

Abstract
Patients with a suspected acute coronary syndrome (ACS) and left bundle branch block (LBBB) present a unique diagnostic and therapeutic challenge to the clinician. Although current guidelines recommend that patients with new or presumed new LBBB undergo early reperfusion therapy, data suggest that only a minority of patients with LBBB are ultimately diagnosed with acute myocardial infarction regardless of LBBB chronicity and that a significant proportion of patients will not have an occluded culprit artery at cardiac catheterization. The current treatment approach exposes a significant proportion of patients to the risks of fibrinolytic therapy without the likelihood of significant benefit, and leads to increased rates of false-positive cardiac catheterization laboratory activation, unnecessary risks, and costs. Therefore, alternative strategies to those for patients with ST-elevation myocardial infarction (STEMI) are needed to guide selection of appropriate patients with suspected ACS and LBBB for urgent reperfusion therapy. In this article, we describe the evolving epidemiology of LBBB in ACS and discuss controversies related to current clinical practice. We propose a more judicious diagnostic approach among clinically stable patients with LBBB who do not have electrocardiographic findings highly specific for STEMI.
Keywords: Acute Myocardial Infarction, Left Bundle Branch Block, Fibrinolysis
Introduction
Patients with a suspected acute coronary syndrome (ACS) in the setting of left bundle branch block (LBBB) present an important diagnostic and therapeutic challenge to the clinician. Not only is the electrocardiographic (ECG) diagnosis of acute myocardial infarction (AMI) difficult due to “masking” of characteristic ECG changes by altered ventricular depolarization, but these patients may be at higher risk for AMI, congestive heart failure, and death compared with patients without bundle branch block (BBB) (1–3). Although current guidelines from the American College of Cardiology/American Heart Association (4) and the European Society of Cardiology (5) recommend that patients with new or presumed new LBBB undergo early reperfusion therapy with fibrinolysis or percutaneous coronary intervention (PCI), these recommendations are based on studies performed more than 20 years ago and the populations studied may differ notably from contemporary patient subsets.
In this article, we review the pathophysiologic mechanisms underlying LBBB in AMI, the historical context, epidemiology, and outcomes of the current recommended treatment approach, discuss controversies in clinical practice, and suggest future strategies for improvement in the efficiency and outcomes of care for patients with LBBB.
Pathophysiology of LBBB in AMI
The intraventricular conduction system of the left ventricle is composed of fibers of the bundle of His that become the main left bundle branch and then divide into anterior and posterior fascicles, further branching to become the distal conduction system. In contrast to the right bundle branch, which is a discrete structure that can be acutely injured with a small focal insult, the left bundle branch is a large and diffuse structure that typically requires a large insult to lead to acute injury (6). When a new LBBB is caused by AMI, the site of infarction is usually anterior or anteroseptal (7), with the infarction involving a large myocardial territory. Inferior or posterior infarctions may uncommonly result in a new LBBB from involvement of the more proximal portion of the conduction system supplied by the atrioventricular nodal artery. However, the majority of LBBB in AMI are not a result of focal infarctions since either a discrete lesion just distal to the bundle of His or extensive myocardial damage involving a large portion of the distal conduction system including both fascicles would be required to cause LBBB (Figure 1).
Figure 1. Anatomy of the Left Bundle Branch.
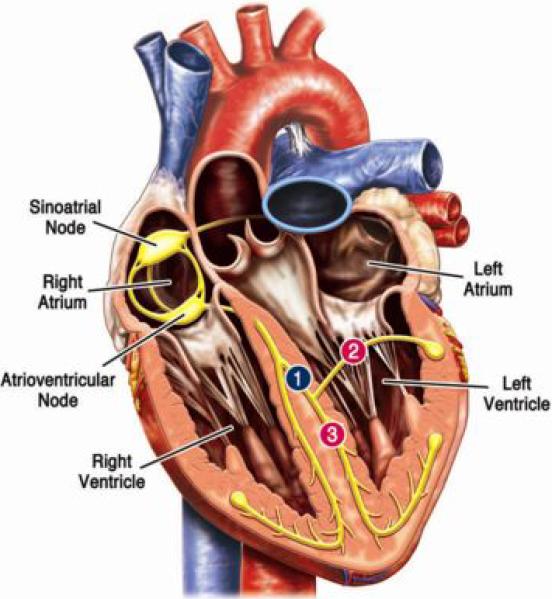
The left bundle branch is comprised of the main left bundle and distal anterior and posterior fascicles. LBBB resulting from an incident myocardial infarction requires a lesion just distal to the bundle of His (#1) or extensive myocardial damage involving a large portion of the distal conduction system including both fascicles (#2 and #3).
LBBB=left bundle branch block
Although LBBB can occur de novo in AMI, it is more often a pre-existing marker of underlying structural heart disease and thus reflective of the patient's baseline cardiovascular risk. In these cases, LBBB may be the result of an aging and/or fibrotic conduction system, chronic ischemic heart disease, left ventricular hypertrophy (most commonly from long-standing hypertension), adverse ventricular remodeling from congestive heart failure, or valvular heart disease. It is not possible to determine the chronicity of the LBBB without reviewing previous ECG tracings since the onset of LBBB is usually asymptomatic. LBBB in AMI may be transient or permanent, although early accounts noted that most cases of permanent LBBB were not the result of an acute transmural infarction, as true AMI-associated LBBB was associated with very high mortality (8).
Historical Perspective
Recognition of LBBB in AMI dates back to 1917 in an account by Oppenheimer and Rothschild (9). Early descriptions of BBB in AMI reported an incidence of 10–15% and a mortality rate of 42–63% (10). Patients with BBB tended to be significantly older and have an increased frequency of hypertension, congestive heart failure, previous myocardial infarction, and cardiogenic shock. It is therefore difficult to discern if historical studies documenting the significantly increased mortality risk (approximately 2-fold) in BBB were confounded by age and co-morbid conditions. Additionally, studies included patients with both left and right bundle branch block, recorded ECGs at widely varied time points, lacked discrimination between new and old infarction, and had limited diagnostic resources to confirm AMI at presentation (11).
Clinicians have recognized that a diagnosis of AMI in the setting of LBBB is especially challenging for over 60 years (12). Since left ventricular activation occurs much later in LBBB and the initial septal activation advances from right to left (opposite of the normal situation), septal Q waves indicative of an AMI are absent. Additionally, secondary ST-T wave abnormalities that occur in LBBB obscure the recognition of injury currents in ischemia and infarction. Despite the suggestion of multiple criteria for diagnosis of AMI in the setting of LBBB, it was generally believed that clinicians remained largely “blind” to ECG changes in patients with LBBB (12). In 1996, Sgarbossa and colleagues published an analysis from the GUSTO-1 trial evaluating multiple different ECG criteria that had been suggested as being potentially useful for the diagnosis of AMI in the setting of LBBB (13). Of these, ST-elevation concordant with the major QRS deflection in any lead and ST-depression in leads V1, V2 or V3 had odds ratios for AMI of 25.2 (95% CI 11.6–54.7) and 6.0 (95% CI 1.9–19.3), respectively; discordant ST-elevation ≥5 mm in any lead had a weaker association (odds ratio 4.3, [95% CI 1.8–10.6]). When combined, these three ECG criteria yielded a sensitivity and specificity of approximately 78% and 90%, respectively. Subsequent validation studies have confirmed that ST-segment concordance criteria are highly specific for AMI, but have generally reported much lower sensitivities than the initial study (14–15). Currently, the Sgarbossa criteria are utilized most extensively to diagnose AMI in the setting of a known chronic LBBB. Although data exists to support use of the Sgarbossa criteria in new or indeterminate-age LBBB, current guidelines do not specifically include this application of the criteria in their recommendations.
Epidemiology and Clinical Trial Results
Individuals with LBBB represent approximately 2% of all patients who present with a suspected ACS (Table 1). They are more likely to be older, female, and have a history of pre-existing cardiovascular disease, hypertension, and congestive heart failure than non-BBB patients with ACS (1, 16). Patients with LBBB also have a greater likelihood of major adverse cardiac events including death, AMI, stroke, and revascularization over long-term follow-up compared with patients without BBB (1). However, these observations may be explained, in large part, by underlying ischemic and structural heart disease that is the substrate for the development of LBBB rather than by the LBBB itself. Since LBBB is strongly related to advancing age which, in turn, is associated with many chronic disease states and the development of cardiac conduction disease, LBBB may be an integrative marker of overall cardiac risk rather than an independent contributor to morbidity and mortality (16).
Table 1.
Prevalence of LBBB and AMI in studies of patients with suspected ACS
| Study | Year | Total, no. of patients | No. of patients with LBBB (%) | No. of LBBB patients with AMI (%) |
|---|---|---|---|---|
| Randomized trials or registries enrolling patients with high suspicion or documentation of AMI, STEMI, or new LBBB | ||||
| Sgarbossa et al. (13) | 1996 | 26,003 | 145 (0.6) | 131 (90) |
| Cannon et al. (3) | 1997 | 1,416 | 127 (9) | 40 (31) |
| Wong et al. (22) | 2005 | 17,073 | 300 (1.8) | 242 (81) |
| Al-Faleh et al. (23) | 2006 | 22,839 | 267 (1.2) | 158 (63) |
| Lopes et al. (36) | 2011 | 5,742 | 98 (1.7) | 85 (87) |
| Jain et al. (42) | 2011 | 892 | 36 (4) | 12 (33) |
| Subtotal (n=6) | 73,965 | 973 (1.3) | 668 (67) | |
| More broadly representative studies of patients with suspected AMI presenting to ED | ||||
| Rude et al. (52) | 1983 | 3,697 | 178 (4.8) | 82 (46) |
| Fesmire et al. (53) | 1989 | 440 | 24 (5.5) | 3 (13) |
| Otto and Aufderheide (54) | 1994 | 428 | 18 (4.2) | 5 (28) |
| Kudenchuk et al. (55) | 1998 | 3,027 | 57 (1.9) | 20 (35) |
| Edhouse et al. (56) | 1999 | 797 | 50 (6) | 26 (52) |
| Shlipak et al. (39) | 1999 | n/a | 83 (100) | 26 (31) |
| Li et al. (15) | 2000 | n/a | 190 (100) | 25 (13) |
| Kontos et al. (14) | 2001 | 7,725 | 182 (2.4) | 24 (13) |
| Gunnarsson et al. (43) | 2001 | n/a | 158 (100) | 76 (48) |
| Maynard et al. (57) | 2003 | n/a | 56 (100) | 18 (32) |
| Chang et al. (31) | 2009 | 7,937 | 191 (2.4) | 11 (6) |
| Bansilal et al. (1) | 2011 | 2,271 | 102 (4.5) | 5 (5) |
| Kontos et al. (34) | 2011 | n/a | 401 (100) | 116 (29) |
| Subtotal (n=13) | 26,322 | 802 (3.0) * | 437 (26) † | |
|
| ||||
| Total (n=19) | 100,287 | 1,775 (1.8) * | 1,105 (42) ‡ | |
does not include studies of patients with LBBB only
includes patients in all studies (n=1,690)
includes patients in all studies (n=2,663)
ACS=acute coronary syndrome; AMI= acute myocardial infarction; ED= emergency department; LBBB= left bundle branch block; n/a= not applicable; STEMI= ST-elevation myocardial infarction
The excess mortality risk associated with LBBB in AMI compared with normal conduction is unclear. Early observations of high mortality rates may have been confounded by co-morbid conditions or delays in diagnosis and treatment due to lack of ECG criteria. More contemporary studies from the reperfusion era reported that patients with BBB were less likely to receive immediate reperfusion therapy (including fibrinolysis or PCI), had longer delays between hospital arrival and initiation of reperfusion therapies, were less likely to receive evidence-based medical therapy, and had a 34–64% increased risk of in-hospital death, even after adjustment for potential confounders (2). However, right bundle branch block (RBBB) was observed to have a greater risk for mortality than LBBB, and other investigators have not been able to confirm an independent mortality risk of LBBB (16–18).
Initial clinical trials investigating the efficacy of fibrinolytic therapy included a broad range of patients, including those with ST-elevation, ST-depression, and BBB. For example, the ISIS-2 trial (19) randomized 17,187 subjects within 24 hours after the onset of suspected AMI to streptokinase alone, aspirin alone, streptokinase plus aspirin, or placebo in addition to usual care. BBB (left or right) was present in 1,032 (6%) of subjects at randomization; those with BBB had numerically lower rates of death with each intervention versus placebo (83 vs. 102, 74 vs. 111, and 29 vs. 57 in the streptokinase, aspirin, and streptokinase plus aspirin groups, respectively). The GISSI trial (20) randomized 11,802 subjects with suspected AMI to streptokinase or usual care, with BBB observed in 661 (5.6%) subjects; 21-day mortality was no different between subjects with BBB receiving streptokinase (8%) versus those receiving placebo (8.6%), with a relative risk of 0.92 (95% CI 0.53–1.60).
An analysis of pooled data from 9 fibrinolytic trials including over 58,000 patients with suspected AMI, including both patients with ST-elevation myocardial infarction (STEMI) and those with BBB, provided more statistical power for evaluation of subgroups with BBB (Table 2). Subjects with BBB (n=2,146) treated with early fibrinolysis had lower mortality (18.7% vs. 23.6%) than those treated with placebo, although the overall benefit was offset by an increase in stroke (2.1% vs. 1.1%) and major bleeding (1.3% vs. 0.3%) (21). These data form the basis for the current recommendations to treat new or presumed new LBBB as a “STEMI-equivalent” requiring urgent reperfusion therapy. However, an important limitation not frequently recognized is that the primary analysis on which these recommendations are based did not differentiate between the type or chronicity of bundle branch block and subjects with BBB represented only 3.6% of the total cohort.
Table 2.
Clinical outcomes in patients with BBB in randomized controlled trials of intravenous fibrinolytic therapy vs. standard care in AMI*
| Patient Population | Death, no. (%) | Stroke, no. (%) | Bleeding, no. (%) | |||
|---|---|---|---|---|---|---|
|
| ||||||
| Fibrinolytic | Control | Fibrinolytic | Control | Fibrinolytic | Control | |
|
|
||||||
| All patients (n=58,600) | 2,820 (9.6) | 3,357 (11.5) | 340 (1.2) | 224 (0.8) | 325 (1.1) | 111 (0.4) |
| Patients with BBB† (n=2,146) | 188 (18.7) | 242 (23.6) | 21 (2.1) | 11 (1.1) | 13 (1.3) | 3 (0.3) |
Data from FTT Collaborative Group (21)
Includes patients with both LBBB and RBBB
AMI=acute myocardial infarction; BBB=bundle branch block; LBBB=left bundle branch block; RBBB=right bundle branch block
Data from more recent fibrinolytic trials, with specific inclusion criteria for patients with presumed new LBBB, provide more direct comparisons of outcomes between STEMI and LBBB. For example, the HERO-2 trial demonstrated that patients with new or presumed new LBBB had a lower incidence of enzymatically confirmed AMI (80.7% vs. 88.7%, p=0.006) and lower 30-day mortality (16% vs. 22.7%, p=0.027) than matched STEMI-controls. Differences were observed, however, between LBBB patients with and without Sgarbossa ST-segment concordance criteria: those without concordance had a lower adjusted risk of 30-day mortality compared with STEMI (odds ratio 0.52, 95% CI 0.33–0.80), whereas those meeting concordance criteria had a similar risk (odds ratio 1.37, 95% CI 0.78–2.47) (22). Similarly, in the ASSENT 2 and 3 trials, 37.5% of LBBB vs. 15.6% of STEMI patients (p<0.001) did not have AMI enzymatically confirmed, and mortality was found to differ between patients with and without Sgarbossa concordance. In this analysis, the adjusted relative risk of mortality at 1-year among patients with LBBB and Sgarbossa concordance (score ≥ 3) compared with STEMI was 3.8 (95% CI 2.17–6.78); however, those with LBBB but without ST-segment concordance had a similar risk of 1-year mortality compared with STEMI patients (relative risk 0.91, 95% CI 0.47–1.77) (23). It should be noted that enrollment in these trials required a high clinical suspicion for AMI and, nevertheless, a substantially higher proportion of LBBB patients did not have AMI confirmed, especially among those without concordant ECG changes. Taken together, these data suggest that 1) patients with LBBB have heterogeneous outcomes with fibrinolytic therapy due, in part, to the significant variability in AMI incidence among this group and 2) Sgarbossa concordance on ECG may identify a high-risk population with similar (or worse) outcomes compared with STEMI.
More contemporary trials comparing the use of primary PCI with fibrinolysis have not provided much additional information regarding the benefit of urgent reperfusion strategies in patients with LBBB. Although the clinical superiority of primary PCI over fibrinolysis has been established, there are limited randomized trial data comparing the two therapies in patients with LBBB. Only 7 of the 23 trials reported in the meta-analysis by Keeley et al. (24) included patients with LBBB; efficacy or safety outcomes in patient sub-groups with LBBB have not been reported from these trials, and the largest trial to date specifically excluded such patients (25). Thus, randomized clinical trial data establishing a clear benefit of urgent reperfusion therapy in patients with LBBB in the modern era is lacking.
Clinical Controversies
The initial rationale for using ST-elevation on the ECG as a decision point for early reperfusion therapy in patients with suspected ACS was the high specificity for identifying patients who had complete occlusion of a coronary artery and who were most likely to benefit from treatment with a fibrinolytic agent. In this regard, a new (or presumably new) LBBB was thought to be equivalent to ST-elevation. However, recent data have called into question the principle that suspected ACS with a new or presumed new LBBB should be treated as a “STEMI-equivalent.” In the fibrinolytic era, a diagnosis of AMI was typically not confirmed angiographically, but rather biochemically with creatine kinase (CK) and/or CK-myocardial band. As primary PCI became more feasible, a larger number of studies have been able to confirm AMI angiographically. Overall, these studies have demonstrated that less than half of all patients with suspected ACS and LBBB will ultimately be diagnosed with an AMI (Table 1). Moreover, a significant proportion of those patients with AMI will not have an occluded culprit artery at catheterization and thus are more appropriately classified as having a non-ST-elevation myocardial infarction (NSTEMI), unstable angina, or non-ACS presentation (Table 3). This has important implications for the treatment of patients with presumed new LBBB who do not have immediate access to coronary angiography. If many of the patients with LBBB do not have AMI, they are unlikely to benefit from early reperfusion therapy. In addition, fibrinolytics have been shown to offer no benefit, and in fact may be harmful, to patients with NSTEMI (26).
Table 3.
Prevalence of “STEMI-equivalent” AMI in angiographic studies of patients with suspected ACS and LBBB
| Study | Year | No. of patients with occluded culprit artery/total with LBBB (%) | |
|---|---|---|---|
| New or presumed new LBBB | Old LBBB | ||
| Larson et al. (35) | 2007 | 20/36 (56) | n/a |
| Chang et al. (31) | 2009 | 4/55 (7) | 7/136 (5) |
| Lopes et al. (36) | 2011 | 60/98 (61) | n/a |
| Jain et al. (42) | 2011 | 5/36 (14) | n/a |
|
| |||
| Total (n=4) | 89/225 (40) | 7/136 (5) | |
ACS=acute coronary syndrome; AMI= acute myocardial infarction; LBBB= left bundle branch block; n/a=not applicable; STEMI= ST-elevation myocardial infarction
The significant variability in the prevalence of AMI complicated by LBBB reported in prior studies may be partially explained by diagnostic criteria with poor specificity for AMI. Since circulating biochemical markers of myocardial necrosis can be associated with structural heart disease, heart failure, kidney disease, and other co-morbid conditions (27–28), patients with LBBB may have been previously misclassified as AMI based solely on biochemical testing. Moreover, as elevated cardiac biomarkers are associated with greater risk in many non-ACS conditions compared with ACS (29), it is likely that a some of the excess risk associated with LBBB reflects co-morbid conditions not related to incident LBBB.
In addition to the more accurate classification of AMI in the primary PCI era, it is also possible that the distribution of new vs. old LBBB has changed. For example, in two reports from the 1970's, the proportion of AMI patients with new (compared with old) LBBB ranged from 53–61% (7, 30). In contrast, a recent study by Chang et al. reported that new LBBB was observed in only 29% of LBBB patients (31). As patients hospitalized with myocardial infarction are increasingly older, more likely to be female, have co-existing conditions such as hypertension, dyslipidemia, and diabetes mellitus, and have undergone previous coronary revascularization (32), the prevalence of chronic LBBB is likely increasing despite a general decline in overall incident STEMI. This phenomenon suggests that chronic LBBB may have become more common while incident LBBB in AMI has decreased, due to longer life expectancy and better survival for patients with heart failure and other co-existing conditions (33). Furthermore, other studies have demonstrated no difference in the prevalence of AMI between patients with chronic LBBB and new or presumed new LBBB (31, 34), suggesting that true MI-associated LBBB is indeed rare.
As pressures to reduce reperfusion times have increased, and acute cardiac care -- both in the emergency department and in the ambulance -- is increasingly driven by protocol, LBBB of unknown duration has emerged as a frequent reason for “false activation” of the cardiac catheterization laboratory for primary PCI. In this setting, a false activation is defined as an activation in which the coronary angiogram does not identify a culprit artery consistent with STEMI. Since only a minority of patients with LBBB are ultimately diagnosed with AMI, false-positive cardiac catheterization laboratory activation is frequent. In a single center study of 1335 patients, Larson et al. (35) reported that the prevalence of false-positive catheterization laboratory activation was 14% overall, but among patients presenting with LBBB, the rate of false activation was 44%. These findings have been confirmed in a recent PCI study demonstrating that 39% of the 98 patients with new LBBB, the majority of whom even had concordant ST-segment changes on ECG, did not have an occluded culprit coronary artery at angiography (36). In our experience it is not uncommon for catheterization laboratory activation to occur in patients with atypical chest pain or evidence of new onset heart failure, in whom a LBBB is present but cannot be confirmed to be old.
Urgent catheterization for “all-comers” can lead to an increased risk of complications related to the invasive procedure, resulting in prolonged hospital length of stay and higher costs, and decreased quality of life for providers (37). In centers where primary PCI is not readily available, these issues are obviously more concerning given the risks of bleeding, particularly intracranial hemorrhage, with fibrinolytic therapy; the risks of fibrinolytic therapy may be magnified in patients with LBBB who are generally older and have higher rates of hypertension. Alternatively, given that patients with LBBB are less likely to receive reperfusion therapy (due to co-morbid conditions or lack of diagnostic accuracy of the ECG), there is appropriate concern that delays in diagnosis and therapy may lead to missed opportunities to reduce morbidity and mortality in patients with LBBB and true AMI (38). For example, a decision analysis found that routine administration of fibrinolytic therapy to all patients with LBBB and possible AMI would result in a small but significant mortality reduction; however, this approach could lead to unnecessary administration of fibrinolytic therapy to the majority of patients who do not have AMI (39). It should be noted that this analysis was performed over 10 years ago, based on epidemiological data suggesting a higher proportion of “STEMI-equivalent” AMI in patients with LBBB than appears to be the case today. In the modern era, the risk-benefit ratio may be even less favorable. Therefore, as systems of care improve and delays in transfer for primary PCI decrease, applying a routine transfer strategy for patients with suspected AMI and LBBB may preserve the benefit of reperfusion therapy for the highest risk patients while minimizing potential harm associated with administering fibrinolytic therapy to patients without occluded arteries.
Do the Sgarbossa Criteria help?
The Sgarbossa criteria (13) as proposed in 1996 are listed in Table 4 and include ST-segment elevation ≥ 1mm concordant with the QRS complex in any lead, ST-segment depression ≥ 1mm in lead V1, V2, or V3, and ST-segment elevation ≥ 5mm discordant with the QRS complex in any lead (Figure 2). These criteria are weighted differently to reflect their varied estimated probability for AMI diagnosis. The original study by Sgarbossa et al. (13) reported that the ST-segment concordance criteria (score ≥ 3) were the most accurate for AMI diagnosis. The authors found that ST-segment discordance (score of 2) was of limited value due to poor specificity and suggested that patients presenting with ST-segment discordance alone should undergo further diagnostic testing. Several prospective studies and a recent meta-analysis have generally concluded that the Sgarbossa criteria, with the exception of discordant ST-segment elevation, are highly specific for the diagnosis of AMI in the setting of LBBB, have good inter-observer agreement (κ=0.81), and have similar utility whether the LBBB is new or old (40). Recent validation studies have confirmed that a Sgarbossa score of ≥ 3 (requiring either concordant ST-segment elevation ≥ 1mm or ST-segment depression ≥ 1mm in lead V1, V2, or V3) has specificity for AMI greater than 95% and is associated with higher 30-day mortality compared with LBBB patients with discordant ST-segment elevation alone (22–23, 41). For example, Kontos et al. studied 401 patients in the emergency department with suspected AMI and found that ST-segment concordant elevation or depression was an independent predictor of AMI (odds ratio 17.0, 95% CI 3.4–81, p<0.001) and 30-day mortality (odds ratio 4.3, 95% CI 1.3–15, p=0.02) (34). Other studies have concluded that ST-segment elevation concordance is the single most specific criterion for the diagnosis of AMI and improves identification of individuals who will develop positive cardiac biomarkers or whom have an occluded culprit-artery on angiography (i.e. “STEMI-equivalent”) (36, 42). However, although use of these ECG criteria improves diagnostic specificity and may decrease false-positive AMI diagnoses, concern appropriately exists over a lack of sensitivity (15), as the sensitivity of a Sgarbossa score of ≥ 3 is only approximately 20% (41). Moreover, other studies suggest that there may be no improvement over clinical judgment alone (43), and some investigators have even advocated for additional ECG criteria to improve sensitivity. For example, Smith and Dodd found “excessive discordance” on ECG, defined as a ratio of ST-elevation to S-wave amplitude of ≤ −0.20, to be 84% sensitive and 99% specific for LAD occlusion in 148 patients with LBBB and suspected AMI (44).
Table 4.
Sgarbossa electrocardiographic criteria for the diagnosis of evolving AMI in the presence of LBBB*

|
Data from Tabas et al. (41); sensitivity, specificity, positive and negative likelihood ratios are presented as summary statistics (95% CI) for scores ≥ 3 and ≥ 2.
ST-segment deviation is measured at the J point. Concordance and discordance of ST segments are determined by comparison to the main direction of the QRS complex.
AMI= acute myocardial infarction; LBBB= left bundle branch block
Figure 2. Electrocardiograms Demonstrating the Three Sgarbossa Criteria for the Diagnosis of Acute Myocardial Infarction in a Patient with LBBB.

Panel A: The ECG shows ST-segment elevation of at least 1 mm that is concordant with the QRS complex (arrows, leads V5 and V6) and ST-segment elevation of at least 5 mm that is discordant with the QRS complex (arrow, lead V3); Panel B: The ECG shows ST-segment depression of at least 1 mm in leads V2 and V3 (arrows). ECGs used with permission courtesy of ECGpedia.org.
ECG=electrocardiogram; LBBB=left bundle branch block
Future Strategies
Given the substantial gap between recent evidence and current recommendations, new diagnostic strategies are needed to guide the selection of appropriate patients with suspected AMI and LBBB for urgent reperfusion therapy. The clinical need is greater in centers without on-site primary PCI, since the implications of false catheterization laboratory activation are not as significant as unnecessary administration of fibrinolytic therapy. Potential strategies include differential algorithms for transfer to primary PCI centers for patients with LBBB compared with those who have ST-elevation and normal conduction, use of more specific ECG criteria, increased use of cardiac biomarkers including sensitive assays for cardiac troponins, and bedside echocardiography to improve diagnostic accuracy and timely intervention.
Transfer for primary PCI in patients presenting with STEMI is equivalent or superior to fibrinolytic therapy as long as the overall first medical contact-to-balloon time is within 120 minutes (45–46). In general, if the anticipated time to reperfusion will exceed this threshold, on-site fibrinolytic therapy is recommended. However, since a substantial proportion of patients with LBBB do not have a “STEMI-equivalent” AMI, and patients with LBBB have an overall higher risk of bleeding (more likely female, older, with pre-existing cardiovascular disease, hypertension, and congestive heart failure), transfer for primary PCI may be the preferred strategy, with judicious use of on-site fibrinolysis reserved for patients highly likely to have a “STEMI-equivalent” AMI when PCI is not available. This approach seems particularly attractive for most LBBB patients, as the risk-benefit calculation in such patients may favor primary PCI even when the delay associated with transfer for primary PCI exceeds 90 minutes (47). Additionally, as pre-hospital triage of chest pain patients by emergency medical services evolves, patients with LBBB may be recognized immediately and preferentially routed to a PCI-capable hospital, as long as delays are within acceptable time limits.
The use of cardiac biomarkers, specifically the cardiac troponins I and T, holds additional promise in the diagnosis of AMI with LBBB. In recent years, the analytic sensitivity for detection of cardiac troponins has improved 100-fold (48). Newer assays have improved precision as well, which enables two cardiac troponin values with a difference as small as a few pg/mL to be reliably differentiated. This is important because while small cardiac troponin elevations can be measured in many chronic cardiac and non-cardiac conditions, and thus lack specificity for AMI, a rise in absolute levels of troponin strongly supports the diagnosis of an evolving AMI (49). A rapid rise in troponin on serial measurement in a patient with LBBB, especially in the setting of ongoing chest discomfort, could represent a “masked” STEMI and prompt additional diagnostic testing such as bedside echocardiography (see below), an invasive angiographic approach, or administration of fibrinolytic therapy if PCI is not available. In contrast, a more gradual rise and lower peak in troponin levels may signal a NSTEMI (in which case transfer to a PCI capable facility would still typically be recommended), whereas a static troponin level would suggest a non-ACS etiology. Although few data are available, it is becoming increasingly more feasible to accelerate the timing of serial biomarker assessment, such that measurements are performed every 15 minutes rather than every 60–90 minutes in patients with LBBB and suspected AMI. Such an approach would minimize reperfusion delays in those ultimately determined to have “STEMI equivalents.” Assessment of rapid biomarker measurements, ideally performed at the point of care (POC), should be the focus of additional study in patients with suspected AMI and LBBB.
Finally, bedside echocardiography may be used as an adjunctive measure in clinically complex situations to gain additional insight as to whether a new or presumed new LBBB is due to a “STEMI-equivalent” ACS presentation. Point-of-care “pocket-sized” echocardiographic devices can be used by emergency medicine physicians and cardiologists and have been shown to have high feasibility and reliability in the assessment of cardiac structure and function (50). The presence of significant cardiac chamber dilatation, wall thinning, or chronic valvular dysfunction in the absence of an acute anterior wall motion abnormality would suggest that the LBBB is more likely secondary to chronic cardiac disease than AMI. Alternatively, evidence of a hypo- or akinetic segmental wall motion abnormality in the anterior wall, in the absence of evidence of a prior infarction (wall thinning, chamber dilatation), may represent a “STEMI-equivalent” AMI and should prompt emergent coronary angiography. In fact, use of portable echocardiography to clarify the diagnosis of STEMI, especially if confounded by LBBB, has a class IIa indication in the most recent ACC/AHA guidelines (51). Thus, rapid beside echocardiography represents another potential strategy for improved clinical decision-making in patients with suspected AMI and LBBB and may be used in conjunction with the other methods described above.
Investigators have recently proposed changes to the current ACC/AHA guidelines for the management of patients with suspected ACS and LBBB, based on the limited randomized trial data demonstrating efficacy of reperfusion therapy in this subgroup. These include demotion of the Class I-A recommendation that new or presumed new LBBB be treated as a “STEMI-equivalent” and a proposal that most patients with LBBB be evaluated for ST-segment concordance on ECG and positive cardiac biomarkers to determine the need for urgent reperfusion therapy (37). We also propose an algorithm for the diagnosis and management of these patients (Figure 3) that includes a rapid clinical and ECG assessment. Clinically or hemodynamically unstable patients with possible AMI and LBBB should be considered for immediate reperfusion therapy. Among stable patients, ECG assessment should be performed to determine the presence or absence of ST-segment concordance criteria in both new and chronic LBBB. Patients meeting ST-segment concordance criteria should be treated as a “STEMI equivalent” and receive urgent reperfusion therapy. If concordance criteria are absent, rapid serial cardiac biomarker testing and/or bedside echocardiography should be considered. If biomarkers increase in the presence of ongoing symptoms, or a large wall motion abnormality in the anterior wall is seen, emergent angiography should be performed, recognizing that many of these individuals will still have NSTEMI- rather than STEMI-equivalents as our current clinical tools are insufficient to distinguish between the two entities when evidence of infarction is present. Given the low positive predictive value of LBBB, we recommend that patients with LBBB and possible ACS be routinely transferred to a PCI-capable hospital; fibrinolytic therapy should only be considered if the diagnosis is highly likely (i.e. meeting Sgarbossa criteria) or the patient is hemodynamically unstable and transfer to a PCI-capable facility would result in marked treatment delay. This algorithm would ensure that urgent reperfusion is delivered to the highest-risk patients with the greatest likelihood of acute thrombotic coronary occlusion while taking a more deliberate approach to diagnosis among individuals in whom the clinical picture is less clear. Ideally, such a strategy would result in only small treatment delays in patients with “STEMI-equivalents”, and would be balanced by less exposure to risk for the larger proportion of patients with non-ST-elevation ACS or non-ACS diagnoses.
Figure 3. Proposed Diagnostic Algorithm for Suspected Myocardial Infarction and LBBB.

ACS=acute coronary syndrome; LBBB=left bundle branch block; NSTEMI=non-ST-elevation myocardial infarction; PCI=percutaneous coronary intervention; STEMI=ST-elevation myocardial infarction; UA=unstable angina
Given the significant advancements in efficacy and safety of AMI treatments and the lack of contemporary evidence for the existing approach to LBBB, more research encompassing additional diagnostic and therapeutic strategies is needed. Due to the difficulty of diagnosing AMI resulting from acute coronary vessel occlusion, inclusion of LBBB in overall STEMI quality reporting (e.g. door-to-balloon times and other metrics) should also be reconsidered in light of the low specificity and positive predictive value of LBBB for “STEMI-equivalent” AMI. Removal of LBBB as an automatic STEMI-equivalent would provide more specific and accurate evaluation of systems of care and quality of outcomes in STEMI. Therefore, as we evolve toward improved quality of care and better outcomes for patients, management of patients with LBBB and suspected AMI should evolve as well to reflect changing epidemiology, new observational and clinical trial data, advances in technology, and continued high-quality evidence-based research.
Conclusion
Patients with a suspected ACS in the setting of LBBB represent a much more heterogeneous population than STEMI without BBB, and present unique diagnostic and therapeutic challenges to the clinician. The majority of patients will not have an AMI regardless of LBBB chronicity and likely would not benefit from urgent reperfusion therapy. Current guideline recommendations and performance measures do not account for the evolving epidemiology and complexity of LBBB among patients with possible ACS. We recommend a slightly more judicious approach to diagnosis among hemodynamically and clinically stable patients with LBBB who do not have ECG findings highly specific for STEMI. Moreover, we recommend a higher threshold for pharmacological reperfusion than primary PCI, given the lower probability of an occluded culprit artery and the bleeding risks of fibrinolytic therapy. The full impact of this approach, with regard to appropriateness and timeliness of therapy, as well as outcomes, requires prospective study.
Acknowledgments
Funding Sources
This work was supported by Award Number T32HL007360 from the National Heart, Lung, and Blood Institute to Dr. Neeland.
Disclosures
Dr. de Lemos has received grant support from Roche Diagnostics and Abbott Diagnostics, lecture honoraria from BMS/Sanofi-Aventis, and consulting income from AstraZeneca. Dr. Kontos has received lecture honoraria from Sanofi-Aventis, Astellas, and AstraZeneca, and consulting income from Sanofi-Aventis, Astellas, and AstraZeneca.
Abbreviations:
- ACS
acute coronary syndrome
- AMI
acute myocardial infarction
- BBB
bundle branch block
- ECG
electrocardiogram
- LBBB
left bundle branch block
- NSTEMI
non-ST-elevation myocardial infarction
- PCI
percutaneous coronary intervention
- RBBB
right bundle branch block
- STEMI
ST-elevation myocardial infarction
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Bansilal S, Aneja A, Mathew V, et al. Long-term cardiovascular outcomes in patients with angina pectoris presenting with bundle branch block. Am J Cardiol. 2011;107:1565–70. doi: 10.1016/j.amjcard.2011.01.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Go AS, Barron HV, Rundle AC, Ornato JP, Avins AL. Bundle-branch block and inhospital mortality in acute myocardial infarction. National Registry of Myocardial Infarction 2 Investigators. Ann Intern Med. 1998;129:690–7. doi: 10.7326/0003-4819-129-9-199811010-00003. [DOI] [PubMed] [Google Scholar]
- 3.Cannon CP, McCabe CH, Stone PH, et al. The electrocardiogram predicts one-year outcome of patients with unstable angina and non-Q wave myocardial infarction: results of the TIMI III Registry ECG Ancillary Study. Thrombolysis in Myocardial Ischemia. J Am Coll Cardiol. 1997;30:133–40. doi: 10.1016/s0735-1097(97)00160-5. [DOI] [PubMed] [Google Scholar]
- 4.Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction; A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction) J Am Coll Cardiol. 2004;44:E1–E211. doi: 10.1016/j.jacc.2004.07.014. [DOI] [PubMed] [Google Scholar]
- 5.Van de Werf F, Bax J, Betriu A, et al. Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: the Task Force on the Management of ST-Segment Elevation Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J. 2008;29:2909–45. doi: 10.1093/eurheartj/ehn416. [DOI] [PubMed] [Google Scholar]
- 6.Godman MJ, Lassers BW, Julian DG. Complete bundle-branch block complicating acute myocardial infarction. N Engl J Med. 1970;282:237–40. doi: 10.1056/NEJM197001292820502. [DOI] [PubMed] [Google Scholar]
- 7.Hindman MC, Wagner GS, JaRo M, et al. The clinical significance of bundle branch block complicating acute myocardial infarction. 1. Clinical characteristics, hospital mortality, and one-year follow-up. Circulation. 1978;58:679–88. doi: 10.1161/01.cir.58.4.679. [DOI] [PubMed] [Google Scholar]
- 8.Bauer GE. Development of Bundle Branch Block. Am J Cardiol. 1964;14:346–51. doi: 10.1016/0002-9149(64)90077-3. [DOI] [PubMed] [Google Scholar]
- 9.Oppenheimer BS, Rothschild MA. Electrocardiographic changes associated with myocardial involvement: with special reference to prognosis. JAMA. 1917;69:429–431. [Google Scholar]
- 10.Bauer GE, Julian DG, Valentine PA. Bundle-branch block in acute myocardial infarction. Br Heart J. 1965;27:724–30. doi: 10.1136/hrt.27.5.724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sgarbossa EB. Value of the ECG in suspected acute myocardial infarction with left bundle branch block. J Electrocardiol. 2000;33(Suppl):87–92. doi: 10.1054/jelc.2000.20324. [DOI] [PubMed] [Google Scholar]
- 12.Wellens HJ. Acute myocardial infarction and left bundle-branch block--can we lift the veil? N Engl J Med. 1996;334:528–9. doi: 10.1056/NEJM199602223340809. [DOI] [PubMed] [Google Scholar]
- 13.Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators. N Engl J Med. 1996;334:481–7. doi: 10.1056/NEJM199602223340801. [DOI] [PubMed] [Google Scholar]
- 14.Kontos MC, McQueen RH, Jesse RL, Tatum JL, Ornato JP. Can myocardial infarction be rapidly identified in emergency department patients who have left bundle-branch block? Ann Emerg Med. 2001;37:431–8. doi: 10.1067/mem.2001.114900. [DOI] [PubMed] [Google Scholar]
- 15.Li SF, Walden PL, Marcilla O, Gallagher EJ. Electrocardiographic diagnosis of myocardial infarction in patients with left bundle branch block. Ann Emerg Med. 2000;36:561–5. doi: 10.1067/mem.2000.108079. [DOI] [PubMed] [Google Scholar]
- 16.Stenestrand U, Tabrizi F, Lindback J, Englund A, Rosenqvist M, Wallentin L. Comorbidity and myocardial dysfunction are the main explanations for the higher 1-year mortality in acute myocardial infarction with left bundle-branch block. Circulation. 2004;110:1896–902. doi: 10.1161/01.CIR.0000143136.51424.38. [DOI] [PubMed] [Google Scholar]
- 17.Sgarbossa EB, Pinski SL, Topol EJ, et al. Acute myocardial infarction and complete bundle branch block at hospital admission: clinical characteristics and outcome in the thrombolytic era. GUSTO-I Investigators. Global Utilization of Streptokinase and t-PA [tissue-type plasminogen activator] for Occluded Coronary Arteries. J Am Coll Cardiol. 1998;31:105–10. doi: 10.1016/s0735-1097(97)00446-4. [DOI] [PubMed] [Google Scholar]
- 18.Yeo KK, Li S, Amsterdam EA, et al. Comparison of clinical characteristics, treatments and outcomes of patients with ST-elevation acute myocardial infarction with versus without new or presumed new left bundle branch block (from NCDR®) Am J Cardiol. 2012;109:497–501. doi: 10.1016/j.amjcard.2011.09.040. [DOI] [PubMed] [Google Scholar]
- 19.Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Lancet. 1988;2:349–60. [PubMed] [Google Scholar]
- 20.Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Gruppo Italiano per lo Studio della Streptochinasi nell'Infarto Miocardico (GISSI) Lancet. 1986;1:397–402. [PubMed] [Google Scholar]
- 21.Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Fibrinolytic Therapy Trialists' (FTT) Collaborative Group. Lancet. 1994;343:311–22. [PubMed] [Google Scholar]
- 22.Wong CK, French JK, Aylward PE, et al. Patients with prolonged ischemic chest pain and presumed-new left bundle branch block have heterogeneous outcomes depending on the presence of ST-segment changes. J Am Coll Cardiol. 2005;46:29–38. doi: 10.1016/j.jacc.2005.02.084. [DOI] [PubMed] [Google Scholar]
- 23.Al-Faleh H, Fu Y, Wagner G, et al. Unraveling the spectrum of left bundle branch block in acute myocardial infarction: insights from the Assessment of the Safety and Efficacy of a New Thrombolytic (ASSENT 2 and 3) trials. Am Heart J. 2006;151:10–5. doi: 10.1016/j.ahj.2005.02.043. [DOI] [PubMed] [Google Scholar]
- 24.Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13–20. doi: 10.1016/S0140-6736(03)12113-7. [DOI] [PubMed] [Google Scholar]
- 25.Andersen HR, Nielsen TT, Rasmussen K, et al. A comparison of coronary angioplasty with fibrinolytic therapy in acute myocardial infarction. N Engl J Med. 2003;349:733–42. doi: 10.1056/NEJMoa025142. [DOI] [PubMed] [Google Scholar]
- 26.Effects of tissue plasminogen activator and a comparison of early invasive and conservative strategies in unstable angina and non-Q-wave myocardial infarction. Results of the TIMI IIIB Trial. Thrombolysis in Myocardial Ischemia. Circulation. 1994;89:1545–56. doi: 10.1161/01.cir.89.4.1545. [DOI] [PubMed] [Google Scholar]
- 27.Wallace TW, Abdullah SM, Drazner MH, et al. Prevalence and determinants of troponin T elevation in the general population. Circulation. 2006;113:1958–65. doi: 10.1161/CIRCULATIONAHA.105.609974. [DOI] [PubMed] [Google Scholar]
- 28.Jeremias A, Gibson CM. Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med. 2005;142:786–91. doi: 10.7326/0003-4819-142-9-200505030-00015. [DOI] [PubMed] [Google Scholar]
- 29.Alcalai R, Planer D, Culhaoglu A, Osman A, Pollak A, Lotan C. Acute coronary syndrome vs nonspecific troponin elevation: clinical predictors and survival analysis. Arch Intern Med. 2007;167:276–81. doi: 10.1001/archinte.167.3.276. [DOI] [PubMed] [Google Scholar]
- 30.Gann D, Balachandran PK, Sherif NE, Samet P. Prognostic significance of chronic versus acute bundle branch block in acute myocardial infarction. Chest. 1975;67:298–303. doi: 10.1378/chest.67.3.298. [DOI] [PubMed] [Google Scholar]
- 31.Chang AM, Shofer FS, Tabas JA, Magid DJ, McCusker CM, Hollander JE. Lack of association between left bundle-branch block and acute myocardial infarction in symptomatic ED patients. Am J Emerg Med. 2009;27:916–21. doi: 10.1016/j.ajem.2008.07.007. [DOI] [PubMed] [Google Scholar]
- 32.Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS. Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362:2155–65. doi: 10.1056/NEJMoa0908610. [DOI] [PubMed] [Google Scholar]
- 33.Jolobe OM. Bundle branch block old and new in myocardial infarction. Am J Emerg Med. 2010;28:749, e5. doi: 10.1016/j.ajem.2009.11.001. [DOI] [PubMed] [Google Scholar]
- 34.Kontos MC, Aziz HA, Chau VQ, Roberts CS, Ornato JP, Vetrovec GW. Outcomes in patients with chronicity of left bundle-branch block with possible acute myocardial infarction. Am Heart J. 2011;161:698–704. doi: 10.1016/j.ahj.2011.01.008. [DOI] [PubMed] [Google Scholar]
- 35.Larson DM, Menssen KM, Sharkey SW, et al. “False-positive” cardiac catheterization laboratory activation among patients with suspected ST-segment elevation myocardial infarction. JAMA. 2007;298:2754–60. doi: 10.1001/jama.298.23.2754. [DOI] [PubMed] [Google Scholar]
- 36.Lopes RD, Siha H, Fu Y, et al. Diagnosing acute myocardial infarction in patients with left bundle branch block. Am J Cardiol. 2011;108:782–8. doi: 10.1016/j.amjcard.2011.05.006. [DOI] [PubMed] [Google Scholar]
- 37.Rokos IC, French WJ, Mattu A, et al. Appropriate cardiac cath lab activation: optimizing electrocardiogram interpretation and clinical decision-making for acute ST-elevation myocardial infarction. Am Heart J. 2010;160:995–1003. e1–8. doi: 10.1016/j.ahj.2010.08.011. [DOI] [PubMed] [Google Scholar]
- 38.Barron HV, Bowlby LJ, Breen T, et al. Use of reperfusion therapy for acute myocardial infarction in the United States: data from the National Registry of Myocardial Infarction 2. Circulation. 1998;97:1150–6. doi: 10.1161/01.cir.97.12.1150. [DOI] [PubMed] [Google Scholar]
- 39.Shlipak MG, Lyons WL, Go AS, Chou TM, Evans GT, Browner WS. Should the electrocardiogram be used to guide therapy for patients with left bundle-branch block and suspected myocardial infarction? JAMA. 1999;281:714–9. doi: 10.1001/jama.281.8.714. [DOI] [PubMed] [Google Scholar]
- 40.Sokolove PE, Sgarbossa EB, Amsterdam EA, et al. Interobserver agreement in the electrocardiographic diagnosis of acute myocardial infarction in patients with left bundle branch block. Ann Emerg Med. 2000;36:566–71. doi: 10.1067/mem.2000.112077. [DOI] [PubMed] [Google Scholar]
- 41.Tabas JA, Rodriguez RM, Seligman HK, Goldschlager NF. Electrocardiographic criteria for detecting acute myocardial infarction in patients with left bundle branch block: a meta-analysis. Ann Emerg Med. 2008;52:329–36. e1. doi: 10.1016/j.annemergmed.2007.12.006. [DOI] [PubMed] [Google Scholar]
- 42.Jain S, Ting HT, Bell M, et al. Utility of left bundle branch block as a diagnostic criterion for acute myocardial infarction. Am J Cardiol. 2011;107:1111–6. doi: 10.1016/j.amjcard.2010.12.007. [DOI] [PubMed] [Google Scholar]
- 43.Gunnarsson G, Eriksson P, Dellborg M. ECG criteria in diagnosis of acute myocardial infarction in the presence of left bundle branch block. Int J Cardiol. 2001;78:167–74. doi: 10.1016/s0167-5273(01)00378-3. [DOI] [PubMed] [Google Scholar]
- 44.Smith SW, Dodd KW. Letter to the Editor regarding “Outcomes in patients with chronicity of left bundle-branch block with possible acute myocardial infarction“. Am Heart J. 2011;162:e23. doi: 10.1016/j.ahj.2011.07.005. [DOI] [PubMed] [Google Scholar]
- 45.Dalby M, Bouzamondo A, Lechat P, Montalescot G. Transfer for primary angioplasty versus immediate thrombolysis in acute myocardial infarction: a meta-analysis. Circulation. 2003;108:1809–14. doi: 10.1161/01.CIR.0000091088.63921.8C. [DOI] [PubMed] [Google Scholar]
- 46.Levine GN, Bates ER, Blankenship JC, et al. ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2011;124:2574–609. doi: 10.1161/CIR.0b013e31823a5596. 2011. [DOI] [PubMed] [Google Scholar]
- 47.Pinto DS, Kirtane AJ, Nallamothu BK, et al. Hospital delays in reperfusion for ST-elevation myocardial infarction: implications when selecting a reperfusion strategy. Circulation. 2006;114:2019–25. doi: 10.1161/CIRCULATIONAHA.106.638353. [DOI] [PubMed] [Google Scholar]
- 48.Mahajan VS, Jarolim P. How to interpret elevated cardiac troponin levels. Circulation. 2011;124:2350–4. doi: 10.1161/CIRCULATIONAHA.111.023697. [DOI] [PubMed] [Google Scholar]
- 49.Reichlin T, Irfan A, Twerenbold R, et al. Utility of absolute and relative changes in cardiac troponin concentrations in the early diagnosis of acute myocardial infarction. Circulation. 2011;124:136–45. doi: 10.1161/CIRCULATIONAHA.111.023937. [DOI] [PubMed] [Google Scholar]
- 50.Andersen GN, Haugen BO, Graven T, Salvesen O, Mjolstad OC, Dalen H. Feasibility and reliability of point-of-care pocket-sized echocardiography. Eur J Echocardiogr. 2011;12:665–70. doi: 10.1093/ejechocard/jer108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction--executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients With Acute Myocardial Infarction) Circulation. 2004;110:588–636. doi: 10.1161/01.CIR.0000134791.68010.FA. [DOI] [PubMed] [Google Scholar]
- 52.Rude RE, Poole WK, Muller JE, et al. Electrocardiographic and clinical criteria for recognition of acute myocardial infarction based on analysis of 3,697 patients. Am J Cardiol. 1983;52:936–42. doi: 10.1016/0002-9149(83)90508-8. [DOI] [PubMed] [Google Scholar]
- 53.Fesmire FM, Percy RF, Wears RL, MacMath TL. Initial ECG in Q wave and non-Q wave myocardial infarction. Ann Emerg Med. 1989;18:741–6. doi: 10.1016/s0196-0644(89)80007-1. [DOI] [PubMed] [Google Scholar]
- 54.Otto LA, Aufderheide TP. Evaluation of ST segment elevation criteria for the prehospital electrocardiographic diagnosis fo acute myocardial infarction. Ann Emerg Med. 1994;23:17–24. doi: 10.1016/s0196-0644(94)70002-8. [DOI] [PubMed] [Google Scholar]
- 55.Kudenchuk PJ, Maynard C, Cobb LA, et al. Utility of the prehospital electrocardiogram in diagnosing acute coronary syndromes: the Myocardial Infarction Triage and Intervention (MITI) Project. J Am Coll Cardiol. 1998;32:17–27. doi: 10.1016/s0735-1097(98)00175-2. [DOI] [PubMed] [Google Scholar]
- 56.Edhouse JA, Sakr M, Angus J, Morris FP. Suspected myocardial infarction and left bundle branch block: electrocardiographic indicators of acute ischaemia. J Accid Emerg Med. 1999;16:331–5. doi: 10.1136/emj.16.5.331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Maynard SJ, Menown IB, Manoharan G, Allen J, Mc CAJ, Adgey AA. Body surface mapping improves early diagnosis of acute myocardial infarction in patients with chest pain and left bundle branch block. Heart. 2003;89:998–1002. doi: 10.1136/heart.89.9.998. [DOI] [PMC free article] [PubMed] [Google Scholar]