
Figure 1. Atrial Basket Positioning for Computational AF Mapping.
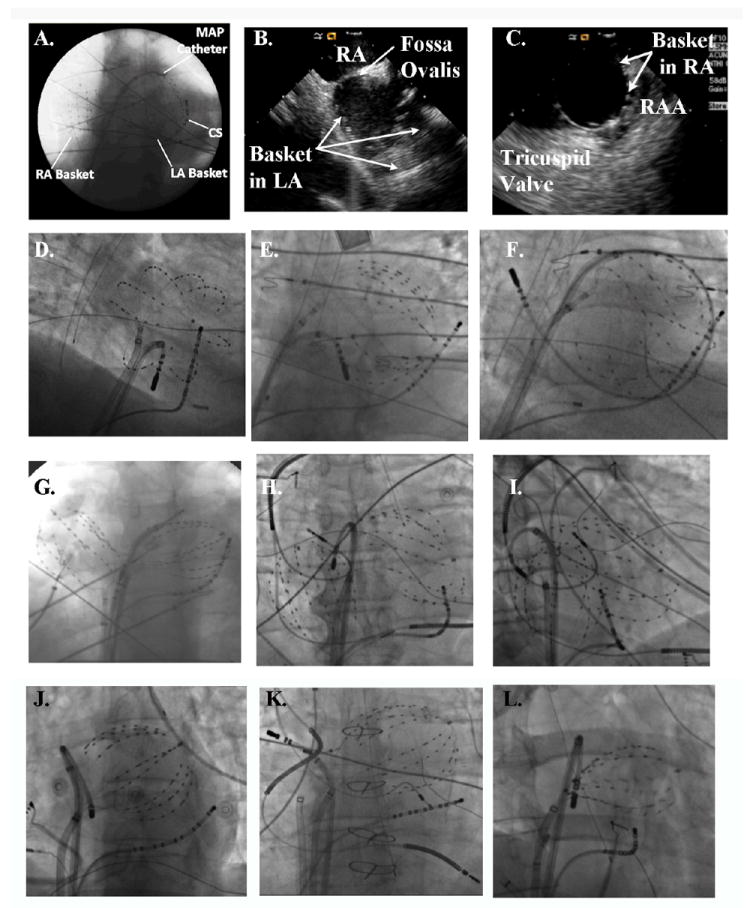
A. Good catheter placement in both atria (48 mm baskets, anteroposterior fluoroscopy), with MAP catheter at the left superior pulmonary vein antrum. B, C. Intracardiac Echocardiography confirms electrode opposition to walls of B. Left Atrium and C. Right Atrium. D. Good Electrode coverage of left atrium (60 mm Basket, RAO 30° fluoroscopy); E. Spline crowding detracts from otherwise good LA coverage (60 mm Basket, AP fluoroscopy); F. Large Left Atrium, With Poor Electrode Coverage of its Septum, outlined by ablation catheter loop with tip at right superior PV os (60 mm basket, LAO 30° fluoroscopy). G. Poor Coverage of Superior LA, indicated by wide separation of LA basket from the left main bronchus; the RA basket is well-deployed (60 mm baskets, AP fluoroscopy). H. Basket Placement With Pre-existing device leads. The RA basket is well positioned in this AP projection, yet the LA basket poorly covers the inferior LA. This appearance is consistent with basket displacement through the mitral apparatus. I. Anterior displacement of the LA basket through the mitral annulus, with the ablation catheter defining the true posterior border of the LA (same patient as panel H, in 30° RAO fluoroscopy). J. Undersized basket, despite an apparently good deployment, floating freely within the large left atrium that gave very poor signals and was replaced. K. Undersized basket in a patient with heart failure, a cardiac-resynchronization defibrillator and previously diagnosed ‘permanent AF’ now reclassified as longstanding persistent AF and undergoing ablation. L. Underexpanded basket, evident from the elliptical shape due to pinching at the interatrial septum. This was remedied by advancing the basket further into the left atrium with clockwise torque.