

Abstract
The expressed emotion (EE) is considered to be an adverse family environment, which includes the quality of interaction patterns and nature of family relationships among the family caregivers and patients of schizophrenia and other psychiatric disorders. Influence of EE has been found to be one of the robust predictors of relapse in schizophrenia. This review article aims to provide a brief description of the origins and evolution of the EE as a construct from the available literature. The EE is modulated by multiple factors–some of which include certain personality profile, attribution factors by caregivers toward patient symptoms, and patient's vulnerability to stress. The psychosocial assessment and interventions specifically focused on family psychoeducation can potentially reduce high EE and relapse of symptoms as well. However, the theory surrounded with EE undermines the caregiver's positive attitudes toward the patients. Hence, it is important that the future studies should focus on both protective and vulnerable factors within the construct of EE in schizophrenia to facilitate comprehensive care.
Keywords: Caregivers, expressed emotion, schizophrenia
INTRODUCTION
Expressed emotion (EE) refers to care giver's attitude towards a person with a mental disorder as reflected by comments about the patient made to an interviewer. It is a significant characteristic of the family milieu that has been found to predict symptom relapse in a wide range of mental disorders.[1] The empirical data show that EE is one of the major psychosocial stressor and it has direct association with recurrence of illness. The importance of EE depends on research that has consistently established that persons with mental illness, such as schizophrenia, who live with close relatives who have negative attitudes, are significantly more likely to relapse.[1] Research on EE was initiated in the 1950s, with researchers observing that close emotional ties between families could lead to sub-optimal stimulation and social withdrawal by the patient.[2] The emotional expressions that form the basis of EE were selected purely based on their considerable relationship to relapse, rather than a particular theory of knowledge.[3]
The construct of EE comprises of the following factors/behavioral patterns: Criticism, hostility, and emotional overinvolvement (EOI). Like many other environmental stressors, EE behaviors are not pathological or unique to families of mental disorders, but they can cause relapse of psychiatric symptoms among people with a vulnerability to stress. It has been sufficiently established that high EE attitudes are reflected in actual interactions within the families of mental illness.[4–7] Findings states that communication patterns in families with high EE relatives are usually characterized by more intense and negative verbal exchanges, oppositional or conflictual in nature[6,8,9] and another significant finding is that interaction patterns in high EE dyads (of patient and caregiver) are more likely to be rigid.[7,8,10,11]
Hence, EE refers to the quality of family interactions, explicitly the existence of hostility, criticism, and EOI. Researchers have positioned EE within the diathesis-stress model of psychopathology, characterizing it as an environmental stressor that can potentially precipitate/cause relapse of psychosis among people with a genetic vulnerability.[12]
ORIGINS OF EXPRESSED EMOTION
To understand the origins of the concept “Expressed Emotion,” one has to go back to the 1950s for the seminal works by George Brown. In 1956, George Brown joined the Medical Research Council Social Psychiatry (MRCSP) Unit of London, which was established in 1948 under Sir Aubrey Lewis's directorship. When George Brown joined the MRCSP unit and at this point of juncture, the antipsychotic drug chlorpromazine was being widely used to treat schizophrenia patients that led to the discharge of long-stay patients after they became symptomatically stable and recovered functionally. However, many of these patients were to be readmitted soon after discharge due to symptom relapse. To understand the basis for the symptom relapse, a study was initiated by George Brown and his colleagues with 229 men discharged from psychiatric hospitals, 156 of them with a diagnosis of schizophrenia.[13]
From the study, it was observed that the strongest link with relapse and readmission was the type of home to which patients were discharged. Surprisingly, the patients who discharged from hospital to stay with their parents or wives were more likely to get relapse and needed readmission than those who lived in lodgings or with their siblings. It was also found that patients staying with their mothers had reduced risk of relapse and readmission if patients and/or their mother went out to work.[14] It suggested the probable adverse influence of prolonged contact of patients with their family members in influencing the degree of disability and level of functioning.[15]
EXPRESSED EMOTION – THE CONSTRUCT
George Brown recognized that it was essential to build up a consistent method of measuring emotional relationships between patients and their close relatives. It was surprising that in 1950s, the assessment of family relationships had little attention, because during that decade family therapy was only emerging. At this point of time, Brown was joined by Michael Rutter who was interested in the study of the emotional impact of neurotic parents on their children. They introduced an audio-taped interview method to measure the emotions and the relationships among the patients and their caregiver relatives. Initially, they focused on married couples, and only later on, they extended their work to include the parents of people with schizophrenia.[15]
THE COMPONENTS OF EXPRESSED EMOTION
George Brown explained five components of EE[15] which includes critical comments, hostility, EOI, positive remarks, and warmth.[16] The quantification of critical comments and hostility is greatly reliant on the way in which the respondent uses their tone of voice to convey their feelings (anger, rejection, irritability, ignorance, blaming, negligence, etc), while the judgment of overinvolvement also takes into account on the basis of reported behavior such as caregivers blaming themselves, sacrificing things, being overprotective of patients, excessively being concerned for patients, neglecting personal needs of self (i.e., caregiver's), and similar others. The following sections provide brief description of these components along with examples to illustrate these components. These corresponding examples are designed based on the items from various scales that are used in the assessment of EE.
Critical comments
These are basically counted during the interview. Careful observations of direct communications among patients and caregivers prove that critical caregivers get involved in angry exchanges with the patient whom they seem unable to prevent or to step away from.[17] These potentially lead to physical violence, and it is the nature of some families with high EE. Patients who are unable to get up in the morning, who fail to wash regularly, or who do not participate in household tasks are criticized for being lazy and selfish; unfortunately, in this context, the caregivers fail to understand that these could be potential manifestations of negative symptoms of schizophrenia or any other psychotic disorder. This is reflected in the fact that 70% of critical comments were found to focus on these negative symptoms of schizophrenia rather than on the florid symptoms of delusions and hallucinations.[18] By contrast, low EE caregivers are more capable to recognize aspects of the patient's behavior which are a manifestation of the illness.
Examples: Family caregiver may express in an increased tone, tempo, and volume that patient frustrates them, deliberately causes problems for them, family members feel burden of patient, living with him is harder, commenting that patient is ignoring or not following their advices.
Hostility
It is rated as being absent or present during the interview and it is a consequence of unmanageable anger and irritation followed by critical comments and leads to rejection of the patient. Hostility is expressed by general criticisms or attitudes that are rejecting of the patient.[16]
Examples: Caregivers state that patient causing problems for them, wishing to live away from the patient, shouting at the patient, easily getting angry and getting irritation, patient can control himself, he is acting.
Emotional overinvolvement
EOI manifests itself by over-emotionality, excessive self-sacrifice, over-identification,[16] and extreme overprotective behavior with the patient. When George Brown[15] extended his initial research interest from married couples to the parents of schizophrenia patients, he became conscious of the need to develop a scale for assessing EOI. Parents of a child, who develops schizophrenia, always feel guilty for the child's illness. This chronic guilt leads them to initiate reparative efforts to make things better for the child, and in its extreme form can signify the overprotectiveness for the sick person. Unfortunately, this has the effect of discouraging the person's skills and self-reliance, so that in the long run, overprotectiveness hampers the person's recovery. It also leads to dependence of the patient on their caregiver. The patient then becomes worried about the outlook of having to cope without the continuous support of their caregiver and becomes dependent. This EOI is most commonly shown by parents, especially mothers, and occasionally by fathers, but rarely by other relatives.
Examples: Caregivers blame themselves for everything, feeling like everything is their fault; showing pity, not allowing the patient to carry out his day-to-day activities, neglecting self, giving less important personal needs rather than patient needs.
Warmth
It is assessed based on kindness, concern, and empathy expressed by the caregiver while talking about the patient. It depends greatly on vocal qualities with smiling being a common accompaniment, which often conveys an empathic attitude by the relative. Warmth is a significant characteristic of the low EE family.
Examples: Caregivers state that patient tries to get along with everyone, he makes a lot of sense, he is easy to get along with, and it is good to have him around, patient's behaviour is appropriate since it is not his/her pre-morbid self.
Positive regard
Positive regard comprises of statements that express appreciation or support for patient's behavior and verbal/nonverbal reinforcement by the caregiver.
Examples: Family states that they feel very close to the patient, they appreciate patient's little efforts or initiation in his day-to-day functioning, they state that they can cope with the patient and enjoy being with him/her.
ASSESSMENT OF EXPRESSED EMOTION
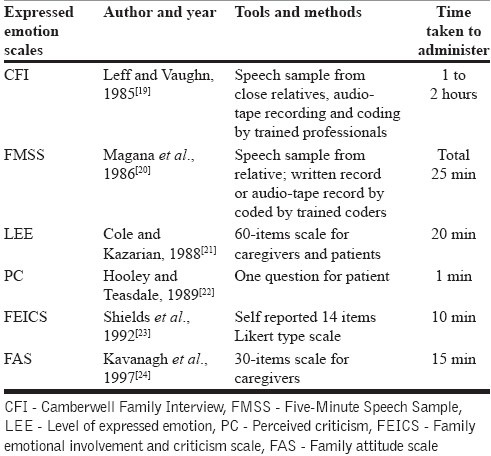
EE measures the attitudes, quality of relationships and interaction patterns among psychiatric patients and their close family members. There are many instruments which assess the family environment in terms of EE and some of the important EE assessment tools are discussed below (an overview of various scales is summarized in Table 1).
Table 1.
An overview of scales that assess expressed emotion
Camberwell family interview[19]
The EE status of the family members can be assessed with the Camberwell Family Interview (CFI) after the patient had been admitted to in-patient care. It is a well-known gold-standard measure of EE. The CFI is conducted with the patient's close relatives (family caregiver) without the patient being present. During the interview, relative's speech is recorded and later used for coding. This semi-structured interview consist of questions which address the onset of the patient's illness and the symptoms that were noticeable to the relative in the months earlier to the patient's worsening of illness or admission to the hospital. Also, the interview focuses on the level of stress in the household, irritability among the family members, participation of the patient in routine household tasks, and the daily routines of the patient and various family members or overall family functioning. The duration of the interview is between 1 to 2 hours. The CFI gives ratings on five scales those are Criticism, Hostility, EOI, Warmth, and Positive Remarks. But, practically speaking, the most important EE scales are Criticism, Hostility, and EOI. The family is being classified as high and low EE based on the ratings of these three scales. If a close family member makes six or more critical comments and makes any statement that is rated as hostile, or shows indication of marked overinvolvement (a rating of 3 or more on a 0 – 5 scale), the relative is classified as high in EE.
Five-minute speech sample[20]
The five-minute speech sample (FMSS) is similar to the CFI in that family members talk about their patient and their relationship for five uninterrupted minutes and the speech is recorded and later coded for the overall level of EE, criticism, and EOI. The FMSS, however, requires less time to administer (5 minutes) and score (20 minutes) compared with the Camberwell Family Interview. One or more critical comments, negative comments about their relationship, or a critical statement at the start of the interview are all indicative of high criticism on FMSS, whereas FMSS EOI is characterized by excessive praising or loving comments about the patient, crying, or extreme emotional involvement, and self-sacrifice. The hostility and warmth are not assessed in this interview, but the FMSS does give a frequency count of the number of affirmative comments given by the relatives about the patient.
Level of expressed emotion scale[21]
This is a 60-item, self-report scale that measures the emotional environment in the patient's most important relationships. It has 60 items that form the four subscales, namely Intrusiveness, Emotional Response, Attitude toward Illness, and Tolerance and Expectations. Items are rated in a true–false format, and the scale produces a score for the level of EE overall as well as a score for each of the four response patterns. Two versions of the Level of expressed emotion (LEE) scale are available, which are patient and the relative's versions. The patient version asks patients to appraise their relationship with their close relative with whom they stay. The relative version requires the close relative to evaluate his or her relationship with the patient. Since it is a self-report measure, it is easy to administer than the CFI.
Perceived criticism[22]
This measure of EE is most simple of all measures. This scale recognizes that the most important element of EE is criticism. It consists of only one question, namely “How critical do you consider your relative to be of you?” It is administered as a 10-point Likert-type scale and anchored with the values “not at all critical” and “very critical indeed.” This scale takes very less time (1 minute) to administer it. Interviewer can ask patients to rate how critical they think their relatives are of them using this scale. In addition, interviewer can also ask patients how critical they think they are towards their relative using the same scale. A subsequent addition expand the questions to include ratings of upset (“When your caregiver or family member criticizes you, how upset do you get” or “When you criticize your caregiver or family member how upset does he or she get?”). In all cases, these items can also be answered by the caregivers or family members themselves.
Family emotional involvement and criticism scale[23]
It is a 14-item scale which assesses two dimensions of EE: EOI and perceived criticism (PC) in the family. It is important to address the EOI and criticism when working with families with member who has severe and persistent mental illness. Higher criticism and overinvolvement scores are associated with more mental healthcare visits to hospitals for biomedical and psychosocial services due to higher rates of relapses. This scale proposes that EE is an important variable in assessing and treating both biopsychological distresses. On 14-item scale, the PC subscale should clearly indicate negative attitudes and EOI scale clearly reveal high levels of emotional involvement.[23] The 14 items are organized such that PC is assessed by even-numbered items and EOI is measured by odd-numbered items. A 5-point Likert-type scale includes response options of almost never, once in a while, some, often, almost always. On this scale, high scores indicate greater levels of PC and EOI.
Family attitude scale[24]
It is a useful 30-item, self-report measure of EE which emphasizes on the criticism and hostility. Respondents report how often each statement is true on a scale ranging from “Everyday” (4) to “Never” (0). Responses are summed to give a score ranging from 0 to 120, with higher scores indicating higher levels of burden or criticism. It is alike to the Level of EE scale in that either close relatives or patients of schizophrenia may complete the scale. Some examples of items include “I wish he were not here,” “He appreciates what I do for him,” “I lose my temper with him,” “He is a real burden,” “He ignores my advice,” and “I feel very close to him,” “He is hard to get close to.”
CAREGIVER FACTORS ASSOCIATED WITH EXPRESSED EMOTION
Caregivers personality factors and expressed emotion
Although precise reason for high or low EE attitudes in caregivers is not yet completely unraveled, it has been suggested that EE might partially reflect caregiver's personality traits.[12] Hooley and Hiller[12] found that caregivers of schizophrenia patients, with high EE reported reduced satisfaction of their individual activities, reduced optimism about their future, and reduced self-efficacy compared with low EE caregivers. Moreover, caregivers of high EE were less empathic, rigid, and impatient than low EE caregivers. A critical comment of caregiver is dependent less on the degree of the patient's symptoms than on the caregiver's own personality factors. If a caregiver is easily adjusted to the difficult circumstances and has patience generally, he or she is likely to be a non-critical caregiver. If a caregiver is usually tense or irritable during stressful situations, this stress can result in feelings of anger.[19] All these factors reveal that personality characteristics are significantly related to caregiver's high or low EE.
Caregivers attribution factors of expressed emotion
Caregiver's attributions about the causes of the patient's illness or their illness behaviors are also been linked with EE. A particular group of attributions related with EE is controllability attributions. EE research reveals a association between caregiver's critical comments and controllability attributions such that high-criticism caregivers are more likely to believe that patients can have control over the manifestation of their symptoms than low-criticism parents.[25,26] An earlier research found that caregivers who focus more on mistakes or perceived discrepancies in their care-giving may believe that they have contributed to the patient's ongoing problems[27] which increases the possibility that feelings of guilt may be an antecedent of EOI behavior in caregivers of schizophrenia patients. If the caregivers believe that they have contributed to the patient's problems[27,28] in some way, then they might consequently behave in an emotionally over-involved way by expressing their feelings of guilt through overstressed emotional responses or protectiveness toward the patient. These guilty attributions of caregivers may be unnecessary (i.e., relatives may well have had nothing to do with the onset or course of illness), but these may be harmful to caregiver's as well as patient's psychological state.
Caregivers controlling behavioral factors and expressed emotion
A tendency to wish to control the patient's behavior may be another variable that underlies high EE.[29] Perhaps, caregivers who want to control a patient may criticize the patient in an attempt to modify his/her behavior. It is also feasible that caregivers who want to control a patient may occupy in behaviors characteristic such as overprotective behavior (EOI). It was said that high-criticism caregivers would report more controlling behavior toward the patient and toward others compared with low-criticism caregivers and the caregivers who blame themselves for the progress of the patient's schizophrenia would have lower levels of criticism and higher levels of EOI compared with those who did not make self-blaming attributions. If caregivers with high EE are likely to attempt to control others and patient, this would suggest that their controlling behaviors and EE tendencies are part of the caregiver's internal or personality traits. However, if they show more recurrent and excessive controlling behaviors toward the patient than others, this would support the notion that EE is more situation-specific than trait-related. It is essential to understand the highlighting of EE so that we can effectively help the families with high EE.
MODELS OF EXPRESSED EMOTION
Locus of control model[30]
Studies show that locus of control and EE has significant associations, especially with internal locus of control. Individuals with a high internal locus of control view themselves as accountable for the consequences of their actions and believe that they have control over reinforcements.[30] Those with a high internal locus of control are more likely to believe that their efforts will be successful and they are more active in seeking information and knowledge regarding their circumstances. Those with a high external locus of control believe that powerful others, fate, or chance primarily determine events. It is said to be the people with high external control who have no hold over the situation and they are reported to be inactive, have decreased self-esteem, and not trusting of others.[31,32] High EE caregivers, particularly those who are high in criticality, have been shown to have a more internally based locus of control than do low EE caregivers[33] and to be more self-blaming[33,34] also found that highly critical caregivers are more likely than low-critical caregivers to have an internal locus of control. Hooley[33] investigated and found that in caregivers of psychotic disorders, criticality and EOI were related with an internal locus of control.
Stress-diathesis model (stress vulnerability model)[35]
Stress-diathesis model combines both biological and ecological factors to explain the manifestation of mental disorders and it is one of the most significant models to understand the development of psychopathology.[35–37] In this model, the degree of vulnerability to a given psychiatric episode is determined by each person's tolerance to traumatic or stressful life events. As EE appears to accurately determine relapse among patients, the research suggested that family environment may be a major contributing factor to critical stress levels among persons with schizophrenia. Stress-diathesis approach facilitates the view that both patients and caregivers are involved in a system of mutual influence in which each contributes to the stress that acts on the intrinsic vulnerabilities of the other; this perspective emphasizes upon interactions between vulnerability and stress variables.
Considerable research data on EE with regard to illness relapse shows EE as a form of psychosocial stress. In the previous decades, the EE construct has led to the development of family-based psychosocial therapies for schizophrenia that seek to decrease patients’ relapse rates by changing structural aspects of the family environment.[38–40] These efforts have been satisfying and have yielded in substantial clinical benefit for many patients and their family caregivers.
EXPRESSED EMOTION AND RELAPSE IN SCHIZOPHRENIA
It is well established that high family levels of EE are consistently associated with higher rates of relapse in patients with schizophrenia. The first study to undertake the EE measure and connect it to the course of schizophrenia was investigated by Brown et al.[41] where the patients were followed up for 9 months after they discharged and sent to their home from hospital. It was found that prolonged contact of patients with the critical caregivers determines the relapse in schizophrenia.[15]
Kavanagh[42] reviewed 26 of studies on EE and found that the mean relapse rate was 48% for patients residing with high EE families and 21% for those in low EE families. A comprehensive analysis by Bebbington and Kuipers[43] of data from 1,346 patients established the relationship between family caregiver's EE and relapse, and also the protective factor of reduced face-to-face contact for patients in high EE families. Evaluation of gender effect showed that although women with schizophrenia had a better outcome than men, the associations held true for both sexes. The odds ratio for relapse in high EE compared with low EE homes was 4.30 for men and 4.37 for women. A meta-analysis of 26 studies[1] confirmed that living in a high EE home environment is more than twice the baseline recurrence rate of symptoms for schizophrenia patients.
PSYCHOSOCIAL INTERVENTIONS TO REDUCE EXPRESSED EMOTION
The advances in the research on EE in the caregivers of patients with schizophrenia in diverse settings have led to the advances in psychosocial intervention strategies with family caregivers. The aim of such strategic interventions is to reduce EE by educating them and also to reduce the direct contact with high EE caregivers to less than 35 hours per week. Good number of studies have shown that it is possible. Low level of EE can be attained through individual and group work with families and patients. The psychosocial interventions are proven to be effective in combination with the pharmacotherapies. Numerous studies have shown that the quality of the caregiver and patient relationships that are the important determinants of outcome, not the type of family. High EE is proven to be a significant family stressor resulting from relationship problems among the caregivers and patients which is also a strong predictor of schizophrenia course. Hence, the family-focused psychosocial interventions primarily emphasize on reducing the levels of EE of caregivers by enhancing their knowledge about the illness.
Family psychoeducation (FP) for schizophrenia refers generally to several different models of treatment in which the caregivers of a person with schizophrenia are active members and focus of interventions. This is because the caregivers play a significant impact on the treatment outcome of the patient's illness. The FP aims at reducing re-hospitalization by controlling the relapse of symptoms and adhering to the treatment, and also it aims to reduce the distress faced by family caregivers and improve patient-family relations and communication patterns. FP includes education to the patient and caregiver about illness, crisis management, problem-solving skills, clarifying myths and misconceptions, and emotional support. The length and duration of the intervention varies across the cultures. It depends upon the person's socioeconomic, education, and domicile status.
Models of psychoeducation
Barrowclough et al.[25] proposed two models of education: Deficit model and interaction model. Deficit model suggests that an inadequate knowledge of information about illness results in negative behavior and disseminating of that knowledge will reduce this behavior. The deficit model suggests that inadequate knowledge of information about the illness results in producing negative attitudes and behaviors in the family caregivers of schizophrenia that have an unfavorable impact on patients and disseminating information will eliminate the inadequate knowledge, and result in more positive attitudes and behaviors toward the patients. This model was the basis behind the inclusion of the education element in the initial experimental (intervention) studies based on the high EE concept of schizophrenia.
Interaction model suggests that people make their own explanations of illness and that information provided by professionals will be understandable, organized, and possibly rejected on the basis of the person's own perceptions and explanations.
Evidence and efficacy of psychoeducation
Tarrier et al.[44] suggested that education of EE to caregivers is more likely to be useful if it is provided earlier when the patient is in acute stage of illness. Hence, the education will target reducing stress in the family caregivers. The goal of psychosocial interventions primarily aimed at reducing from High to Low EE, because High EE caregivers are associated with higher rates of symptom relapse. Successful transitions from high EE to low EE has been demonstrated, when intervention is provided in group therapy format.[38,44,45]
The history of family-focused interventions aimed at reducing the high EE was well documented in the study by Brown et al.,[41] with the primary of clarifying the association between EE and relapse, and to recognize the effective treatment strategies for persons having schizophrenia with high EE. They developed an intervention consisting of education about schizophrenia, problem solving and communication skills, reducing caregiver and patient's direct contact, strengthening the families’ social support, and decreasing the caregiver's expectations on patients.[46] A randomized controlled trial which included the high EE caregivers of persons with schizophrenia and intervention was found to be effective in changing three quarters of the experimental group families in the desired direction.[45] Although the patients in the experimental families had a relapse rate of only 8% over nine months, the control group rate had a rate of 50%.
In another study that reported a two-year follow-up of a trial of family sessions in the home (including patients) (12 families) vs a relatives' group (excluding patients) (11 families), it was observed that the relapse rates for patients in the family-therapy and relatives’-group streams were 33% and 36% at two years, respectively. When the authors combined these data with the results of a previous trial, it was found that patients in families assigned to any form of social intervention had a two-year relapse rate of 40%, significantly lower than the 75% relapse rate for patients whose families were offered no help.[47]
Brown and Rutter[2] confirmed, and Butzlaff and Hooley[1] have lately supported the theory, that schizophrenia patients who got discharge from the hospitals and returned to their families who were high in EE were more likely to experience a relapse during the following year regardless of adequate pharmacotherapy. Even though high EE attitudes are not specific to family caregivers of patients with schizophrenia,[1] the EE literature suggests most of the early randomized controlled trials of family interventions which aimed at reducing symptom relapse in schizophrenia to be beneficial.
The family interventions are primarily designed at reducing patient's relapse rates by reducing EE. However, previous decades’ research has unraveled various other factors to be involved in the origin and maintenance of family caregiving relationships, such as illness understanding and attributions, coping strategies, social support, depression, increased distress, and reduced self-esteem.[48] This has led to the inclusion of new targets for these interventions as well as new outcome measures focusing not only on service users, but also on caregivers. Traditionally, lack of educational approaches has resulted in dearth of data on the effectiveness of family interventions.[49] However, in recent years, we have seen a lot of studies in Asia, Latin America, and Europe reporting successful replication of controlled trial results.[50–52] Published clinical trials have demonstrated reliable evidence on family interventions reducing symptom relapses, having a positive impact on family relationships, and reducing overall costs of care.[50,53] More recent meta-analyses have shown that compared with as usual case management, family-focused interventions decrease patient's relapse rates and re-hospitalization, improve patient's adherence to pharmacotherapy, and improve social dysfunction as well as the amount of EE within the family.[54]
CONCLUSIONS AND FUTURE DIRECTIONS
Caring for a person with schizophrenia is highly challenging and it might result in negative emotional atmosphere in the patient's family. This emotional atmosphere means the quality of caregiver's attitudes and relationships toward the patients is a robust variable which can negatively affect both the patients and caregivers. Moreover, this negative family atmosphere causes not only relapse of symptoms and re-hospitalization, but it has significant effect on the course of the illness. The symptoms of patient influence the caregiver's EE and this in turn influence the symptom relapse in patients. Hence, the treatment should attempt at a holistic, a multidisciplinary, bio-psychosocial approach which should manage the patient and family in all dimensions. Moreover, clinical practitioners need different outlook in assessing, providing interventions, and carry out research work.
Measurement
Much of the EE literature continues to use the families as high and low EE with terms of negative approach such as critical, hostile, and over involved families. The caregivers’ invaluable contribution in the treatment is under-recognized. Even though the families show positive regard and warmth toward the patient, which is strength for better treatment outcome, it has been ignored as part of routine clinical EE assessment. Many of the available assessments focus on negatively classifying the families and their positive side has been neglected in the EE evaluation. Another short come of the current assessments is that they have been constructed, standardized, and validated in the western countries and while applying in different cultural context, one has to consider various methodological constraints. Thus, cultural-specific measurements have to be constructed and validated.
Training
The assessment of EE can be accurate when the clinical rater is trained. Thus, postgraduate training programs should give emphasis to train the students of psychiatry, clinical psychology, psychiatric social work, and psychiatric nursing in the measurement of EE. They should be trained in both qualitative-quantitative and structured-semi-structured interview methods.
Interventions
The psychosocial interventions such as psychoeducation, communication skills, problem-solving skills, social skills and occupational training, crisis management, and healthy coping strategies with the ongoing pharmacotherapy proved effective in reducing the high EE and improving treatment outcome. However, giving these interventions means seeing families as pathological and not recognizing their potentials or what we can say strengths. Thus, current psychosocial interventions employ deficit models of interventions. Now, there is a paradigm shift in clinical interventions since resilience or strength-based interventions are drawing much attention in clinical practice, which examines client's strengths in terms of their potentials, skills, wisdom, goals, ability to growth and change, social support networks, their needs and make use of these resources in the interventions. The individual case management has been demonstrated to adaptively influence the clinical outcomes in some studies, but the group interventions are yet to be explored systematically.
Future research
There is some evidence available on strength-based intervention in the field of child and adolescents behavioral problems and alcohol dependence, but there is a dearth of research regarding the resiliency or strength-based approaches with regard to the interventions for EE for families with schizophrenia patients. Hence, future research should stress on the feasibility and efficacy of the strength-based or resiliency-based interventions with ongoing psychosocial interventions at individual or group level for the persons and families of schizophrenia to deal with the negative emotional atmosphere of the family. This approach can address both vulnerable and protective factors (strengths) of caregivers which will help in comprehensive assessment- and need-based service provision to the patient and the family.
ACKNOWLEDGMENT
This work is supported by the Wellcome Trust/DBT India Alliance Senior Fellowship Grant.
Footnotes
Source of Support: Wellcome Trust/DBT India Alliance Senior Fellowship Grant
Conflict of Interest: None.
REFERENCES
- 1.Butzlaff RL, Hooley JM. Expressed emotion and psychiatric relapse: A meta-analysis. Arch Gen Psychiatry. 1998;55:547–52. doi: 10.1001/archpsyc.55.6.547. [DOI] [PubMed] [Google Scholar]
- 2.Brown GW, Rutter M. The measurement of family activities and relationships: A methodological study. Hum Relations. 1966;19:241–58. [Google Scholar]
- 3.Greenley JR. Social control and expressed emotion. J Nerv Ment Dis. 1986;174:24–30. doi: 10.1097/00005053-198601000-00004. [DOI] [PubMed] [Google Scholar]
- 4.Miklowitz DJ, Goldstein MJ, Doane JA, Nuechterlein KH, Strachan AM, Snyder KS, et al. Is expressed emotion an index of a transactional process? I. Parents’ affective style. Fam Process. 1989;28:153–67. doi: 10.1111/j.1545-5300.1989.00153.x. [DOI] [PubMed] [Google Scholar]
- 5.Strachan AM, Feingold D, Goldstein MJ, Miklowitz DJ, Nuechterlein KH. Is expressed emotion an index of a transactional process? II. Patient's coping style. Fam Process. 1989;28:169–81. doi: 10.1111/j.1545-5300.1989.00169.x. [DOI] [PubMed] [Google Scholar]
- 6.Wuerker AM. Relational control patterns and expressed emotion in families of persons with schizophrenia and bipolar disorder. Fam Process. 1994;33:389–407. doi: 10.1111/j.1545-5300.1994.00389.x. [DOI] [PubMed] [Google Scholar]
- 7.Wuerker AK. Communication patterns and expressed emotion in families of persons with mental disorders: The negotiation of who's in charge. Schizophrenia Bull. 1996;22:671–90. doi: 10.1093/schbul/22.4.671. [DOI] [PubMed] [Google Scholar]
- 8.Hahlweg K, Goldstein MJ, Nuechterlein KH, Magafia AB, Mintz J, Doane JA, et al. Expressed emotion and patient-relative interaction in families of recent onset schizophrenics. J Consult Clin Psychol. 1989;57:11–8. doi: 10.1037//0022-006x.57.1.11. [DOI] [PubMed] [Google Scholar]
- 9.Cook WL, Strachan AM, Goldstein MJ, Miklowitz DJ. Expressed emotion and reciprocal affective relationships in families of disturbed adolescents. Fam Process. 1989;28:337–48. doi: 10.1111/j.1545-5300.1989.00337.x. [DOI] [PubMed] [Google Scholar]
- 10.Hubschmid T, Zemp M. Interactions in high- and low- EE families. Soc Psychiatry Psychiatr Epidemiol. 1989;24:113–9. doi: 10.1007/BF01788635. [DOI] [PubMed] [Google Scholar]
- 11.Wuerker AK, Haas GL, Bellack AS. Interpersonal control and expressed emotion in families of persons with schizophrenia: Change over time. Schizophrenia Bull. 2001;27:671–86. doi: 10.1093/oxfordjournals.schbul.a006906. [DOI] [PubMed] [Google Scholar]
- 12.Hooley JM, Hiller JB. Personality and expressed emotion. J Abnorm Psychol. 2000;109:40–4. [PubMed] [Google Scholar]
- 13.Leff J. Expressed emotion: Measuring relationships. In: Harris T, editor. Where inner and outer worlds meet: Psychosocial research in the tradition of George W Brown. London: Routledge; 2000. pp. 97–100. [Google Scholar]
- 14.Brown GW. Experiences of discharged chronic schizophrenic mental hospital patients in various types of living groups. Milbank Mem Fund Q. 1959;37:105–31. [PubMed] [Google Scholar]
- 15.Brown GW. The discovery of expressed emotion: Induction or deduction? In: Leff J, Vaughn C, editors. Expressed emotion in families. New York: Guilford Press; 1985. pp. 7–25. [Google Scholar]
- 16.Wearden AJ, Tarrier N, Barrowclough C, Zastowny TR, Rahill AA. A review of expressed emotion research in health care. Clin Psychol Rev. 2000;20:633–66. doi: 10.1016/s0272-7358(99)00008-2. [DOI] [PubMed] [Google Scholar]
- 17.Hooley J, Hahlweg K. The marriages and interaction patterns of depressed patients and their spouses: Comparison of high and low EE dyads. In: Goldstein MJ, Hand I, Hahlweg K, editors. Treatment of Schizophrenia: Family assessment and intervention. Berlin: Springer Verlag; 1986. pp. 85–95. [Google Scholar]
- 18.Vaughn CE, Leff JP. The measurement of expressed emotion in the families of psychiatric patients. Br J Soc Clin Psychol. 1976;15:157–65. doi: 10.1111/j.2044-8260.1976.tb00021.x. [DOI] [PubMed] [Google Scholar]
- 19.Leff J, Vaughn C. Expressed Emotion in Families. New York: Guilford Press; 1985. [Google Scholar]
- 20.Magana AB, Goldstein MJ, Kamo M, Miklowitz DJ, Jenkins J, Falloon IR. A brief method for assessing expressed emotion in relatives of psychiatric patients. Psychiatry Res. 1986;17:203–13. doi: 10.1016/0165-1781(86)90049-1. [DOI] [PubMed] [Google Scholar]
- 21.Cole JD, Kazarian SS. The Level of Expressed Emotion Scale: A new measure of expressed emotion. J Clin Psychol. 1988;44:392–7. doi: 10.1002/1097-4679(198805)44:3<392::aid-jclp2270440313>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 22.Hooley JM, Teasdale JD. Predictors of relapse in unipolar depressives: Expressed emotion, marital distress, and perceived criticism. J Abnorm Psychiatry. 1989;98:229–35. doi: 10.1037//0021-843x.98.3.229. [DOI] [PubMed] [Google Scholar]
- 23.Shields CG, Franks P, Harp JJ, McDaniel SH, Campbell TL. Development of the family emotional involvement and criticism scale (FEICS): A self-report scale to measure expressed emotion. J Marital Fam Ther. 1992;18:395–407. [Google Scholar]
- 24.Kavanagh DJ, O’Halloran P, Manicavasagar V, Clark D, Piatkowska O, Tennant C, et al. The family attitude scale: Reliability and validity of a new scale for measuring the emotional climate of families. Psychiatry Res. 1997;70:185–95. doi: 10.1016/s0165-1781(97)00033-4. [DOI] [PubMed] [Google Scholar]
- 25.Barrowclough C, Johnston M, Tarrier N. Attributions, expressed emotion, and patient relapse: An attributional model of relatives’ response to schizophrenia illness. Behav Ther. 1994;25:67–88. [Google Scholar]
- 26.Hooley JM. The nature and origins of expressed emotion. In: Hahlweg K GM, editor. Understanding major mental disorder: The contribution of family interaction research. New York: Family Process; 1987. pp. 176–94. [Google Scholar]
- 27.Bentsen H, Notland TH, Munkvold O, Boye B, Ultsein I, Bjorge H, et al. Guilt proneness and expressed emotion in relatives of patients with schizophrenia or related psychoses. Br J Med Psychol. 1998;71:125–38. doi: 10.1111/j.2044-8341.1998.tb01374.x. [DOI] [PubMed] [Google Scholar]
- 28.Chambless DL, Bryan AD, Aiken LS, Steketee G, Hooley JM. Predicting expressed emotion: A study with families of obsessive-compulsive and agoraphobic outpatients. J Fam Psychol. 2001;15:225–40. doi: 10.1037//0893-3200.15.2.225. [DOI] [PubMed] [Google Scholar]
- 29.Hooley JM. Expressed emotion: A review of the critical literature. Clin Psychol Review. 1985;5:119–39. [Google Scholar]
- 30.Rotter JB. Social learning and clinical psychology. New York: Prentice-Hall; 1954. [Google Scholar]
- 31.Silvester J, Anderson-Gough FM, Anderson NR, Mohammed AR. Locus of control, attributions and impression management in the selection interview. J Occup Organ Psychol. 2002;75:59–76. [Google Scholar]
- 32.Loosemore M, Lam AS. The locus of control: A determinant of opportunistic behaviour in construction health and safety. Constr Manage Econ. 2004;22:385–94. [Google Scholar]
- 33.Hooley JM. Expressed emotion and locus of control. J Nerv Ment Dis. 1998;186:374–8. doi: 10.1097/00005053-199806000-00009. [DOI] [PubMed] [Google Scholar]
- 34.Docherty NM, Cutting LE, Bers SA. Expressed emotion and the differentiation of self in the relatives of stable schizophrenia outpatients. Psychiatry. 1998;61:269–78. doi: 10.1080/00332747.1998.11024839. [DOI] [PubMed] [Google Scholar]
- 35.Zubin J, Spring BJ. Vulnerability: A new view of schizophrenia. J Abnorm Psychol. 1977;86:103–26. doi: 10.1037//0021-843x.86.2.103. [DOI] [PubMed] [Google Scholar]
- 36.Monroe SM, Simons AD. Diathesis-stress theories in the context of life stress research: Implications for the depressive disorders. Psychol Bull. 1991;110:406–25. doi: 10.1037/0033-2909.110.3.406. [DOI] [PubMed] [Google Scholar]
- 37.Rosenthal D. Genetic theory and abnormal behavior. New York: McGraw-Hill; 1970. [Google Scholar]
- 38.Hogarty GE, Anderson CM, Reiss DJ, Kornblith SJ, Greenwald DE, Janva CD, et al. Family psychoeducation, social skills training, and maintenance chemotherapy in the aftercare treatment of schizophrenia. Arch Gen Psychiatry. 1986;43:633–42. doi: 10.1001/archpsyc.1986.01800070019003. [DOI] [PubMed] [Google Scholar]
- 39.McFarlane WR, Link B, Dushay R, Marchal J, Crilly J. Psychoeducational multiple family groups: Four-year relapse outcome in schizophrenia. Fam Process. 1995;34:127–44. doi: 10.1111/j.1545-5300.1995.00127.x. [DOI] [PubMed] [Google Scholar]
- 40.McFarlane WR, Lukens E, Link B, Dushay R, Deakins SA, Newmark M, et al. Multiple-family groups and psychoeducation in the treatment of schizophrenia. Arch Gen Psychiatry. 1995;52:679–87. doi: 10.1001/archpsyc.1995.03950200069016. [DOI] [PubMed] [Google Scholar]
- 41.Brown GW, Birley JL, Wing JK. Influence of family life on the course of schizophrenia disorder. Br J Psychiatry. 1972;121:241–58. doi: 10.1192/bjp.121.3.241. [DOI] [PubMed] [Google Scholar]
- 42.Kavanagh DJ. Recent developments in expressed emotion and schizophrenia. Br J Psychiatry. 1992;160:601–20. doi: 10.1192/bjp.160.5.601. [DOI] [PubMed] [Google Scholar]
- 43.Bebbington P, Kuipers E. The predictive utility of expressed emotion in schizophrenia: An aggregate analysis. Psychol Med. 1994;24:707–12. doi: 10.1017/s0033291700027860. [DOI] [PubMed] [Google Scholar]
- 44.Tarrier N, Barrowclough C, Vaughn C, Bamrah JS, Porceddu K, Watts S, et al. The community management of schizophrenia: A controlled trial of a behavioural intervention with families to reduce relapse. Br J Psychiatry. 1988;152:618–24. doi: 10.1192/bjp.153.4.532. [DOI] [PubMed] [Google Scholar]
- 45.Leff J, Kuipers L, Berkowitz R, Eberlein-Fries R, Sturgeon D. A controlled trial of social intervention in the families of schizophrenic patients. Br J Psychiatry. 1982;141:121–34. doi: 10.1192/bjp.141.2.121. [DOI] [PubMed] [Google Scholar]
- 46.Kuipers E, Leff J, Lam D. Family work for schizophrenia- a practical guide. London: Gaskell; 1992. [Google Scholar]
- 47.Leff J, Berkowitz R, Shavit N, Strachan A, Glass I, Vaughn C. A trial of family therapy versus a relatives’ group for schizophrenia, two year follow-up. Br J Psychiatry. 1990;157:571–7. doi: 10.1192/bjp.157.4.571. [DOI] [PubMed] [Google Scholar]
- 48.Kuipers E, Onwumere J, Bebbington P. Cognitive model of caregiving in psychosis. Br J Psychiatry. 2010;196:259–65. doi: 10.1192/bjp.bp.109.070466. [DOI] [PubMed] [Google Scholar]
- 49.Dixon L, Postrado L, Delahanty J, Fisher P, Lehman A. The association of medical comorbidity in schizophrenia with poor physical and mental health. J Nerv Ment Dis. 1999;187:496–502. doi: 10.1097/00005053-199908000-00006. [DOI] [PubMed] [Google Scholar]
- 50.Falloon IR. Family interventions for mental disorders: Efficacy and effectiveness. World Psychiatry. 2003;2:20–8. [PMC free article] [PubMed] [Google Scholar]
- 51.Leff J. Family work for schizophrenia: Practical application. Acta Psychiatr Scand Suppl. 2000;102(suppl 407):78–82. doi: 10.1034/j.1600-0447.2000.00013.x. [DOI] [PubMed] [Google Scholar]
- 52.Magliano L, Fiorillo A. Psychoeducational family interventions for schizophrenia in the last decade: From explanatory to pragmatic trials. Epidemiol Psichiatr Soc. 2007;16:22–34. [PubMed] [Google Scholar]
- 53.McFarlane WR, Dixon L, Lukens E, Luckstead A. Family psychoeducation and schizophrenia: A review of the literature. J Marital Fam Ther. 2003;29:223–45. doi: 10.1111/j.1752-0606.2003.tb01202.x. [DOI] [PubMed] [Google Scholar]
- 54.Pharoah F, Mari J, Rathbone J, Wong W. Family intervention for schizophrenia. Cochrane Database of Systematic Reviews. 2010;12:CD000088. doi: 10.1002/14651858.CD000088.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]