

Abstract
A 4-year-old, male Newfoundland cross was presented for lethargy, anorexia, and dysuria. The main clinical finding was an enlarged and painful prostate gland. While the dog was hospitalized, priapism developed. Following euthanasia, microscopic examination revealed that a carcinoma involving both bladder and prostate gland had widely metastasized to the penile vasculature.
A 4-year-old, intact, male Newfoundland cross, weighing 36 kg, was presented for anorexia, lethargy, melena, and urinary problems, including dysuria, stranguria, and hemorrhagic preputial discharge. Five days earlier, another veterinarian had tentatively diagnosed prostatitis and had prescribed ketoprofen (Anafen; Merial Canada, Baie D'Urfé, Quebec), 30 mg, PO, q24h for 4 d, and trimethoprim-sulfamethoxazole (Apo-Sulfatrim; Apotex, Weston, Ontario), 480 mg, PO, q12h for 10 d. The dog was recumbent, dehydrated, and depressed, and it had an enlarged and turgid bladder. On transrectal examination, the prostate appeared to be symmetrically enlarged and painful.
A urinary catheter was inserted and 2 L of urine removed. A complete blood cell (CBC) count revealed a stress leukogram, with mild neutrophilia (12.51 × 109/L; reference range, 3 to 11.5 × 109/L), moderate lymphopenia (0.41 × 109/L; reference range, 1.0 to 4.8 × 109/L), and normocytic, normochromic, nonregenerative anemia (hematocrit, 0.26; reference range, 0.37 to 0.55). Results from bacteriologic urine culture were negative. Treatment was instituted with lactated Ringer's solution, IV; enrofloxacin (Baytril; Bayer, Toronto, Ontario), 195 mg, IV, q24h; misoprostol (Cytotec; Searle, Mississauga, Ontario), 150 μg, PO, q12h; and sucralfate (Sulcrate; Aventis Pharma, Laval, Quebec), 1 g, PO, q12h.
Over the following 4 d, the dog became ambulatory and more responsive, but it was still weak and unwilling to eat and drink without encouragement. It was kept in hospital on the same treatment regimen. A radiograph of the caudal part of the abdomen confirmed an enlarged prostate. Another CBC count showed a slight improvement in the hematocrit (0.30) but persistent lymphopenia (0.30 × 109/L), which was still considered to be compatible with a stress leukogram. The owners declined referral for ultrasonography, biopsy, and exploratory surgery, for financial reasons.
By day 6 following presentation, the melena had resolved and the dog was drinking well on his own; therefore, the IV fluids, misoprostol, and sucralfate were discontinued, and oral treatment with enrofloxacin, 150 mg, q12h, was instituted. Although the prostate was not painful and was considerably smaller than when previously palpated, a soft, cavitated area was felt on its left side, and the dysuria, stranguria, and hemorrhagic preputial discharge persisted. In addition, priapism — a painful and erect penis with engorgement of the bulbus glandis — became evident.
On day 9 following presentation, a prostatic wash was performed, with the dog under sedation with butorphanol and diazepam. The fluid was submitted to the Atlantic Veterinary College for cytologic examination, which revealed moderate to marked neutrophilic inflammation and possible dysplastic changes in epithelial cells. A retrograde urethrogram and a double-contrast cystogram did not show any evidence of bladder abnormalities or urethral obstruction, but a notable reflux of contrast into the prostate could be seen. The dog was anesthetized with isoflurane and castrated, in an attempt to ameliorate any component of the prostatic hyperplasia that was secondary to endogenous androgens.
Eleven days following presentation, the dog was eating and drinking with encouragement but was still exhibiting priapism and could not urinate. The prostate was enlarged again and painful on transrectal palpation, and dark-brown diarrhea had again developed. Dexamethasone (Dexamethasone 2; Vétoquinol, Lavaltrie, Quebec), 3.6 mg, SC, q24h for 3 d, was administered in an attempt to reduce the prostatic and urethral inflammation, and oral treatment with misoprostol and sucralfate was resumed.
On day 15 after presentation, acepromazine (Acevet; Vétoquinol), 25 mg, PO, was administered to determine whether the dysuria could be the result of urethral spasm. After this treatment, the bulbus glandis appeared to be less engorged, but the dog remained unable to urinate. Soon after, bilateral epistaxis that was unresponsive to nasal epinephrine developed; it was interpreted to be due to disseminated intravascular coagulation. Owing to the deterioration in its condition, the lack of response to aggressive medical treatment, and the presumed grave prognosis, the owners elected to have the dog euthanized. The animal was sent to the Atlantic Veterinary College for postmortem examination.
At necropsy, the distended and turgid urinary bladder was found to contain a large amount of hemorrhagic urine mixed with a few blood clots. Close gross examination of the bladder revealed localized thickening of the vesical wall around the ureteric and urethral opening (trigone). Also, the bladder had a few irregular polypoid nodules, 0.5 to 2.0 cm in diameter, protruding from the mucosal surface (Figure 1). There was moderate atrophy of the renal crests and mild bilateral distention of the ureters and renal pelvis (Figure 1). The prostate was moderately enlarged, and a conspicuous, fluctuant cyst filled with necrotic debris and fibrinosuppurative exudate was present in the right dorsal region (Figure 1). The penis was diffusely reddened and erect, and it extended more than 6 cm from the preputial orifice. From these findings, prostatitis and cystitis were tentatively diagnosed, and tissue samples were fixed and processed for microscopic examination.
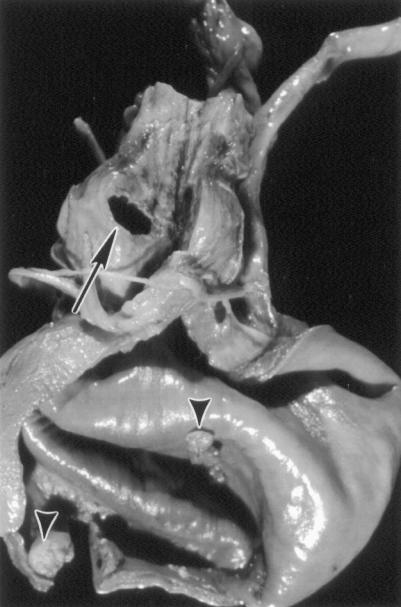
Figure 1. Urinary tract, fixed in Clots preservative. Multiple exophytic nodules on the mucosal surface of the bladder (arrowheads). Enlarged prostate, with a cystic cavitation on the right side (arrow) and mild distention of the right ureter.
Microscopic examination of the bladder revealed that the exophytic masses and the thickening of the vesical wall in the trigone were the results of tumor infiltration and inflammation. Tumor cells extended deep into the submucosa and muscularis, forming nests, cords, or pseudoacini. The neoplastic cells were large, with round to oval nuclei, abundant eosinophilic cytoplasm, and poorly defined cell borders. There were 2 or more mitotic figures per 40X field and marked anisokaryosis. Some vesical blood vessels contained clusters of neoplastic cells, which often occluded the lumen.
The prostate also contained large aggregates of tumoral epithelial cells with morphologic features identical to those described for the bladder. The cavitated lesion in the prostate was composed of tumor cells admixed with polymorphonuclear leukocytes and clusters of gram-positive cocci. Tumor cells were commonly seen in the prostatic vasculature. Coronal sections of the penis revealed clusters of neoplastic cells in the corpus spongiosum and the corpora cavernosa (Figures 2a and 2b).
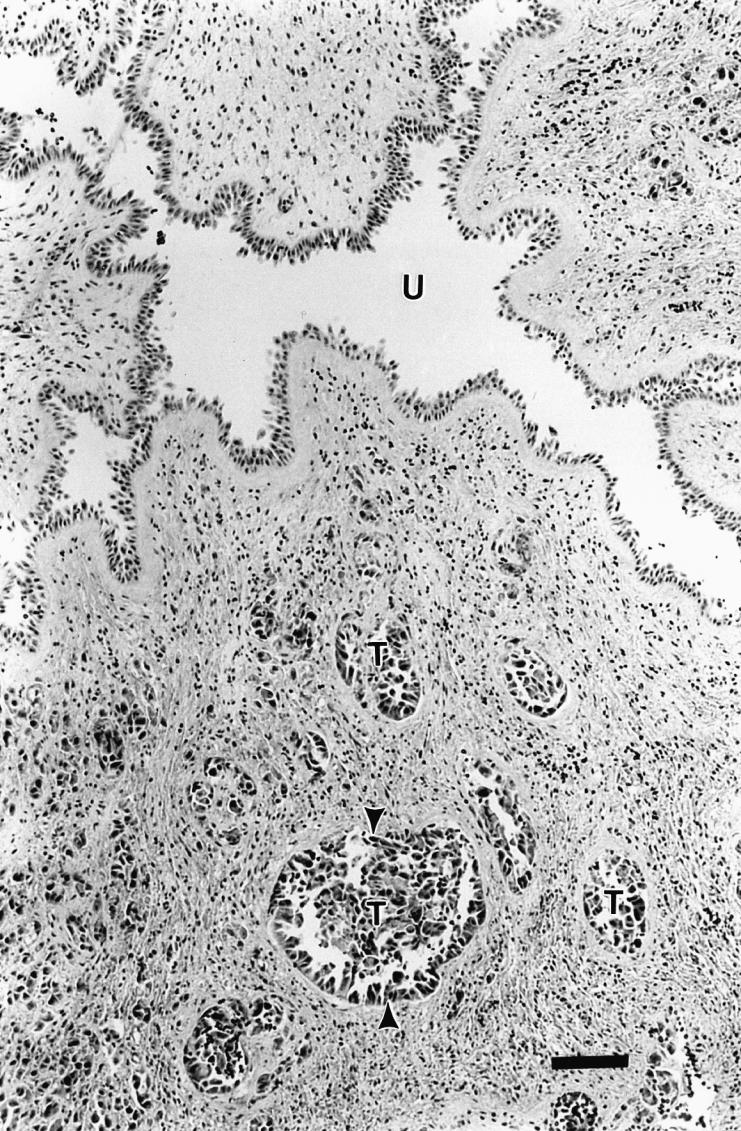
Figure 2a. Cross-section of the penis. Normal urethral lumen (U) and multiple tumoral emboli (T) in the penile vasculature (arrowheads). Hematoxylin and eosin stain; bar = 62.5 μm.
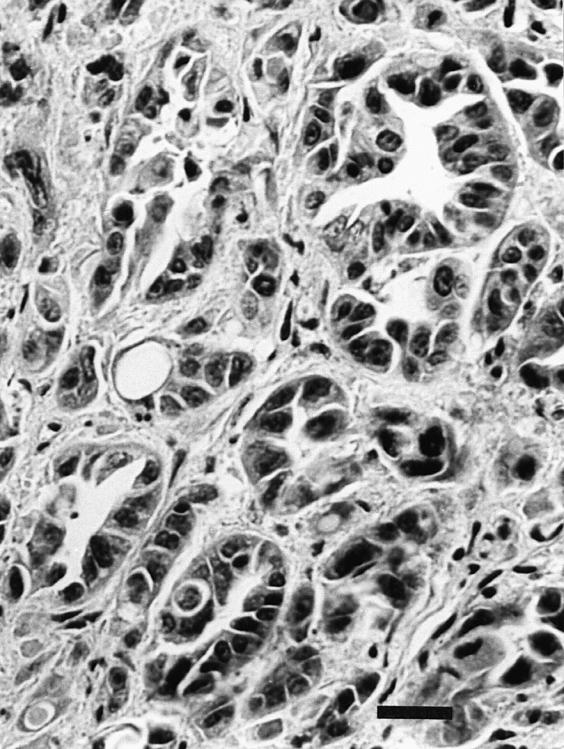
Figure 2b. Close-up of penile corpus cavernosum. Cluster of carcinomatous cells lining the blood vessels. Note the scirrhous reaction in the surrounding stroma. Hematoxylin and eosin stain; bar = 25 μm.
Microscopic examination of the lungs revealed that a medium-sized pulmonary vessel contained a large aggregate of comparable tumor cells. No changes were observed in the spinal cord or brain.
From the histologic findings, the final diagnosis was undifferentiated carcinoma, originating from the urinary bladder or the prostate, with multiple metastases. What made this case unusual was the clinical presentation of priapism and the widespread metastasis to the penile vasculature, which was detected only upon histologic examination.
Priapism, characterized by a persistent and painful penile erection, is rare, being diagnosed only sporadically in humans and domestic animals (1,2). A recent study showed that the incidence in humans is only 1.5 cases per 100 000 person-years (3). The incidence in domestic animals has not been determined (2).
The pathogenesis of priapism is complex, but the condition is generally associated with penile vascular damage or obstruction, excessive release of erectile neurotransmitters, or prolonged smooth muscle relaxation, all of which can contribute to an increase in arterial blood flow or a decrease in venous outflow, causing erection, usually in the absence of sexual stimulation (1). The most common causes in humans are traumatic injury to the pelvic, penile, or perineal region (4), genitourinary cancer (5), the use of psychotropic or anti-impotence drugs (6), and sickle cell disease (3). Idiopathic priapism has also been described (7).
Most of the veterinary medical literature proposes spinal injury and thromboembolic accidents involving the penile vasculature as the most common causes of canine and feline priapism (2). Distemper encephalomyelitis has also been incriminated in dogs (8). Priapism secondary to metastatic tumors has been reported rarely in domestic animals (9). In one case, a stallion that was euthanized because of unresponsive priapism was subsequently found to have generalized malignant melanoma; the priapism was associated with tumoral damage to the dorsal penile nerves and not penile vascular metastasis.
Microscopic examination of the penis was crucial to explaining the priapism in the case reported here. It clearly showed a diffuse and obvious vascular obstruction caused by the carcinomatous metastases in the corpus spongiosum and corpora cavernosa. Similar findings have been well documented in men and children in whom bladder, prostate, or urethral carcinomas had metastasized and obstructed penile blood flow (5). Some investigators use the term “malignant priapism” (10).
In conclusion, unresponsive priapism in dogs, particularly those with no evidence of spinal lesions and especially those with other signs of urinary tract disease, should be carefully investigated for possible metastasis to the penis. Although not used in this dog, cytologic or microscopic examination of biopsy specimens taken from the priapic penis is commonly used to confirm the diagnosis of penile metastasis in humans (5). CVJ
Footnotes
Address correspondence and reprint requests to Dr. Laura Rogers.
References
- 1.Melman A, Serels S. Priapism. Int J Impot Res 2000;12(Suppl 4): S133–S139. [DOI] [PubMed]
- 2.Gunn-Moore DA, Brown PJ, Holt PE, Gruffydd-Jones TJ. Priapism in seven cats. J Small Anim Pract 1995;36:262–266. [DOI] [PubMed]
- 3.Eland IA, van der Lei J, Stricker BH, Sturkenboom MJ. Incidence of priapism in the general population. Urology 2001;57:970–972. [DOI] [PubMed]
- 4.Moscovici J, Barret E, Galinier P, et al. Post-traumatic arterial priapism in the child: a study of four cases. Eur J Pediatr Surg 2000;10:72–76. [DOI] [PubMed]
- 5.Hettiarachchi JA, Johnson GB, Panageas E, Drinis S, Konno S, Das AK. Malignant priapism associated with metastatic urethral carcinoma. Urol Int 2001;66:114–116. [DOI] [PubMed]
- 6.Sur RL, Kane CJ. Sildenafil citrate-associated priapism. Urology 2000;55:950. [DOI] [PubMed]
- 7.Pitetti RD, Nangia A, Bhende MS. Idiopathic priapism. Pediatr Emerg Care 1999;15:404–406. [DOI] [PubMed]
- 8.Guilford WG, Shaw DP, O'Brien DP, Maxwell VD. Fecal incontinence, urinary incontinence, and priapism associated with multifocal distemper encephalomyelitis in a dog. J Am Vet Med Assoc 1990;197:90–92. [PubMed]
- 9.Blanchard TL, Schumacher J, Edwards JF, et al. Priapism in a stallion with generalized malignant melanoma. J Am Vet Med Assoc 1991;198:1043–1044. [PubMed]
- 10.Witters S, Cornelissen M, Vereecken RL. Malignant priapism. Eur Urol 1985;11:431–432. [DOI] [PubMed]