

Abstract
Ellis-van Creveld syndrome is a rare autosomal-recessive disorder characterized by short limbs, post-axial polydactyly, ectodermal dysplasia, edentulous mandibular incisor region, absence of mucobuccal fold, congenitally missing teeth, slight serrations of the alveolar ridge and multiple small alveolar notches. The clinical report not only describes the classical oral and dental manifestations of Ellis-van Creveld syndrome but also presents unusual findings such as single-rooted and funnel-shaped primary first molars, single conical roots of primary second molars and taurodontisum, which must be considered in the differential diagnostic criteria to avoid misdiagnosis of syndromes. The article also discusses the differential diagnosis and preventive and therapeutic oral health care for these patients. The management of Ellis-van Creveld syndrome is multidisciplinary and, therefore, the oral health care provider should get updated with latest knowledge for timely referral to prevent the patient from further complications of heart defect and bony deformity.
Keywords: Absence of mucobuccal fold, alveolar notches, autosomal recessive, genu valgum, partial harelip
Introduction
Ellis-van Creveld syndrome (EvC, OMIM # 225500), also known as chondroectodermal dysplasia, was first described by Ellis and van Creveld in 1940.[1] The syndrome is caused by a mutation in the two genes EVC1 and EVC2, mapping both on chromosome 4p16, in a head to head configuration.[2,3] The disorder is commonly seen among the Old Order Amish Community of Pennsylvania (approximately five of 1,000 live births), but, today, the syndrome is known to affect all races. In the general population, the birth prevalence is estimated to be 7/1,000,000.[4] Parental consanguinity was reported with 30% of the cases.[5] Ellis-van Creveld syndrome is a rare autosomal-recessive disorder affecting bone growth, for which minimally diagnostic criteria include short limb dwarfism, postaxial polydactyly of hands and feet, malformation of the wrist bones, hypoplastic fingernails, teeth dystrophy and congenital heart defect (particularly atrioventricular canal with common atrium).[1] The clinical report outlines the classical and unusual oral and dental manifestations, which will assist the oral health care providers in diagnosing the syndrome and timely referrals to appropriate health care professionals to prevent the patient from further complications of heart defect and bony deformity.
Case Report
An 11-year-old female patient reported to the department with the chief complaint of pain and mobility in the mandibular right posterior region since 1 month. Family history revealed that the girl was the first child of consanguineously married and normally developed parents. She has a sister (9 years) and a brother (7 years) with no congenital abnormality. Pregnancy and birth was uneventful. Medical history revealed congenital heart defect (single atrium), which was corrected at the age of 2 years. Developmental history revealed that the patient started walking at the age of 3 years and the teeth started erupting at the same age. The patient was short statured (97 cm), which was relatively short for her age, and had a waddling gait. The limbs were shortened and markedly deformed. Fingernails were hypoplastic, thin and spoon shaped. Bimanual hexadactyly was noted on the ulnar side [Figure 1]. Head morphology, facial appearance and quality and quantity of hair were normal. Intraoral examination revealed carious primary mandibular right second molar, edentulous mandibular incisor region, absence of mandibular anterior mucobuccal fold, mandibular hyperplastic frenula and morphological abnormalities of maxillary and mandibular anterior teeth [Figures 2 and 3]. Slight serrations of the alveolar ridge were observed distally to the maxillary central incisors [Figure 3]. Panoramic radiograph showed missing permanent maxillary right lateral incisor and permanent mandibular central incisors, delayed formation of tooth buds of permanent maxillary right and left canines, first and second premolars and permanent mandibular left canines, first and second premolars [Table 1]. Primary first molars and maxillary primary second molars were single rooted; roots of primary mandibular second molars were conical and convergent. Taurodontisum were present with all the first permanent molars [Figure 4] [Table 1]. Intraoral periapical radiograph showed multiple small alveolar notches on the crest of the mandibular anterior alveolar ridge, giving a serrated appearance [Figure 5]. Radiograph of the upper and lower limb showed shortening of the extremities, genu valgum, post-axial polydactyly, fusion of hamate and capitate bones and fusion of the 5th and 6th metacarpal bones [Figure 6]. Based on the clinical and radiographic findings, we strongly suspected Ellis-van Creveld syndrome. Thereafter, the patient was referred to the pediatrician for thorough medical examination to reveal any evidence of systemic involvement, such as congenital heart malformation, lung, liver, kidney and central nervous system disorders. Her mental development was within the normal range and no systemic involvement was reported; thus, confirming the diagnosis.
Figure 1.

Hypoplastic fingernails of the hands
Figure 2.

Intraoral photograph showing edentulous mandibular central incisor region, absence of mandibular anterior mucobuccal fold and hyperplastic frenula
Figure 3.

Morphological abnormalities of maxillary and mandibular anterior teeth and serrations of the alveolar ridge
Table 1.
Comparison of oral manifestation of Ellis-van Creveld syndrome in the literature with the patient from this report
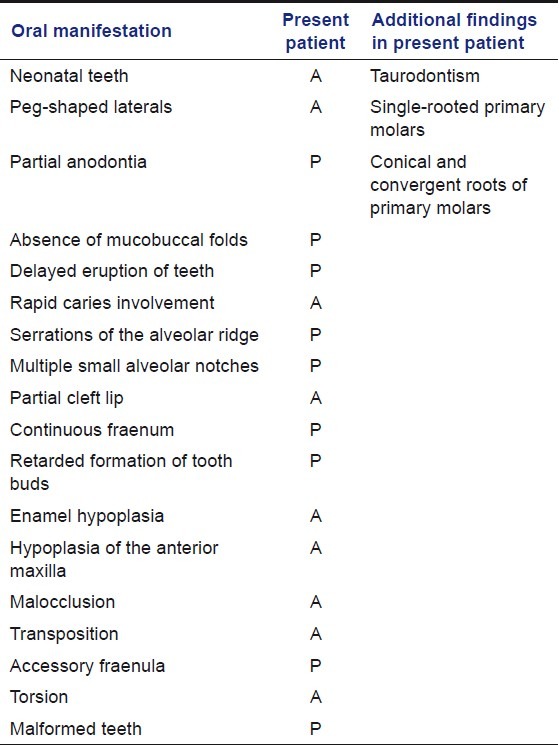
Figure 4.

Panoramic radiograph showing missing teeth, delayed formation of tooth buds, single-rooted primary molars and taurodontisum
Figure 5.

Radiograph showing multiple small alveolar notches giving a serrated appearance
Figure 6.
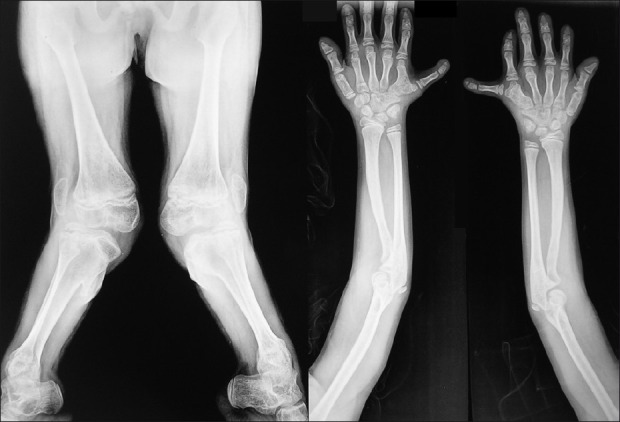
Radiograph of the upper and lower limb showed shortening of the extremities, genu valgum, post-axial polydactyly, fusion of hamate and capitate bones and fusion of 5th and 6th metacarpals
Clinically, the mandibular right primary second molar was unrestorable. Radiographically, 2/3rd of the pathologic root resorption was evident with the same tooth. Therefore, mandibular right primary second molar was extracted under local anesthesia using Lignocaine hydrochloride (Dentocaine 2% Pharma Health Care Product, Mumbai, Mumbai, India) and antibiotic coverage. To increase the mandibular anterior mucobuccal fold, frenectomy was advised but the patient's parent refused for the frenectomy. After 15 days, healing and follow-up were uneventful.
Discussion
The presentation of medically compromised and syndromic children in the dental office is a great challenge to the oral health care providers. Various syndromes are identified early in children and demand special attention right from birth. Ellis-van Creveld syndrome is one of these syndromes, which is characterized by ectodermal disturbances and chondrodysplasia.[2]
Ellis-van Creveld syndrome presents phenotypic diverse oral manifestations of the soft tissues and teeth. These include hyperplastic frenula, absence of mucobuccal fold, serrations of the alveolar ridge, multiple small alveolar notches, partial cleft lip, neonatal teeth, peg-shaped laterals, partial anodontia, conical and microdontic teeth, enamel hypoplasia and delayed eruption of teeth [Table 1].[1,6,7] But, similar oral manifestations are also observed in other syndromes like Jeune syndrome (JS), Orofaciodigital syndrome (OFDS), McKusick-Kaufman syndrome (MKK) and Weyers acrofacial dysostosis (WAD). Thus, we consider these syndromes in the differential diagnosis of Ellis-van Creveld. JS is an inherited form of dwarfism that produces short limbs similar to Ellis-van Creveld. Other symptoms the individuals of JS may have and are absent in Ellis-van Creveld are small chest, renal dysplasia, retinal degeneration, liver dysplasia and intestinal malformation. In addition, individuals with Ellis-van Creveld have a finger nail hypoplasia, a finding generally absent in JS.[8] MKK syndrome, a recessively inherited disorder, can be distinguished from Ellis-van Creveld by the presence of hydrometrocolpos in the former, whereas WAS, an autosomal-dominant condition has ectodermal disturbances similar to Ellis-van Creveld but absence of other features like dwarfism, thoracic-dysplasia and congenital heart diseases.[9,10] As all the clinical findings in the reported patient were favoring Ellis-van Creveld syndrome, the diagnosis was thus made. Many new cases reported present a rare aberration in shape and structure of the teeth. In the present case, we noticed some unusual findings such as single-rooted and funnel-shaped primary first molars, single conical roots of primary second molars and taurodontisum [Table 1]. Investigations have shown that dental anomalies like taurodontisum and single conical root forms of primary molars may develop in the presence of any one of a large number of different genetic alterations. These findings suggest that the chromosomal abnormalities may disrupt the development of the tooth's form and that these anomalies are not the result of a specific genetic abnormality.[11] Thus, the additional findings of single conical root forms of primary molars and taurodontisum in the present case could possibly serve as diagnostic criteria for Ellis-van Creveld, but more often may lead to misdiagnosis if the more relevant oral and general findings are inconclusive. Taurodontisum is a noted observation in OFDS and so are the other oral features of Ellis-van Creveld. However, OFDS can be differentiated from Ellis-van Creveld by the presence of cleft palate, trifurcation of soft palate, ocular hypertelorism, hypoplasia of alae nasi, polycystic kidney diseases and mild intellectual deformity (50%) in the patients of OFDS.[12] Single conical roots in relation to primary molars and taurodontisum were also reported by Vinay[13] and Hunter,[14] respectively.
Malocclusions are common in Ellis-van Creveld but are not of any specific type. The literature described hypoplasia of the anterior maxilla, prognathism of the mandible and increased height of the lower third of the face.[4] In the present case report, we did not observe any such malocclusion.
Developmental history of the patient revealed delayed eruption of teeth. Radiographical examination showed delay in the calcification of permanent teeth. Thus, the dental age of our patient does not correspond to the chronological age.
Unfortunately, 50% of the children with Ellis-van Creveld syndrome die in early infancy due to cardiorespiratory problems, and those who survive require a multidisciplinary approach for treatment, i.e. orthopedic correction of genuvalgum, amputation of extra digit, surgical repair of cardiac malformation and dental intervention.[15]
As there are many oral manifestations, there is no standard formula for dental treatment. Treatment planning and delivery may require an interdisciplinary approach. Treatment needs may include preventive measures against caries, restorations of decayed and malformed teeth, partial dentures with frequent adjustment and replacement and correction of malocclusion. Children with Ellis-van Creveld syndrome have a high risk for caries due to malformed hypoplastic teeth and molars with deeps pits and fissures. Therefore, the patient and the patient's parents should be made aware of the importance of home-based preventive measures such as diet control, oral hygiene maintenance, daily fluoride mouth rinses and use of fluoridated denitrifies. Simultaneously, preventive professional care such as pit and fissure sealants, oral prophylaxis and professional topical fluoride application must be provided. Congenitally missing teeth, hypoplastic teeth and malocclusion can affect the speech, appearance and mastication of patients with Ellis-van Creveld syndrome. To maintain space and to improve speech, mastication and esthetic, partial or fixed denture (considering age) is advocated. Hypoplastic teeth and decayed teeth can be restored with composite restorations for better esthetics and preservation of tooth structure.[5,16] Parental and child counseling is often required to treat psychological trauma due to compromised oral manifestations and medical health. Surgical correction is advised for soft tissue and skeletal abnormalities.[17]
Often, one may misunderstand the use of antibiotics to prevent endocarditis. Antibiotics prophylaxis is recommended for surgical patients with prosthetic cardiac valves, previous bacterial endocarditis, mitral valve prolapse with valvular regurgitation or thickened leaflets. For these patients, anti-Staphylococcal antibiotics (e.g., cephalosporins) should be given before surgery only, when the procedure involves significant risk of bacteremia (e.g., incision into infected tissues) or as soon as the risk is recognized.[18] Ellis-van Creveld syndrome has a high incidence of congenital cardiac defects. The dental treatment must be performed under prophylactic antibiotic coverage with consideration for the high incidence of cardiac defects in Ellis-van Creveld patients. But, as in the present case, the defect was corrected at the age of 2 years, there was no previous history of bacterial endocarditis and the present cardiac examination was normal (as reported by the pediatrician), there was no indication for antibiotic prophylaxis. However, to control the spread of local infection (as indicated by the 2/3 pathologic root resorption of the carious primary mandibular right second molar), antibiotic coverage was provided.
Conclusion
Diagnosis and management of Ellis-van Creveld syndrome is a great challenge to the oral health care provider. Because of the genetic and environmental phenotype-modifying factors in syndromes, the oral health care providers may come across some unusual oral and dental manifestations. Therefore, they should get updated with the latest knowledge to minimize the risk of misdiagnosis. To achieve satisfactory functional and aesthetic results, multidisciplinary treatment planning is required both in terms of preventing oral disease and in providing restorative care.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Ellis RW, van Creveld S. A syndrome characterized by ectodermal dysplasia, polydactyly, chondrodysplasia and congenital morbus cordis. Report of 3 cases. Arch Oral Dis Child. 1940;15:65–4. doi: 10.1136/adc.15.82.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ruiz-Perez VL, Ide SE, Strom TM. Mutation in a new gene in Ellis-van Creveld Syndrome and weyers acrodental dysostosis. Nat Genet. 2000;24:283–6. doi: 10.1038/73508. [DOI] [PubMed] [Google Scholar]
- 3.Galdzicka M, Patnala S, Hirshman MG, Cai JF, Nitowsky H, Egeland JA, et al. A new gene, EVC2, is mutated in Ellis-van Creveld syndrome. Mol Genet Metab. 2002;77:291–5. doi: 10.1016/s1096-7192(02)00178-6. [DOI] [PubMed] [Google Scholar]
- 4.Mckusick VA, Egeland JA, Eldridge R, Krusen DE. Dwarfism in the Amish I. The Ellis-van Creveld Syndrome. Bull Johns Hopkins Hosp. 1964;115:306–36. [PubMed] [Google Scholar]
- 5.Cahuana A, Palma C, Gonzales W, Gean E. Oral manifestation in Ellis-van Creveld syndrome: Report of 5 cases. Pediatr Dent. 2004;26:277–82. [PubMed] [Google Scholar]
- 6.Himelhoch DA, Mostoji R. Oral manifestations in the Ellis-van Creveld Syndrome. Case report. Pediatr Dent. 1988;10:309–13. [PubMed] [Google Scholar]
- 7.Sarnat H, Amir E, Legum CP. Developmental Dental anomaliesin chondrectodermal dysplasia (Ellis-van Creveld Syndrome) J Dent Child. 1980;47:28–31. [PubMed] [Google Scholar]
- 8.Tüysüz B, Bariş S, Aksoy F, Madazli R, Ungür S, Sever L. Clinical variability of asphyxiating thoracic dystrophy (Jeune) syndrome: Evaluation and classification of 13 patients. Am J Med Genet A. 2009;149:1727–33. doi: 10.1002/ajmg.a.32962. [DOI] [PubMed] [Google Scholar]
- 9.Digilio MC, Marino B, Giannotti A, Dallapiccola B. Atrioventricular canal defect and postaxial polydactyly indicating phenotypic overlap of Ellis-van Creveld and Kaufman-McKusick syndromes. Pediatr Cardiol. 1997;18:74–5. doi: 10.1007/s002469900116. [DOI] [PubMed] [Google Scholar]
- 10.Howard TD, Guttmacher AE, McKinnon W, Sharma M, McKusick VA, Jabs EW. Autosomal dominant postaxial polydactyly, nail dystrophy, and dental abnormalities map to chromosome 4p16, in the region containing the Ellis-van Creveld syndrome locus. Am J Hum Genet. 1997;61:1405–12. doi: 10.1086/301643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Witkop CJ, Jr, Keenan KM, Cervenka J, Jaspers MT. Taudodontisum: An anomaly of teeth reflecting disruptive developmental homeostasis. Am J Med Gent. 1988;4:85–97. doi: 10.1002/ajmg.1320310513. [DOI] [PubMed] [Google Scholar]
- 12.McWilliam CA, Devlin MF, Joss SK, Koppel DA, Longman C, Ray A, et al. Cleft lip and palate with associated digital and cardiac anomalies: A new dominant orofacial clefting syndrome? Clin Dysmorphol. 2011;20:89–91. doi: 10.1097/MCD.0b013e3283428f60. [DOI] [PubMed] [Google Scholar]
- 13.Vinay C, Sudhakara RR, Uloopi KS, Sekhar R Chandra. Clinical manifestation of Ellis-Van Creveld syndrome. Indian Soc Pedod Prev Dent. 2009;27:256–9. doi: 10.4103/0970-4388.57663. [DOI] [PubMed] [Google Scholar]
- 14.Hunter ML, Roberts GJ. Oral and dental anomalies in Ellis van Creveld syndrome (Chondroectodermal dysplasia): Report of a case. Int J Paediatr Dent. 1998;8:153–7. doi: 10.1046/j.1365-263x.1998.00069.x. [DOI] [PubMed] [Google Scholar]
- 15.Mody P, Garg P, Lall KB. Ellis-van Creveld Syndrome. Indian Pediatr. 1989;26:1046–9. [PubMed] [Google Scholar]
- 16.Hattab FN, Yassin OM, Sasa IS. Oral manifestations of Ellis-van Creveld syndrome: Report of two siblings with unusual dental anomalies. J Clin Pediatr Dent. 1998;22:159–65. [PubMed] [Google Scholar]
- 17.Susami T, Kuroda T, Yoshimasu H, Suzuki R. Ellis- van Creveld syndrome: Craniofacial morphology and multidisciplinary treatment. Cleft Palate Craniofac J. 1999;36:345–52. doi: 10.1597/1545-1569_1999_036_0345_evcscm_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 18.Nestor MS. Perioperative use of antibiotics: Preventing and treating perioperative infections. J Drugs Dermatol. 2005;4(6 suppl):34–6. [PubMed] [Google Scholar]