
Fig. 2.
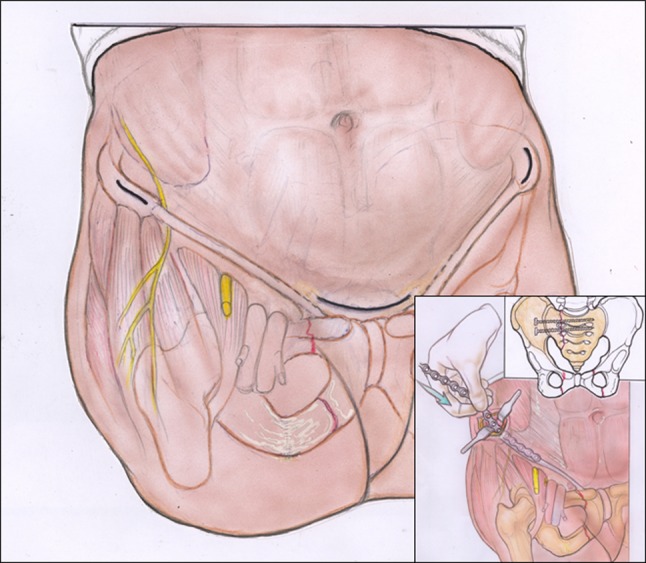
Skin incisions are demonstrated for the anterior pelvic bridge technique using locking reconstruction plates. Three incisions are required to place bilateral reconstruction plates: one incision over each ASIS and a transverse Pfannenstiel incision centered over the symphysis pubis. Important neurovascular structures are shown, including the LFCN coursing inferiorly to the inguinal ligament and the femoral nerve overlying the psoas muscle. Insertion of the precontoured reconstruction plates can be performed by hand after carefully creating a subcutaneous tunnel above the external oblique muscle with a cob or periosteal surfer (inset). The plate slides over the area of the conjoint tendon, well anterior to the posterior neurovascular structures. The posterior pelvic ring must be either stable or stabilized as the primary consideration of treatment for pelvic ring injuries. Reprinted with permission and copyright 2012 by Wolters Kluwer Health from Cole PA, Gauger EM, Anavian J, Ly TV, Morgan RA, Heddings AA. Anterior Pelvic External Fixator Versus Subcutaneous Internal Fixator in the Treatment of Anterior Ring Pelvic Fractures. J Orthop Trauma. 2012 February 21 [Epub ahead of print].