
Figure 1. Fundamental mechanisms by which arousal and exercise triggers differentially affect LQT1 vs. LQT2.
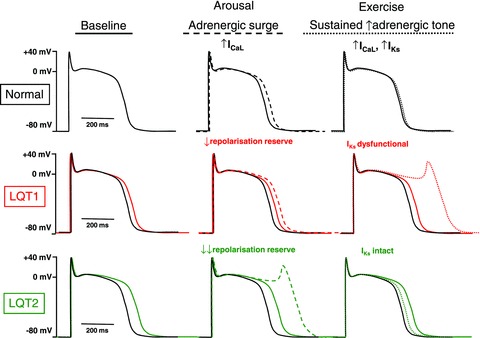
The normal cardiac AP is shown in black in all panels, whereas APs in LQT1 or LQT2 are shown in red and green, respectively (baseline APs are shown as continuous lines in each panel). Dashed and dotted lines in middle and right panels indicate changes resulting respectively from arousal (adrenergic surge) and exercise (sustained increase in adrenergic tone). Since IKr is the predominant repolarizing current under normal conditions, APs are more prolonged in LQT2 at baseline. With sudden arousal stimuli, there is a transient surge of adrenergic tone, which increases ICaL before any change in IKs. In LQT2, with major loss in repolarisation reserve due to loss of IKr, APs are strongly prolonged and EADs arise. In LQT1, intact IKr prevents excess AP prolongation. With exercise, sustained increases in adrenergic tone increase both ICaL and IKs, producing little net change in AP duration when IKs is intact. However, when IKs is dysfunctional and cannot increase to compensate for ICaL enhancement (LQT1), strong AP prolongation and EADs occur.