Medial opening wedge high-tibial osteotomy using a kinematic navigation system versus a conventional method: a 1-year retrospective, comparative study. 2008. [DOI] [PubMed]
- Yaffe MA, Koo SS, Stulberg SD. Radiographic and navigation measurements of TKA limb alignment do not correlate. Clin Orthop Relat Res. 2008;466:2736–44. doi: 10.1007/s11999-008-0427-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8:135–60. doi: 10.1191/096228099673819272. [DOI] [PubMed] [Google Scholar]
- Keppler P. et al. Computer aided high tibial open wedge osteotomy. Injury. 2004;35(Suppl 1):68–78. doi: 10.1016/j.injury.2004.05.013. [DOI] [PubMed] [Google Scholar]
- Wang G. et al. Implementation, accuracy evaluation, and preliminary clinical trial of a CT-free navigation system for high tibial opening wedge osteotomy. Comput Aided Surg. 2005;10:73–85. doi: 10.3109/10929080500228837. [DOI] [PubMed] [Google Scholar]
- Goleski P. et al. Reliability of navigated lower limb alignment in high tibial osteotomies. Am J Sports Med. 2008;36:2179–86. doi: 10.1177/0363546508319314. [DOI] [PubMed] [Google Scholar]
- Krackow KA, Pepe CL, Galloway EJ. A mathematical analysis of the effect of flexion and rotation on apparent varus/valgus alignment at the knee. Orthopedics. 1990;13:861–8. doi: 10.3928/0147-7447-19900801-09. [DOI] [PubMed] [Google Scholar]