

Abstract
Background:
Primary spinal primitive neuroectodermal tumors (PNET) and/or spinal extraskeletal Ewing's sarcoma family tumors (ESET) are rare lesions appearing in the spinal extradural space. One hundred forty-one primary spinal PNETs, including 29 intramedullary lesions, have been reported in the literature. Encountering a case of primary epidural EES/peripheral PNET (pPNET) in sacral level, which is the fifth one occurring at this level in the literature, we have tried to conduct a meta-analysis of the reported cases.
Case Description:
A 44-year-old lady with epidural EES/pPNET is reported here. She was once operated for L5/S1 herniated disc, which did not ameliorate her symptoms. The clinical, imaging, surgical, and histopathologic characteristics of our case are presented and wide search of the literature is also done. All the reports were level 3 or less evidences and most of the series had missing parts. 106 cases of primary intraspinal (extradural/extramedullary-intradural) EES/pPNET and 29 cases of primary intramedullary PNET (CNS-PNET) have been reported in the literature. The most common clinical presentation in both entities was muscle weakness proportionate to the tumor location. Distant metastasis occurred in 38 of 99 (38%) cases of primary intraspinal EES/pPNET, while the rate of metastasis was 48% in patients with PNETs occurring in the intramedullary region (P > 0.05). One-year survival rate of the patients who underwent chemo-radiation after total or subtotal resection was better than those who did not receive chemotherapy or radiotherapy, or did not have total or subtotal resection. However, this difference was not repeated in 2-year survival rate in any of the tumor groups.
Conclusion:
It seems that total or subtotal removal of the tumor and adjuvant chemo- and radiation therapy can improve the outcome in these patients.
Keywords: Ewing's sarcoma, primitive neuroectodermal tumor, spine
INTRODUCTION
Primary spinal primitive neuroectodermal tumors (PNET) and/or spinal extraskeletal Ewing's sarcoma family tumors (ESET) are rare lesions appearing in the spinal extradural space.[2,81,116] Undifferentiated round cell tumors include inhomogeneous group of malignant tumors which may arise in any organ because of their embryonic origin. A subgroup of these tumors named “PNET” may affect the CNS primarily.[2,94] The origin of PNET in CNS seems to be the matrix or germinal cells of the embryonic neural tube. The well-known tumor of this subgroup is medulloblastoma which is a primary cerebellar tumor and the most common primary posterior fossa tumor in children, comprising 20% of all the intracranial tumors in this age group.[94] The classification of tumors of CNS published by World Health Organization (WHO) in 1993 designated other cerebral medulloblastoma-like tumors as supratentorial PNET.[33,63,64] In the more recent classification by WHO, these tumors were subdivided under medulloblastoma as CNS-PNETs.[65,76] Even though spine seeding secondary to intracranial medulloblastoma is common, primary spinal intramedullary CNS-PNET occurs rarely[2,81,116] and only 29 cases have been reported in 22 series so far [Table 1]. Among the undifferentiated round cell tumors such as neuroblastoma, non-Hodgkin's lymphoma, and rhabdomyosarcoma, it seems that PNETs have similarities to Ewing's sarcoma (ES).[21,34] ES is one of the childhood tumors mostly affecting skeletal tissues.[93,108] Tefft et al. in 1969 introduced the first case of ES without skeletal involvement,[108] and since then, several cases of extraskeletal ES (EES) have been reported. Osseous ES, EES, Askin's tumor, and peripheral PNET (pPNET) are nowadays generally known as Ewing's sarcoma family tumors (ESFTs).[47,84,109] Occurrence of CNS-PNET (as we call it in our report) or primary intraspinal EES/pPNET (extradural/intradural) in the spine is unusual, and we intend to report our case of EES/pPNET which is the fifth one occurring in the sacral level, describe the clinical presentation, and make a meta-analysis of the reports in the literature.
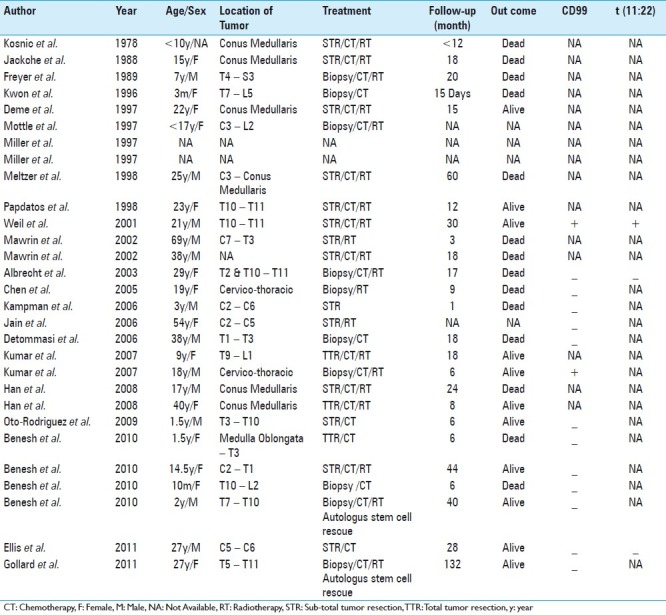
Table 1.
Details of 29 cases of primary spinal intramedullary CNS-primitive neuroectodermal tumors extracted from 22 reports
CASE REPORT
A 44-year-old woman was referred to an orthopedic clinic in a city hospital, complaining of low back pain (LBP) of several years duration. Her severe sciatalgia had exacerbated since 6 months before admission. The diagnosis of L5/S1 disc herniation compressing S1 root on the left side was made and she underwent operation. It was a no-contrast standard lumbosacral magnetic resonance imaging (MRI). At operation, L5 and partial S1 laminectomy followed by bilateral S1 foraminotomy, and bilateral L5/S1 discectomy was performed. Two weeks after the operation, the patient's symptoms exacerbated and paresthesia appeared in the left buttock. Paresthesia of the perineal region and urinary incontinency were also added to her previous complaints. On admission to our department, the muscle forces of the lower limb were intact both proximally and distally, but pin prick sensation was disturbed in S1, S2, and S3 dermatomes, and Achilles tendon reflex was absent in the left side. However, anal sphincter tone was intact. Re-evaluation of the previous preoperative lumbosacral MRI revealed that in addition to the L5/S1 bulged disc, there was an extradural dorsally located mass at S1, S2, and S3 levels. The new contrast-enhanced MRI revealed a 3 × 2 × 2 cm extradurally located tumor, extending from lower edge of S1 down to S2/S3 interspace. The tumor was hypointense in both T1 and T2 images and enhanced homogenously after contrast material injection. Scalloping of the posterior aspect of the S2 vertebra was also detectable [Figure 1a–d]. In the second operation, the previous laminectomy was extended from lower edge of L5 down to S3. A reddish gray tumor located in the extradural space, extending from S1 root axilla down to the S3 root, could be excised totally. There was neither tumor invasion to the dura or intradural space, nor any bone involvement detectable under microscopic observation. Histopathologic examination revealed a highly cellular neoplasm composed of diffuse sheets of tumor cells having monomorphic, round to oval, finely vesicular nuclei and occasional nucleoli with indistinct cytoplasmic border. Delicate fibrovascular septae surrounded the tumor mass along with intra tumoral extensions. In some foci, tumor cells gathered in groups around small vessels (pseudo-rosette appearance). There were nerve bundle entrapments within the tumor nests. Several groups of mitotic figures were noted, but no necrosis was detected [Figure 2a and b].
Figure 1.
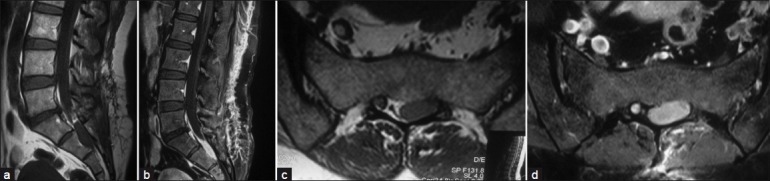
(a) Sagittal T1-W MRI without contrast injection, before the first surgery. An extradural hyposignal lesion is observed at S1–S3 level, which was neglected in the first intervention. (b) Sagittal T1 MRI with contrast from the lumbosacral region after the first operation. Homogenous enhancement of the lesion is observed. (c and d) Axial T1 MRI views of the lesion with and without contrast, after the first operation
Figure 2.
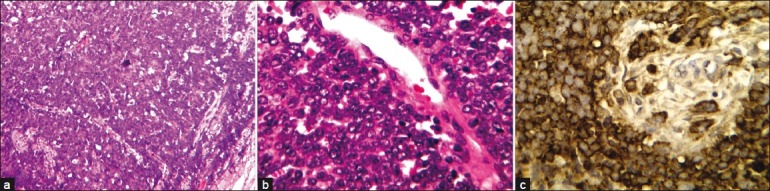
(a and b) Hematoxylin and Eosin staining of the tumor under low- and high-power microscopic fields revealing a highly cellular neoplasm composed of diffuse sheets of tumor cells having monomorphic, round to oval, finely vesicular nuclei and occasional nucleoli with indistinct cytoplasmic border. In some foci, tumor cells are grouped around small vessels (pseudo-rosette appearance). Several groups of mitotic figures were noted, but no necrosis was detected. (c) Immunohistochemistry study for CD99 depicting tumor cells highly positive for the marker
Immunohistochemical (IHC) staining showed that the tumor cells stained positively for neuron-specific enolase, synaptophysin, and chromogranin, suggestive of neuronal differentiation of the tumor. Tumor cells also expressed CD99, consistent with the diagnosis of ES/PNET [Figure 2c]. Ki-67 proliferative index showed about 10–15% proliferative activity. Other markers such as leukocyte common antigen (LCA), epithelial membrane antigen (EMA), cytokeratin (CK), desmin, smooth muscle actin (SMA), and myogenin were negative. Fluorescence in situ hybridization and chromosomal study were not performed.
The postoperative course was uneventful and all her symptoms including radicular pain and sphincter problems improved rapidly. The patient was referred for radiotherapy as the adjuvant therapy. In the last re-evaluation of the patient after 18 months, there was no sign of tumor recurrence in MRI.
Method
Article selection
After our wide search using Tehran University of Medical Sciences electronic resources (www.tums.ac.ir) and motor searches of Pubmed, Ovid, and EBSCO using the key words, spinal primitive neuroectodermal tumor and spinal extraskeletal Ewing sarcoma, 106 abstracts were found in the form of case series and case reports, which reported 141 cases of primary intraspinal EES/pPNET. Full texts of all the articles were collected from different electronic and paper archives including English, French, Spanish, and Italian articles. The earliest articles were published by Smith et al.[106] and Tefft et al.[108] in 1969 and the latest by Gollard et al.[37] in Feb 2011. Patients’ information including age, sex, clinical signs and symptoms, duration of symptoms, family history, location of the tumor, metastasis, recurrences, therapeutic methods, duration of follow-up, and eventual outcome were all extracted from resources. As the articles were reported from various clinical departments (e.g. Neurosurgery, Orthopedics, Radiology, Oncology, Pathology, Pediatrics), different aspects of the disease were reviewed in each, and this led to neglecting some other aspects resulting in missed values regarding some subjects. In some of them with missing data about the mode of therapy, final outcome, or follow-up of the patients, the authors were contacted via e-mail directly for the required information. In spite of sending e-mail to 20 authors, only one reply was received.[89]
Statistical analysis
After collecting and classifying the information, the data were analyzed utilizing SPSS version 13.0.
For analysis of the numeric variables such as age, Kolmogorov–Smirnov test was used to evaluate normal distribution of the data upon which we could decide to utilize parametric versus non-parametric tests to compare the data. Chi-square test (χ2) was used when comparing two nominal or ordinal variables such as 1-year survival in patients receiving different therapies. Independent sample t-test was used to evaluate numerical variable among two populations (e.g. age in different subgroups). P-values less than 0.05 were considered statistically significant.
RESULTS OF THE META-ANALYSIS
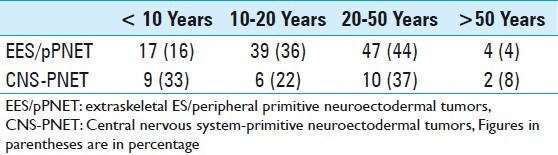
Considering the rarity of primary intraspinal EES/pPNET as a pathologic diagnosis and scarce information on this entity in the references, we decided to review the literature on the issue. By now, 106 cases[1–5,7–9,12–14,16,17,19,23,25–32,36,38,41–50,52–54,56–62,66–68,70,71,73,77–79,81,84,86–90,92,93,95,97–113,115,116] of primary intraspinal EES/pPNET (extradural/intradural extramedullary lesions) and 29 cases[3,11,18,20,22,28,35,37,40,51,52,55,69,71,72,80,82,83,85,91,94,114] of primary intramedullary PNET (CNS-PNET) have been reported in the literature [Tables 1 and 2]. In some studies, neither intra- nor extramedullary location of the tumor was mentioned, so they were not included in any of the groups in our review (i.e. 135 cases out of 141).[10,15,69,96] The average age of occurrence for primary intraspinal EES/pPNET was 22.9 ± 13.9 and for CNS-PNET was 19.5 ± 12.8, and this difference was not statistically significant (χ2, P > 0.05). The youngest and the eldest patients with primary intraspinal EES/pPNET were 40 days and 70 years old, respectively, whereas these age extremes for CNS-PNET patients were 3 months and 69 years. The proportion of primary intraspinal EES/pPNET and CNS-PNET in different age groups is summarized in Table 3. Our case was 41 years old and present in the elder side of the reported cases.
Table 2.
Summary of the cases of primary spinal primitive neuroectodermal tumors-Ewing's sarcoma family tumors reported in the literature
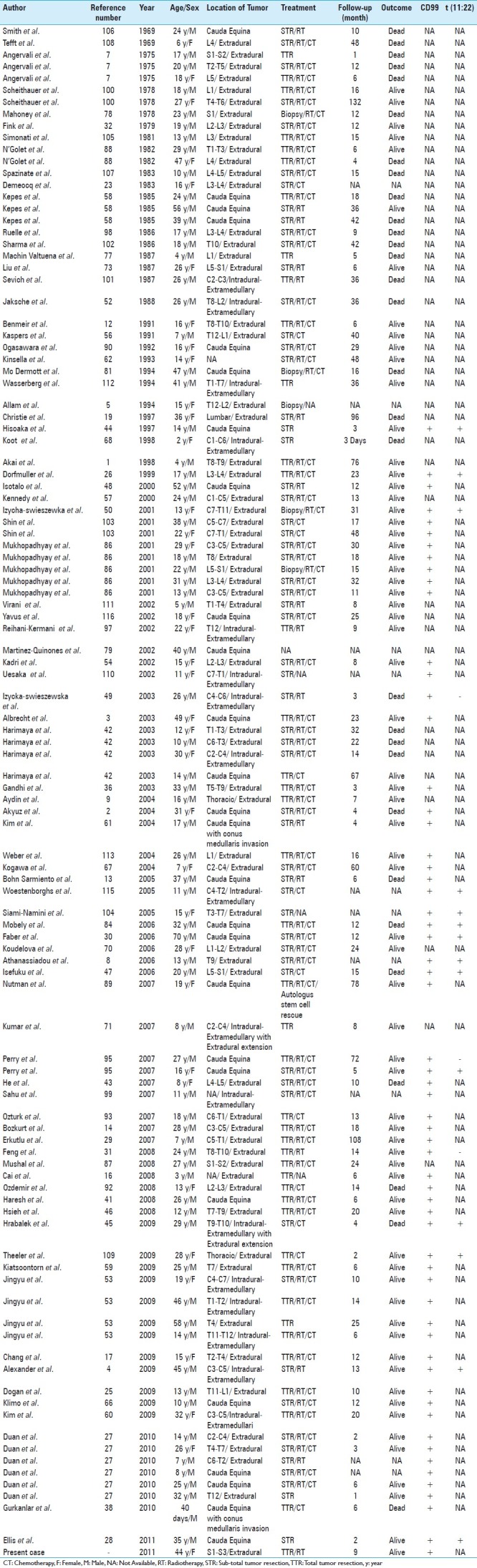
Table 3.
The proportion of primary intra-spinal extraskeletal ES/peripheral primitive neuroectodermal tumors and central nervous system-primitive neuroectodermal tumors in different age groups
Among 107 patients with primary intraspinal EES/pPNET, 71 (66%) were males, whereas of 26 patients with CNS-PNET, 12 (46%) were males and the gender of three patients was unidentified. Duration of symptoms before diagnosis was 4.52 ± 7.01 months and 2.80 ± 3.40 months, respectively, in patients with primary intraspinal EES/pPNET and CNS-PNET. The most common clinical presentation in both entities was muscle weakness proportionate to the tumor location. Other clinical symptoms and their incidences are summarized in Table 4. Our case was a lady complaining of LBP of about 4 years duration, who presented with aggravation of sciatalgia during the previous 6 months and signs compatible with the location of the tumor.
Table 4.
Summarizing the clinical findings of the cases in the two groups

The incidence of primary intraspinal EES/pPNET in lumbar region is twice as much as in thoracic and cervical regions. Only 5% of these tumors have been reported in sacral spine and our case is one of these rare occurrences. On the other hand, CNS-PNET is distributed equally throughout the spine [Table 5]. Distant metastasis occurred in 38 of 99 (38%) cases of primary intraspinal EES/pPNET, while this rate was 12 of 25 (48%) patients with CNS-PNET (χ2, P > 0.05). However, extra-CNS distant metastases were significantly more common in patients with primary intraspinal EES/pPNET [Table 6]. In our case which was an extradural intraspinal EES/pPNET, there has been no evident metastasis in 18 months follow-up.
Table 5.
Demonstrating the distribution of the lesion along the spine

Table 6.
Showing the rate of metastasis in different series

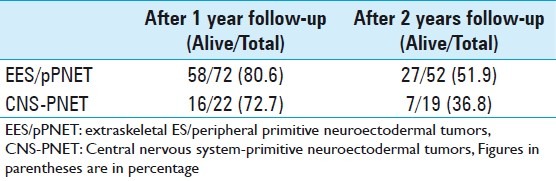
Duration of follow-up for patients with primary intraspinal EES/pPNET and CNS-PNET was 20.5 ± 23.2 and 21.0 ± 23.3 months, respectively, in different series reported in the literature. One-year and 2-year survival rates of the patients (without considering modality of therapy) were not significantly different between the two tumor types (χ2, P > 0.05) [Table 7].
Table 7.
Survival rate in different series
Among the 106 patients with primary intraspinal EES/pPNET who underwent surgery, 5 (5%) had only biopsy taken, 57 (54%) had subtotal, and 44 (41%) had total tumor excision. Eighty patients (78%) with primary intraspinal EES/pPNET had radiotherapy and 77 (75%) received chemotherapy as the adjuvant therapy. Of 27 patients with CNS-PNET, 10 (37%) cases had biopsy, 14 (52%) had subtotal, and 3 (11%) had total tumor resection. Eighteen patients with CNS-PNET (67%) underwent radiotherapy and 23 (85%) had chemotherapy after surgery. Among patients with primary intraspinal EES/pPNET, 64 cases received both radio- and chemotherapies after total/subtotal tumor resection. Fifteen patients with CNS-PNET were managed in a similar way. We managed our case with gross total excision of the tumor and radiotherapy only.
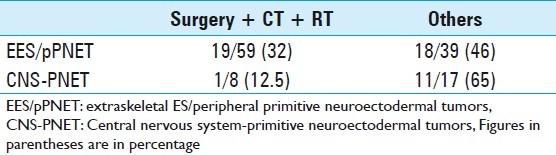
One-year survival rate of the patients who underwent chemo-radiation therapy after total or subtotal resection of the lesion was better than that of those who did not receive chemotherapy or radiotherapy or did not have total or subtotal resection. This difference was statistically significant for patients with CNS-PNET (χ2, P < 0.05) and marginally nonsignificant for primary intraspinal EES/pPNET patients (χ2, P = 0.056). However, this difference was not repeated in 2-year survival rate in any of the tumor groups (χ2, P > 0.05) [Table 8]. Again, combination of chemo-radiation and total/subtotal surgery reduced the rate of distant metastasis in CNS-PNET patients (χ2, P < 0.05) but not in primary intraspinal EES/pPNET group (χ2, P = 0.163) [Table 9]. We undertook radiotherapy as the adjuvant mode of therapy and have not encountered any sign of local recurrence or distant metastasis after 18 months follow-up.
Table 8.
The rate of survival in different groups undergoing adjuvant therapies
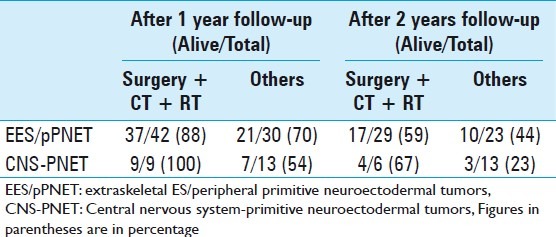
Table 9.
The rate of distant metastasis in different groups
DISCUSSION
Pathology: The occurrence of CNS-PNET and primary intraspinal EES/pPNET in spine is unusual, and if it happens, the pathological distinction is difficult.[89] The authors had adopted the general term of primary spinal PNET or spinal EES before 2000. Advances in the recent decade in cytogenetic and IHC methods have shown chromosomal translocations especially in t(11;22)(q24;q12) gene and CD99 expression to be characteristics for ES, while in CNS-PNET a normal chromosomal arrangement is observed and the tumor cells are negative for CD99 marker.[6,24,39,74,75] In our review, only 75 cases out of 135 patients underwent IHC evaluations for CD99, which were mostly after 2000 [Tables 1 and 2]. All the 61 patients with primary intraspinal EES/pPNET were positive for CD99, but this happened in only 2 of 14 patients with CNS-PNET. Chromosomal studies were performed in only 20 of 135 patients reviewed from the literature [Tables 1 and 2]. Considering these findings, CD99 has a high specificity for primary intraspinal EES/pPNET. This may obviate the need for chromosomal studies, though their application can be complementary. The IHC and CD99 confirmed the presumptive diagnosis in our patient.
Demography: It seems that primary intraspinal EES/pPNET is more prevalent than CNS-PNET in spine as their reported cases were four times more common than CNS-PNET patients. Contrary to the previous belief that primary intraspinal EES/pPNET and CNS-PNET are more common in childhood, our evaluations and analysis showed that less than one-sixth of primary intraspinal EES/pPNET and less than one-third of CNS-PNET occur in children younger than 10 years of age, and they both occur mostly in young adults. Both primary intraspinal EES/pPNET and CNS-PNET occur rarely after 50 years of age. CNS-PNET occurs equally in both sexes, but primary intraspinal EES/pPNET shows a male sex propensity.
Presentation: The most common symptom in both tumor groups is muscle weakness. However, sensory symptoms, local pain, and radiculopathy are more common in primary intraspinal EES/pPNET. The symptoms mimic spinal disc herniation in any case. The same problem happened in our patient who first underwent discectomy while the tumor could hardly be diagnosed on MRI. Although CNS-PNET equally affects spine in different regions, around half of the primary intraspinal EES/pPNET cases happen in lumbar spine. Only five patients with sacral primary intraspinal EES/pPNET have been reported and they were all males. Our case is the first female patient with sacral epidural primary intraspinal EES/pPNET.
Clinical course: Primary intraspinal EES/pPNET and CNS-PNET follow completely different behavior regarding metastasis. Extra CNS metastasis in CNS-PNET is a rare event, while half of the patients developed metastasis to CNS during follow-up, which is the issue comparable with the medulloblastoma patients. Contrarily, CNS metastasis occurs in less than one-fifth of patients with primary intraspinal EES/pPNET, while extra CNS metastasis occurs frequently, with lung being the most common site, followed by the skeletal system. One-year survival is not different between the two tumor groups; however, two-year survival rate is slightly more in patients with primary intraspinal EES/pPNET.
Treatment options: No certain therapeutic protocol has been applied for all the patients with CNS-PNET or primary intraspinal EES/pPNET. This is mostly due to the limited number of the reported cases. Accordingly, primary intraspinal EES/pPNET and CNS-PNET of spine are treated as extraspinal ES and medulloblastoma, respectively. Surgical treatment is necessary to achieve diagnosis and decompression, which is usually followed by improvement of symptoms. Even though adjuvant chemotherapy is proposed both for ES and medulloblastoma, this was not performed in some of the reports mostly due to age limitations, early mortality, or lack of compliance of the patients. Our data analysis shows that chemotherapy improves 1- and 2-year survival rates after total or subtotal tumor resection in both primary intraspinal EES/pPNET and CNS-PNET patients, respectively. This difference was statistically significant only in 1-year survival rate of patients with CNS-PNET. Adjuvant chemotherapy may reduce CNS metastasis in cases with CNS-PNET [Table 9].
Prognosis: Primary intraspinal EES/pPNET and CNS-PNET are both aggressive malignant tumors leading to mortality within 2 years after diagnosis in nearly half and two-thirds of the patients, respectively. Age is one of the important prognostic factors in both tumors as survival reduces at both age extremes. However, survival did not show any differences regarding gender of the patients. It seems that total or subtotal tumor resection combined with both radiation and chemotherapy improves the outcome of the patients significantly.
CONCLUSION
The reported cases of undifferentiated small round cell tumors in the spine have increased in number in recent years. Our review and analysis showed that CNS-PNET and EES/pPNET of spine have different clinical courses, necessitating further histopathologic evaluations including that of CD99 and t(11;22)(q24;q12) to distinguish these entities from each other. Tumor location is an important clue in differentiating the two, as CNS-PNETs are mostly intramedullary in contrast with EES/pPNETs which are often extramedullary.
Due to limited evidence regarding the therapeutic aspects of these tumors, no definite protocol can be formulated for their treatment and the best mode of therapy should be individualized for each case. However, our review supports the fact that total/subtotal tumor removal followed by adjuvant chemo-radiation is associated with the best clinical outcome.
Future studies should mainly focus on finding evidences denoting the best treatment strategies for these tumors. Autologous stem cell rescue besides adjuvant chemotherapy has been associated with prolonged survival in some reports,[27,29,72] which can be the matter of further investigation in the future.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2012/3/1/55/96154
Contributor Information
Saeed Saeedinia, Email: saeediniasaeed@yahoo.com.
Mohsen Nouri, Email: m_nouri01@yahoo.com.
Meysam Alimohammadi, Email: m_alimohamadi@yahoo.com.
Hedieh Moradi, Email: hedieh_moradi@yahoo.com.
Abbas Amirjamshidi, Email: abamirjamshidi@yahoo.com.
REFERENCES
- 1.Akai T, Iizuka H, Kadaya S, Nojima T, Kohno M. Primitive neuroectodermal tumor in the spinal epidural space: Case report. Neurol Med Chir (Tokyo) 1998;38:508–11. doi: 10.2176/nmc.38.508. [DOI] [PubMed] [Google Scholar]
- 2.Akyüz M, Demiral AN, Gürer IE, Uçar T, Tuncer R. Primary primitive neuro-ectodermal tumor of cauda equina with intracranial seeding. Acta Neurochir (Wien) 2004;146:525–8. doi: 10.1007/s00701-003-0212-1. [DOI] [PubMed] [Google Scholar]
- 3.Albrecht CF, Weiss E, Schulz-Schaeffer WJ, Albrecht T, Fauser S, Wickboldt J, et al. Primary intraspinal primitive neuroectodermal tumor: Report of two cases and review of the literature. J Neurooncol. 2003;61:113–20. doi: 10.1023/a:1022118317876. [DOI] [PubMed] [Google Scholar]
- 4.Alexander HS, Koleda C, Hunn MK. Peripheral Primitive Neuroectodermal Tumor (pPNET) in the cervical spine. J Clin Neurosci. 2010;17:259–61. doi: 10.1016/j.jocn.2009.05.020. [DOI] [PubMed] [Google Scholar]
- 5.Allam K, Sze G. MR of primary extraosseous Ewing sarcoma. AJNR Am J Neuroradiol. 1994;15:305–7. [PMC free article] [PubMed] [Google Scholar]
- 6.Ambros IM, Ambros PF, Strehl S, Kovar H, Gadner H, Salzer-Kuntschik M. MIC2 is a specific marker for Ewing's sarcoma and peripheral primitive neuroectodermal tumors. Evidence for a common histogenesis of Ewing's sarcoma and peripheral primitive neuroectodermal tumors from MIC2 expression and specific chromosome aberration. Cancer. 1991;67:1886–93. doi: 10.1002/1097-0142(19910401)67:7<1886::aid-cncr2820670712>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 7.Angervall L, Enzinger FM. Extraskeletal neoplasm resembling Ewing's sarcoma. Cancer. 1975;36:240–51. doi: 10.1002/1097-0142(197507)36:1<240::aid-cncr2820360127>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 8.Athanassiadou F, Tragiannidis A, Kourti M, Papageorgiou T, Kotoula V, Kontopoulos V, et al. Spinal epidural extraskeletal Ewing sarcoma in an adolescent boy: A case report. Pediatr Hematol Oncol. 2006;23:263–7. doi: 10.1080/08880010500506297. [DOI] [PubMed] [Google Scholar]
- 9.Aydin MV, Sen O, Ozel S, Kayaselcuk F, Caner H, Altinors N. Primary primitive neuroectodermal tumor within the spinal epidural space: Report of a case and review of the literature. Neurol Res. 2004;26:774–7. doi: 10.1179/016164104225014111. [DOI] [PubMed] [Google Scholar]
- 10.Baum ES, Morgan ER, Dal Centro MC, West PM. Review of experience with primitive neuroectodermal tumors of childhood. In: Humphrey GB, Dehner LP, editors. Pediatric Oncology 1. The Hague: Martinus Nijhoff; 1981. pp. 239–42. [Google Scholar]
- 11.Benesch M, Sperl D, von Bueren AO, Schmid I, von Hoff K, Warmuth-Metz M, et al. Primary central nervous system primitive neuroectodermal tumors (CNS-PNETs) of the spinal cord in children: Four cases from the German HIT database with a critical review of the literature. J Neurooncol. 2011;104:279–86. doi: 10.1007/s11060-010-0485-1. [DOI] [PubMed] [Google Scholar]
- 12.Benmeir P, Sagi A, Hertzanu Y, Zirkin H, Rosenberg L, Peiser J, et al. Primary and secondary spinal epidural extraskeletal Ewing's sarcoma. Report of two cases and review of the literature. Spine (Phila Pa 1976) 1991;16:224–7. [PubMed] [Google Scholar]
- 13.Bohn Sarmiento U, Aguiar Bujanda D, Camacho Galán R, Rivero Vera JC, Aguiar Morales J. Lumbar region intra-spinal primitive neuroectodermal tumor (PNET) combined with neurofibromatosis type 1. Clin Transl Oncol. 2005;7:464–7. doi: 10.1007/BF02716598. [DOI] [PubMed] [Google Scholar]
- 14.Bozkurt G, Ayhan S, Turk CC, Akbay A, Soylemezoglu F, Palaoglu S. Primary extraosseous Ewing sarcoma of the cervical epidural space. Case illustration. J Neurosurg Spine. 2007;6:192. doi: 10.3171/spi.2007.6.2.192. [DOI] [PubMed] [Google Scholar]
- 15.Bruno LA, Rorke LB, Norris DG. Primitive neuroectodermal tumors of infancy and childhood. In: Humphrey GB, Dehner LP, editors. Pediatric Oncology 1. The Hague: Martinus Nijhoff; 1981. pp. 265–7. [Google Scholar]
- 16.Cai C, Zhang Q, Shen C, Hu X. Primary intraspinal primitive neuroectodermal tumor: A case report and review of literature. J Pediatr Neurosci. 2008;3:154–6. [Google Scholar]
- 17.Chang SI, Tsai MC, Tsai MD. An unusual primitive neuroectodermal tumor in the thoracic epidural space. J Clin Neurosci. 2010;17:261–3. doi: 10.1016/j.jocn.2009.05.018. [DOI] [PubMed] [Google Scholar]
- 18.Chen YC, Tang LM, Chen CJ, Jung SM, Chen ST. Intracranial hypertension as an initial manifestation of spinal neuroectodermal tumor. Clin Neurol Neurosurg. 2005;107:408–11. doi: 10.1016/j.clineuro.2004.09.011. [DOI] [PubMed] [Google Scholar]
- 19.Christie DR, Bilous AM, Carr PJ. Diagnostic difficulties in extraosseous Ewing's sarcoma: A proposal for diagnostic criteria. Australas Radiol. 1997;41:22–8. doi: 10.1111/j.1440-1673.1997.tb00463.x. [DOI] [PubMed] [Google Scholar]
- 20.De Tommasi A, De Tommasi C, Occhiogrosso G, Cimmino A, Parisi M, Sanguedolce F, et al. Primary intramedullary primitive neuroectodermal tumor (PNET): Case report and review of the literature. Eur J Neurol. 2006;13:240–3. doi: 10.1111/j.1468-1331.2006.01183.x. [DOI] [PubMed] [Google Scholar]
- 21.Delattre O, Zucman J, Melot T, Garau XS, Zucker JM, Lenoir GM, et al. The Ewing family of tumors--A subgroup of smallround-cell tumors defined by specific chimeric transcripts. N Engl J Med. 1994;331:294–9. doi: 10.1056/NEJM199408043310503. [DOI] [PubMed] [Google Scholar]
- 22.Deme S, Ang LC, Skaf G, Rowed DW. Primary intramedullary primitive neuroectodermal tumor of the spinal cord: Case report and review of the literature. Neurosurgery. 1997;41:1417–20. doi: 10.1097/00006123-199712000-00040. [DOI] [PubMed] [Google Scholar]
- 23.Demeocq F, Fonck Y, Legros M, Chazal J, Plagne R, Dauplat J. Extraskeletal Ewing's sarcoma. Anatomo-clinical study of a new case. Pediatrie. 1983;38:475–8. (Article in French) [PubMed] [Google Scholar]
- 24.Dierick AM, Roels H, Langlois M. The immunophenotype of Ewing's sarcoma. An immunohistochemical analysis. Pathol Res Pract. 1993;189:26–32. doi: 10.1016/S0344-0338(11)80113-5. [DOI] [PubMed] [Google Scholar]
- 25.Dogan S, Leković GP, Theodore N, Horn EM, Eschbacher J, Rekate HL. Primary thoracolumbar Ewing's sarcoma presenting as isolated epidural mass. Spine (Phila Pa 1976) 2009;9:9–14. doi: 10.1016/j.spinee.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 26.Dorfmüller G, Würtz FG, Umschaden HW, Kleinert R, Ambros PF. Intraspinal primitive neuroectodermal tumor: Report of two cases and review of the literature. Acta Neurochir (Wien) 1999;141:1169–75. doi: 10.1007/s007010050414. [DOI] [PubMed] [Google Scholar]
- 27.Duan XH, Ban XH, Liu B, Zhong XM, Guo RM, Zhang F, et al. Intraspinal primitive neuroectodermal tumor: Imaging findings in six cases. Eur J Radiol. 2011;80:426–31. doi: 10.1016/j.ejrad.2010.06.005. [DOI] [PubMed] [Google Scholar]
- 28.Ellis JA, Rothrock RJ, Moise G, McCormick PC, 2nd, Tanji K, Canoll P, et al. Primitive neuroectodermal tumors of the spine: A comprehensive review with illustrative clinical cases. Neurosurg Focus. 2011;30:E1. doi: 10.3171/2010.10.FOCUS10217. [DOI] [PubMed] [Google Scholar]
- 29.Erkutlu I, Buyukhatipoglu H, Alptekin M, Ozsarac C, Buyukbese I, Gok A. Primary spinal epidural extraosseous Ewing's sarcoma mimicking a spinal abscess. Pediatr Hematol Oncol. 2007;24:537–42. doi: 10.1080/08880010701534163. [DOI] [PubMed] [Google Scholar]
- 30.Fabre E, Guillevin R, Chretien F, Le Guerinel C, Duffau H. Peripheral primitive neuroectodermal tumor of the cauda equina in an elderly patient. Case report. J Neurosurg Spine. 2006;5:68–71. doi: 10.3171/spi.2006.5.1.68. [DOI] [PubMed] [Google Scholar]
- 31.Feng JF, Liang YM, Bao YH, Pan YH, Jiang JY. Multiple primary primitive neuroectodermal tumors within the spinal epidural space with non-concurrent onset. J Int Med Res. 2008;36:366–70. doi: 10.1177/147323000803600222. [DOI] [PubMed] [Google Scholar]
- 32.Fink LH, Meriwether MW. Primary epidural Ewing's sarcoma presenting as a lumbar disc protrusion. Case report. J Neurosurg. 1979;51:120–3. doi: 10.3171/jns.1979.51.1.0120. [DOI] [PubMed] [Google Scholar]
- 33.Fletcher CD, Unni KK, Mertens F. World Health Organization Classification of Tumors: Pathology and Genetics of Tumors of Soft Tissue and Bone. Lyon: IARC Press; 2002. [Google Scholar]
- 34.Folpe AL, Goldblum JR, Rubin BP, Shehata BM, Liu W, Dei Tos AP, et al. Morphologic and immunophenotypic diversity in Ewing family tumors: A study of 66 genetically confirmed cases. Am J Surg Pathol. 2005;29:1025–33. [PubMed] [Google Scholar]
- 35.Freyer DR, Hutchinson RJ, McKeever PE. Primary primitive neuroectodermal tumor of the spinal cord associated with neural tube defect. Pediatr Neurosci. 1989;15:181–7. doi: 10.1159/000120466. [DOI] [PubMed] [Google Scholar]
- 36.Gandhi D, Goyal M, Belanger E, Modha A, Wolffe J, Miller W. Primary epidural Ewing's sarcoma: Case report and review of literature. Can Assoc Radiol J. 2003;54:109–13. [PubMed] [Google Scholar]
- 37.Gollard RP, Rosen L, Anson J, Mason J, Khoury J. Intramedullary PNET of the spine: Long-term survival after combined modality therapy and subsequent relapse. J Pediatr Hematol Oncol. 2011;33:107–12. doi: 10.1097/MPH.0b013e3181f84b7f. [DOI] [PubMed] [Google Scholar]
- 38.Gurkanlar D, Korkmaz E, Gurler IE, Gokhan G, Kazan S. Multilevel primary intraspinal PNETs in an infant associated with hydrocephalus. Turk Neurosurg. 2010;20:82–5. [PubMed] [Google Scholar]
- 39.Gyure KA, Prayson RA, Estes ML. Extracerebellar primitive neuroectodermal tumors: A clinicopathologic study with bcl-2 and CD99 immunohistochemistry. Ann Diagn Pathol. 1999;3:276–80. doi: 10.1016/s1092-9134(99)80022-7. [DOI] [PubMed] [Google Scholar]
- 40.Han IH, Kuh SU, Chin DK, Kim KS, Jin BH, Cho YE. Surgical treatment of primary spinal tumors in the conus medullaris. J Korean Neurosurg Soc. 2008;44:72–7. doi: 10.3340/jkns.2008.44.2.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Haresh KP, Chinikkatti SK, Prabhakar R, Rishi A, Rath GK, Sharma DN, et al. A rare case of intradural extramedullary Ewing's sarcoma with skip metastasis in the spine. Spinal Cord. 2008;46:582–4. doi: 10.1038/sc.2008.8. [DOI] [PubMed] [Google Scholar]
- 42.Harimaya K, Oda Y, Matsuda S, Tanaka K, Chuman H, Iwamoto Y. Primitive neuroectodermal tumor and extraskeletal Ewing sarcoma arising primarily around the spinal column: Report of four cases and a review of the literature. Spine (Phila Pa 1976) 2003;28:E408–12. doi: 10.1097/01.BRS.0000085099.47800.DF. [DOI] [PubMed] [Google Scholar]
- 43.He SS, Zhao J, Han KW, Hou TS, Hussain N, Zhang SM. Primitive neuroectodermal tumor of lumbar spine: Case report. Chin Med J (Engl) 2007;120:844–6. [PubMed] [Google Scholar]
- 44.Hisaoka M, Hashimoto H, Murao T. Peripheral primitive neuroectodermal tumor with ganglioneuroma-like areas arising in the cauda equina. Virchows Arch. 1997;431:365–9. doi: 10.1007/s004280050112. [DOI] [PubMed] [Google Scholar]
- 45.Hrabálek L, Kalita O, Svebisova H, Ehrmann J, Jr, Hajduch M, Trojanec R, et al. Dumbbell-shaped peripheral primitive neuroectodermal tumor of the spine: Case report and review of the literature. J Neurooncol. 2009;92:211–7. doi: 10.1007/s11060-008-9744-9. [DOI] [PubMed] [Google Scholar]
- 46.Hsieh CT, Chiang YH, Tsai WC, Sheu LF, Liu MY. Primary spinal epidural Ewing sarcoma: A case report and review of the literature. Turk J Pediatr. 2008;50:282–6. [PubMed] [Google Scholar]
- 47.Isefuku S, Seki M, Tajino T, Hakozaki M, Asano S, Hojo H, et al. Ewing's sarcoma in the spinal nerve root: A case report and review of the literature. Tohoku J Exp Med. 2006;209:369–77. doi: 10.1620/tjem.209.369. [DOI] [PubMed] [Google Scholar]
- 48.Isotalo PA, Agbi C, Davidson B, Girard A, Verma S, Robertson SJ. Primary primitive neuroectodermal tumor of the cauda equina. Hum Pathol. 2000;31:999–1001. doi: 10.1053/hupa.2000.16532. [DOI] [PubMed] [Google Scholar]
- 49.Izycka-Swieszewska E, Debiec-Rychter M, Wasag B, Wozniak A, Gasecki D, Plata-Nazar K, et al. A unique occurrence of a cerebral atypical teratoid/rhabdoid tumor in an infant and a spinal canal primitive neuroectodermal tumor in her father. J Neurooncol. 2003;61:219–25. doi: 10.1023/a:1022532727436. [DOI] [PubMed] [Google Scholar]
- 50.Izycka-Swieszewska E, Stefanowicz J, Debiec-Rychter M, Rzepko R, Borowska-Lehman J. Peripheral primitive neuroectodermal tumor within the spinal epidural space. Neuropathology. 2001;21:218–21. doi: 10.1046/j.1440-1789.2001.00387.x. [DOI] [PubMed] [Google Scholar]
- 51.Jain A, Jalali R, Nadkarni TD, Sharma S. Primary intramedullary primitive neuroectodermal tumor of the cervical spinal cord. Case report. J Neurosurg Spine. 2006;4:497–502. doi: 10.3171/spi.2006.4.6.497. [DOI] [PubMed] [Google Scholar]
- 52.Jaksche H, Wöckel W, Wernert N. Primary spinal medulloblastomas? Neurosurg Rev. 1988;11:259–65. doi: 10.1007/BF01741419. [DOI] [PubMed] [Google Scholar]
- 53.Jingyu C, Jinning S, Hui M, Hua F. Intraspinal primitive neuroectodermal tumors: Report of four cases and review of the literature. Neurol India. 2009;57:661–8. doi: 10.4103/0028-3886.57804. [DOI] [PubMed] [Google Scholar]
- 54.Kadri PA, Mello PM, Olivera JG, Braga FM. Primary lumbar epidural Ewing's sarcoma: Case report. Arq Neuropsiquiatr. 2002;60:145–9. doi: 10.1590/s0004-282x2002000100027. (Article in Portuguese) [DOI] [PubMed] [Google Scholar]
- 55.Kampman WA, Kros JM, De Jong TH, Lequin MH. Primitive neuroectodermal tumors (PNETs) located in the spinal canal: The relevance of classification as central or peripheral PNET: Case report of a primary spinal PNET occurrence with a critical literature review. J Neurooncol. 2006;77:65–72. doi: 10.1007/s11060-005-9006-z. [DOI] [PubMed] [Google Scholar]
- 56.Kaspers GJ, Kamphorst W, van de Graaff M, van Alphen HA, Veerman AJ. Primary spinal epidural extraosseous Ewing's sarcoma. Cancer. 1991;68:648–54. doi: 10.1002/1097-0142(19910801)68:3<648::aid-cncr2820680335>3.0.co;2-q. [DOI] [PubMed] [Google Scholar]
- 57.Kennedy JG, Eustace S, Caulfield R, Fennelly DJ, Hurson B, O’Rourke KS. Extraskeletal Ewing's sarcoma: A case report and review of the literature. Spine (Phila Pa 1976) 2000;25:1996–9. doi: 10.1097/00007632-200008010-00022. [DOI] [PubMed] [Google Scholar]
- 58.Kepes JJ, Belton K, Roessmann U, Ketcherside WJ. Primitive neuroectodermal tumors of the cauda equina in adults with no detectable primary intracranial neoplasm--Three case studies. Clin Neuropathol. 1985;4:1–11. [PubMed] [Google Scholar]
- 59.Kiatsoontorn K, Takami T, Ichinose T, Chokyu I, Tsuyuguchi N, Ohsawa M, et al. Primary epidural peripheral primitive neuroectodermal tumor of the thoracic spine. Neurol Med Chir (Tokyo) 2009;49:542–5. doi: 10.2176/nmc.49.542. [DOI] [PubMed] [Google Scholar]
- 60.Kim SW, Shin H. Primary intradural extraosseous Ewing's sarcoma. J Korean Neurosurg Soc. 2009;45:179–81. doi: 10.3340/jkns.2009.45.3.179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Kim YW, Jin BH, Kim TS, Cho YE. Primary intraspinal primitive neuroectodermal tumor at conus medullaris. Yonsei Med J. 2004;45:533–8. doi: 10.3349/ymj.2004.45.3.533. [DOI] [PubMed] [Google Scholar]
- 62.Kinsella TJ. Extraskeletal Ewing's sarcoma. J Clin Oncol. 1993;1:489. doi: 10.1200/JCO.1983.1.8.489. [DOI] [PubMed] [Google Scholar]
- 63.Kleihues P, Burger PC, Scheithauer BW. The new WHO classification of brain tumors. Brain Pathol. 1993;3:255–68. doi: 10.1111/j.1750-3639.1993.tb00752.x. [DOI] [PubMed] [Google Scholar]
- 64.Kleihues P, Cavenee WK. World Health Organization Classification of Tumors: Pathology and Genetics: Tumors of the Nervous System. Lyon: IARC Press; 1997. [Google Scholar]
- 65.Kleihues P, Cavenee WK. World Health Organization Classification of Tumors: Pathology and Genetics: Tumors of the Nervous System. 2nd ed. Lyon: IARC Press; 2000. [Google Scholar]
- 66.Klimo P, Jr, Codd PJ, Grier H, Goumnerova LC. Primary pediatric intraspinal sarcomas. Report of 3 cases. J Neurosurg Pediatr. 2009;4:222–9. doi: 10.3171/2009.3.PEDS08272. [DOI] [PubMed] [Google Scholar]
- 67.Kogawa M, Asazuma T, Iso K, Koike Y, Domoto H, Aida S, et al. Primary cervical spinal epidural Extra-osseous Ewing's sarcoma. Acta Neurochir (Wien) 2004;146:1051–3. doi: 10.1007/s00701-004-0294-4. [DOI] [PubMed] [Google Scholar]
- 68.Koot RW, Henneveld HT, Albrecht KW. [Two children with unusual causes of torticollis: Primitive neuroectodermal tumor and Grisel's syndrome.] Ned Tijdschr Geneeskd. 1998;142:1030–3. (Article in Dutch) [PubMed] [Google Scholar]
- 69.Kosnik EJ, Boesel CP, Bay J, Sayers MP. Primitive neuroectodermal tumors of the central nervous system in children. J Neurosurg. 1978;48:741–6. doi: 10.3171/jns.1978.48.5.0741. [DOI] [PubMed] [Google Scholar]
- 70.Koudelová J, Kunesová M, Koudela K, Jr, Matejka J, Novák P, Prausová J. [Peripheral primitive neuroectodermal tumor--PNET.] Acta Chir Orthop Traumatol Cech. 2006;73:39–44. (Article in Czech) [PubMed] [Google Scholar]
- 71.Kumar R, Reddy SJ, Wani AA, Pal L. Primary spinal primitive neuroectodermal tumor: Case series and review of the literature. Pediatr Neurosurg. 2007;43:1–6. doi: 10.1159/000097517. [DOI] [PubMed] [Google Scholar]
- 72.Kwon OK, Wang KC, Kim CJ, Kim IO, Chi JG, Cho BK. Primary intramedullary spinal cord primitive neuroectodermal tumor with intracranial seeding in an infant. Childs Nerv Syst. 1996;12:633–6. doi: 10.1007/BF00261661. [DOI] [PubMed] [Google Scholar]
- 73.Liu HM, Yang WC, Garcia RL, Noh JM, Malhotra V, Leeds NE. Intraspinal primitive neuroectodermal tumor arising from the sacral spinal nerve root. J Comput Tomogr. 1987;11:350–4. doi: 10.1016/0149-936x(87)90071-3. [DOI] [PubMed] [Google Scholar]
- 74.Llombart-Bosch A, Machado I, Navarro S, Bertoni F, Bacchini P, Alberghini M, et al. Histological heterogeneity of Ewing's sarcoma/PNET: An immunohistochemical analysis of 415 genetically confirmed cases with clinical support. Virchows Arch. 2009;455:397–411. doi: 10.1007/s00428-009-0842-7. [DOI] [PubMed] [Google Scholar]
- 75.Llombart-Bosch A, Navarro S. Immunohistochemical detection of EWS and FLI-1 proteins in Ewing sarcoma and primitive neuroectodermal tumors: Comparative analysis with CD99 (MIC-2) expression. Appl Immunohistochem Mol Morphol. 2001;9:255–60. doi: 10.1097/00129039-200109000-00010. [DOI] [PubMed] [Google Scholar]
- 76.Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. WHO Classification of Tumors of the Central Nervous System. 4th ed. Lyon: IARC; 2007. [Google Scholar]
- 77.Machin Valtueña M, Garcia-Sagredo JM, Muñoz Villa A, Lozano Giménez C, Aparicio Meix JM. 18q-syndrome and extraskeletal Ewing's sarcoma. J Med Genet. 1987;24:426–8. doi: 10.1136/jmg.24.7.426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Mahoney JP, Ballinger WE, Jr, Alexander RW. So-called extraskeletal Ewing's sarcoma. Report of a case with ultrastructural analysis. Am J Clin Pathol. 1978;70:926–31. doi: 10.1093/ajcp/70.6.926. [DOI] [PubMed] [Google Scholar]
- 79.Martínez-Quiñones JV, de Antonio A, Hernandez G, Moratinos P, Hijosa M. Primitive neuroectodermal tumor of the cauda equina. Report of a case. Neurocirugia (Astur) 2002;13:46–9. doi: 10.1016/s1130-1473(02)70651-9. (Article in Spanish) [DOI] [PubMed] [Google Scholar]
- 80.Mawrin C, Synowitz HJ, Kirches E, Kutz E, Dietzmann K, Weis S. Primary primitive neuroectodermal tumor of the spinal cord: Case report and review of the literature. Clin Neurol Neurosurg. 2002;104:36–40. doi: 10.1016/s0303-8467(01)00171-8. [DOI] [PubMed] [Google Scholar]
- 81.McDermott VG, el-Jabbour JN, Sellar RJ, Bell J. Primitive neuroectodermal tumor of the cauda equina. Neuroradiology. 1994;36:228–30. doi: 10.1007/BF00588138. [DOI] [PubMed] [Google Scholar]
- 82.Meltzer CC, Townsend DW, Kottapally S, Jadali F. FDG imaging of spinal cord primitive neuroectodermal tumor. J Nucl Med. 1998;39:1207–9. [PubMed] [Google Scholar]
- 83.Miller DC, Rorke LB, Weinberg J, Allen JC, Epstein FJ. Histopathologic diagnoses of intramedullary spinal cord tumors in children. J Neuropathol Exp Neurol. 1997;56:607. [Google Scholar]
- 84.Mobley BC, Roulston D, Shah GV, Bijwaard KE, McKeever PE. Peripheral primitive neuroectodermal tumor/Ewing's sarcoma of the craniospinal vault: Case reports and review. Hum Pathol. 2006;37:845–53. doi: 10.1016/j.humpath.2006.02.011. [DOI] [PubMed] [Google Scholar]
- 85.Mottl H, Koutecky J. Treatment of spinal cord tumors in children. Med Pediatr Oncol. 1997;29:293–5. doi: 10.1002/(sici)1096-911x(199710)29:4<293::aid-mpo10>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 86.Mukhopadhyay P, Gairola M, Sharma M, Thulkar S, Julka P, Rath G. Primary spinal epidural extraosseous Ewing's sarcoma: Report of five cases and literature review. Australas Radiol. 2001;45:372–9. doi: 10.1046/j.1440-1673.2001.00942.x. [DOI] [PubMed] [Google Scholar]
- 87.Musahl V, Rihn JA, Fumich FE, Kang JD. Sacral intraspinal extradural primitive neuroectodermal tumor. Spine J. 2008;8:1024–9. doi: 10.1016/j.spinee.2007.04.001. [DOI] [PubMed] [Google Scholar]
- 88.N’Golet A, Pasquier B, Pasquier D, Lachard A, Couderc P. Extraskeletal Ewing's sarcoma of the epidural space. A report of two new cases with literature review (author's transl) Arch Anat Cytol Pathol. 1982;30:10–3. (Article in French) [PubMed] [Google Scholar]
- 89.Nutman A, Postovsky S, Zaidman I, Elhasid R, Vlodavsky E, Kreiss Y, et al. Primary intraspinal primitive neuroectodermal tumor treated with autologous stem cell transplantation: Case report and review of the literature. Pediatr Hematol Oncol. 2007;24:53–61. doi: 10.1080/08880010601001396. [DOI] [PubMed] [Google Scholar]
- 90.Ogasawara H, Kiya K, Kurisu K, Muttaqin Z, Uozumi T, Sugiyama K, et al. Intracranial metastasis from a spinal cord primitive neuroectodermal tumor: Case report. Surg Neurol. 1992;37:307–12. doi: 10.1016/0090-3019(92)90158-j. [DOI] [PubMed] [Google Scholar]
- 91.Otero-Rodríguez A, Hinojosa J, Esparza J, Muñoz MJ, Iglesias S, Rodríguez-Gil Y, et al. Purely intramedullary spinal cord primitive neuroectodermal tumor: Case report and review of the literature. Neurocirugia (Astur) 2009;20:381–7. doi: 10.1016/s1130-1473(09)70159-9. [DOI] [PubMed] [Google Scholar]
- 92.Ozdemir N, Usta G, Minoglu M, Erbay AM, Bezircioglu H, Tunakan M. Primary primitive neuroectodermal tumor of the lumbar extradural space. J Neurosurg Pediatr. 2008;2:215–21. doi: 10.3171/PED/2008/2/9/215. [DOI] [PubMed] [Google Scholar]
- 93.Ozturk E, Mutlu H, Sonmez G, Vardar Aker F, Cinar Basekim C, Kizilkaya E. Spinal epidural extraskeletal Ewing sarcoma. J Neuroradiol. 2007;34:63–7. doi: 10.1016/j.neurad.2007.01.009. [DOI] [PubMed] [Google Scholar]
- 94.Papadatos D, Albrecht S, Mohr G, del Carpio-O’Donovan R. Exophytic primitive neuroectodermal tumor of the spinal cord. AJNR Am J Neuroradiol. 1998;19:787–9. [PMC free article] [PubMed] [Google Scholar]
- 95.Perry R, Gonzales I, Finlay J, Zacharoulis S. Primary peripheral primitive neuroectodermal tumors of the spinal cord: Report of two cases and review of the literature. J Neurooncol. 2007;81:259–64. doi: 10.1007/s11060-006-9178-1. [DOI] [PubMed] [Google Scholar]
- 96.Priest J, Dehner LP, Sung JH, Nesbit ME. Primitive neuroectodermal tumors. Embryonal gliomas of childhood. A clinicopathologic study of 12 cases. In: Humphrey GB, Dehner LP, editors. Pediatric oncology. The Hague: Martinus Nijhoff; 1981. pp. 247–64. [Google Scholar]
- 97.Reihani-Kermani H, Amizadeh B. Primary intraspinal primitive neuroectodermal tumors: Report of a case. Arch Iran Med. 2002;5:262–6. [Google Scholar]
- 98.Ruelle A, Boccardo M. Epidural extraskeletal Ewing's sarcoma simulating a herniated disk. Clinical case. Riv Neurol. 1986;56:183–8. (Article in Italian) [PubMed] [Google Scholar]
- 99.Sahu JK, Seth R, Karak A, Thavaraj V, Kabra SK. Primitive neuroectodermal tumor presenting as cauda equina syndrome. Indian J Med Paediatr Oncol. 2007;28:34–7. [Google Scholar]
- 100.Scheithauer BW, Egbert BM. Ewing's sarcoma of the spinal epidural space: Report of two cases. J Neurol Neurosurg Psychiatry. 1978;41:1031–5. doi: 10.1136/jnnp.41.11.1031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Sevick RJ, Johns RD, Curry BJ. Primary spinal primitive neuroectodermal tumor with extraneural metastases. AJNR Am J Neuroradiol. 1987;8:1151–2. [PMC free article] [PubMed] [Google Scholar]
- 102.Sharma BS, Khosla VK, Banerjee AK. Primary spinal epidural Ewing's sarcoma. Clin Neurol Neurosurg. 1986;88:299–302. doi: 10.1016/s0303-8467(86)80050-6. [DOI] [PubMed] [Google Scholar]
- 103.Shin JH, Lee HK, Rhim SC, Cho KJ, Choi CG, Suh DC. Spinal epidural extraskeletal Ewing sarcoma: MR findings in two cases. AJNR Am J Neuroradiol. 2001;22:795–8. [PMC free article] [PubMed] [Google Scholar]
- 104.Siami-Namini K, Shuey-Drake R, Wilson D, Francel P, Perry A, Fung KM. A 15-year-old female with progressive myelopathy. Brain Pathol. 2005;15:265–7. doi: 10.1111/j.1750-3639.2005.tb00531.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Simonati A, Vio M, Iannucci AM, Bricolo A, Rizzuto N. Lumbar epidural Ewing sarcoma. Light and electron microscopic investigation. J Neurol. 1981;225:67–72. doi: 10.1007/BF00313464. [DOI] [PubMed] [Google Scholar]
- 106.Smith DR, Hardman JM, Earle KM. Metastasizing neuroectodermal tumors of the central nervous system. J Neurosurg. 1969;31:50–8. doi: 10.3171/jns.1969.31.1.0050. [DOI] [PubMed] [Google Scholar]
- 107.Spaziante R, de Divitiis E, Giamundo A, Gambardella A, Di Prisco B. Ewing's sarcoma arising primarily in the spinal epidural space: Fifth case report. Neurosurgery. 1983;12:337–41. doi: 10.1227/00006123-198303000-00018. [DOI] [PubMed] [Google Scholar]
- 108.Tefft M, Vawter GF, Mitus A. Paravertebral: “Round cell” tumors in children. Radiology. 1969;92:1501–9. doi: 10.1148/92.7.1501. [DOI] [PubMed] [Google Scholar]
- 109.Theeler BJ, Keylock J, Yoest S, Forouhar M. Ewing's sarcoma family tumors mimicking primary central nervous system neoplasms. J Neurol Sci. 2009;284:186–9. doi: 10.1016/j.jns.2009.03.031. [DOI] [PubMed] [Google Scholar]
- 110.Uesaka T, Amano T, Inamura T, Ikezaki K, Inoha S, Takamatsu M, et al. Intradural, extramedullary spinal Ewing's sarcoma in childhood. J Clin Neurosci. 2003;10:122–5. doi: 10.1016/s0967-5868(02)00279-5. [DOI] [PubMed] [Google Scholar]
- 111.Virani MJ, Jain S. Primary intraspinal primitive neuroectodermal tumor (PNET): A rare occurrence. Neurol India. 2002;50:75–80. [PubMed] [Google Scholar]
- 112.Wasserberg J, Al-Sarraj S, Bridges LR. Peripheral neuroepithelioma presenting as a spinal cord tumor. Br J Neurosurg. 1994;8:497–9. doi: 10.3109/02688699408995122. [DOI] [PubMed] [Google Scholar]
- 113.Weber DC, Rutz HP, Lomax AJ, Schneider U, Lombriser N, Zenhausern R, et al. First spinal axis segment irradiation with spot-scanning proton beam delivered in the treatment of a lumbar primitive neuroectodermal tumor. Case report and review of the literature. Clin Oncol (R Coll Radiol) 2004;16:326–31. doi: 10.1016/j.clon.2004.03.002. [DOI] [PubMed] [Google Scholar]
- 114.Weil RJ, Zhuang Z, Pack S, Kumar S, Helman L, Fuller BG, et al. Intramedullary Ewing sarcoma of the spinal cord: Consequences of molecular diagnostics. Case report. J Neurosurg. 2001;95(Suppl 2):270–5. doi: 10.3171/spi.2001.95.2.0270. [DOI] [PubMed] [Google Scholar]
- 115.Woestenborghs H, Debiec-Rychter M, Renard M, Demaerel P, Van Calenbergh F, Van Gool S, et al. Cytokeratin-positive meningeal peripheral PNET/Ewing's sarcoma of the cervical spinal cord: Diagnostic value of genetic analysis. Int J Surg Pathol. 2005;13:93–7. doi: 10.1177/106689690501300114. [DOI] [PubMed] [Google Scholar]
- 116.Yavuz AA, Yaris N, Yavuz MN, Sari A, Reis AK, Aydin F. Primary intraspinal primitive neuroectodermal tumor: Case report of a tumor arising from the sacral spinal nerve root and review of the literature. Am J Clin Oncol. 2002;25:135–9. doi: 10.1097/00000421-200204000-00007. [DOI] [PubMed] [Google Scholar]