
Fig. 2.
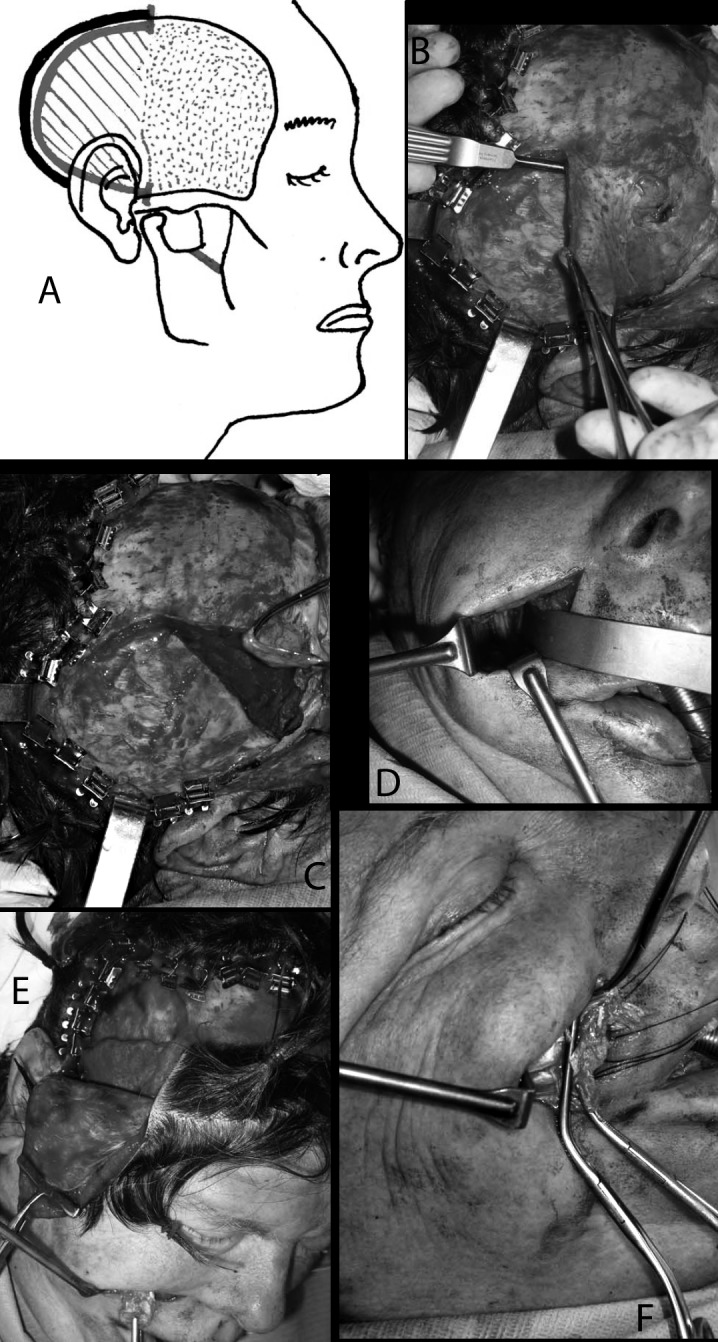
The continuous line shows incision of the temporal aponeurosis on the posterior part of the insertion of temporalis muscle, which in the hatched area is completely dissected and in the dotted area (anteriorly) is dissected only on its deeper surface (a). In the following pictures, the steps on the surgical bed are shown more in detail. After posterior detachment of the temporal aponeurosis (b), dissection of the posterior part of the muscle is carried out starting from the retrozygomatic region. The deep surface of the temporalis is dissected along a subperiostal plane down to the sphenotemporal crest below and to the temporal crest above (c). The coronoid process is reached through the nasolabial fold approach (d). After incision in the nasolabial crease and after tunnelizing in the corpus adiposum buccae synsarcosis by scissors, as in V1, the coronoid process is visualized and sectioned, preserving the attachments of the temporalis muscle. The coronoid process is grabbed and pulled towards the labial rim through the tunnel, with the muscle, whose dissection from masseterine fibres is completed in this phase, and the lengthening at the expense of the posterior part becomes evident (e). Finally, the coronoid process can be detached from the tendon which is sutured to the lips as in V1.