
Figure 1.
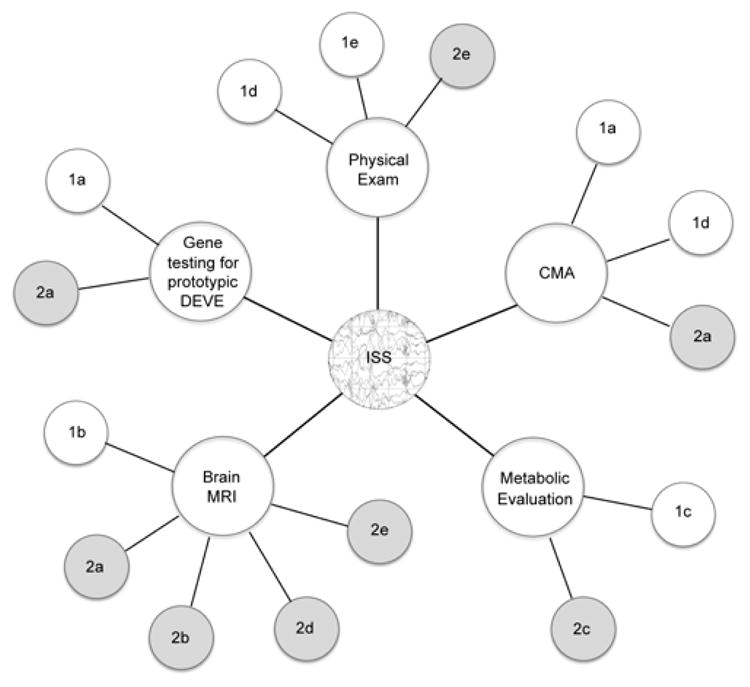
Evaluation of infantile spasms (ISS) using the classification system in Table 1. Diagnosis of ISS centers upon epileptic spasms associated with ictal electrodecrement. Evaluations may be carried out concurrently, depending upon the clinical scenario. Physical exam findings may lead to recognition of syndromes of genomic imbalance (Group 1d) such as Down syndrome, Williams syndrome, or Miller-Dieker syndrome; or may suggest other syndromes putatively associated with ISS (Group 1e); or recognizable genotype-unknown syndromes (Group 2e). Gene testing for the prototypic developmental epilepsies (DEVE) may find mutations in known associated genes (Group 1a); or if negative may suggest a genotype-unknown prototypic DEVE (Group 2a). Brain MRI may find specific structural brain malformations (Group 1b) and lead to specific follow-up genetic testing; or may reveal non-specific abnormalities associated with genotype-unknown prototypic DEVE (Group 2a), findings associated with genotype-unknown syndromes (Group 2b), extrinsic injury patterns (Group 2d), or recognizable abnormalities putatively associated with ISS (Group 2e). Metabolic evaluation may lead to identification of specific inborn errors of metabolism associated with ISS, leading to genetic testing for those disorders (Group 1c); or may reveal metabolic abnormalities associated with genotype-unknown conditions (Group 2c). Chromosomal microarray (CMA) may identify prototypic DEVE such as duplication of FOXG1 or deletion of CDKL5 or MEF2C (Group 1a); diagnose known syndromes of genomic imbalance associated with ISS (Group 1d); or may be negative suggesting a genotype-unknown prototypic DEVE (Group 2a).