

Abstract
Celiac trunk usually trifurcates and supplies the organs in the supracolic compartment. The vascular variations are common in this region. There are reports on the variant course of right hepatic artery (RHA). The tortuous RHA forming a caterpillar hump is a rare finding and also its providing origin to gastroduodenal artery (GDA) is an important observation. During routine dissection of abdomen of approximately 60-year-old male cadaver, concurrent arterial variations were observed. The celiac trunk bifurcated into splenic and common hepatic arteries. The left gastric artery arose from the abdominal aorta. The common hepatic artery was tortuous and divided into right and left hepatic arteries in front of portal vein. The RHA gave origin to GDA and then made a characteristic loop around the bile duct with the convexity to the right side. Knowledge of arterial variations of celiac trunk and its branches is useful in planning and executing the radiological interventions and surgeries in the supracolic abdominal compartment.
Keywords: Caterpillar hump, Celiac trunk, Common hepatic artery, Gastroduodenal artery, Right hepatic artery, Supracolic abdominal compartment
Introduction
The celiac trunk (CT) is the first ventral branch of abdominal aorta and arises at the level of T12/L1.[1] The main branches of CT include left gastric, common hepatic, and splenic arteries. CT supplies the primary organs of the supracolic abdominal compartment. After arising from CT, the common hepatic artery runs downward and to the right to reach the first part of the duodenum. At this level, it divides into hepatic artery proper and gastroduodenal arteries (GDA). GDA divides into the right gastroepiploic and superior pancreaticoduodenal arteries. Usually, the common hepatic artery gives right gastric branch before its termination. The hepatic artery proper ascends in the right free margin of lesser omentum and divides into right and left hepatic arteries. Cystic artery arises from right hepatic artery (RHA). Presence of collateral branches,[2] complete absence of the trunk,[3] and bifurcation of the trunk[4] are the reported variations of CT. Very few reports pertaining to the unusual course of RHA have been reported in the literature.[5,6] Knowledge of arterial variations of CT and its branches is useful in planning and executing the radiological interventions and surgeries in supracolic abdominal compartment.
The present case is of tremendous importance because the loop of the RHA might get injured during laparoscopic cholecystectomy.
Case Report
During the routine dissection classes for first-year undergraduate medical students, we observed concurrent arterial variations in the supracolic abdominal compartment. These variations were found in a male cadaver of Indian origin, aged approximately 60 years. The CT bifurcated into splenic and common hepatic arteries. The left gastric artery arose from the abdominal aorta, very close to the origin of CT, at the level of twelfth thoracic vertebra. The common hepatic artery was tortuous and it terminated in front of the portal vein by dividing into right and left hepatic arteries [Figures 1 and 2]. The RHA gave origin to GDA in front of the bile duct and then made a characteristic loop around the bile duct with convexity to the right side, and then entered the liver by passing through the porta hepatis behind the bile duct [Figure 2]. This characteristic loop measured around 2 cm in length. The splenic artery passed along the upper border of the pancreas to reach the spleen.
Figure 1.
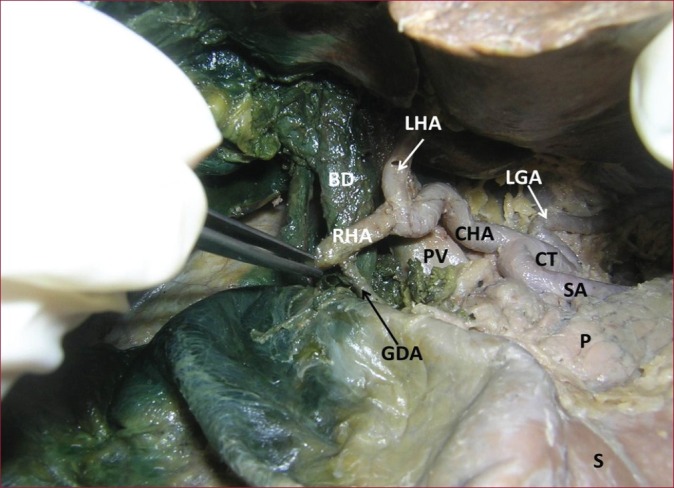
Dissection of the supracolic compartment of the abdominal cavity showing the origin of celiac trunk (CT) in the form of hepatosplenic trunk and origin of left gastric artery (LGA) directly from abdominal aorta, close to the origin of CT. Origin of right hepatic artery (RHA) and left hepatic artery (LHA) is also seen. Note the origin of gastroduodenal artery (GDA) from the right hepatic artery (RHA) in front of bile duct (BD). [Splenic artery (SA), Common hepatic artery (CHA), Portal vein (PV), Stomach (S), Pancreas (P)]
Figure 2.
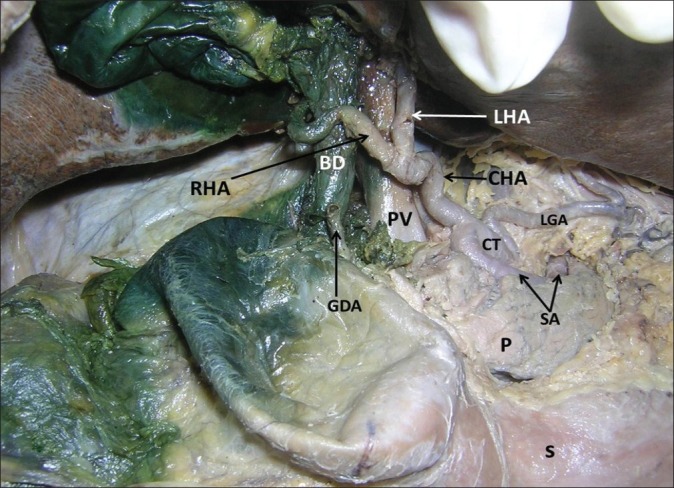
Dissection of the supracolic compartment of the abdominal cavity showing the characteristic loop of right hepatic artery (RHA) around the bile duct with convexity to the right side, before entering into porta hepatis and detached portion of gastroduodenal artery (GDA) from the right hepatic artery (RHA). [Celiac trunk (CT), Splenic artery (SA), Common hepatic artery (CHA), Right hepatic artery (RHA), Left hepatic artery (LHA), Portal vein (PV), Bile duct (BD), Pancreas (P), Stomach (S)]
Discussion
The supracolic abdominal compartment receives its blood supply mainly from the CT. CT frequently shows variations in its branches and distribution. The variations in the CT are due to unusual embryological development of the ventral splanchnic branches of the aorta.[2] Usually, CT branches into the splenic, common hepatic, and left gastric arteries. All the three of its branches might come directly from the abdominal aorta as independent branches. Additional branches of the CT other than its usual branches are commonly referred to as collaterals.[3] Mburu et al. have reported the prevalence of collateral branches from CT, in 20.3% cases.[4] Earlier, the varied origin of collaterals from the CT has been reported.[7] A study conducted on the branching pattern of CT in Kenyan population observed that the CT trifurcated in 61.7% and bifurcated in 17.9% of cases.[4] Different patterns of bifurcation of the CT such as gastrophrenic, hepatosplenic, hepatogastric, and lienogastric trunks have been reported.[4] Mburu et al. and Chitra have reported the incidence of hepatosplenic trunk in 13.1% and 2% cases, respectively.[4,8] In the present case, we observed the hepatosplenic trunk with left gastric artery arising from the abdominal aorta, close to the origin of CT. Computerized tomographic angiography is usually used to reveal the vascular variations of the upper abdomen. A sound knowledge of possible existence of vascular variations, as observed in the present case, is essential for radiologists and surgeons to prevent iatrogenic injuries in this region.
GDA may arise directly from CT. Earlier, a cadaveric study documented the origin of GDA from the CT, in 3.61% of cases.[4] GDA may also arise from the superior mesenteric artery and right or left hepatic artery.[9,10] Nishida et al. have reported a case of GDA steal syndrome during liver transplantation.[11] This syndrome is characterized by low arterial flow towards the graft caused by a shift of flow into GDA. It may cause arterial hepatic hypoperfusion of the graft liver and devastating consequences.[11] Therefore, awareness of possible existence of aberrant origin of GDA is important for recognition and successful ligation of GDA to prevent such consequences. In the procedure of hepatic arterial infusion pumps in hepatic arterial chemotherapy and also for liver and/or colon resection, usually the GDA is cannulated. Hence, the knowledge of varied origin of GDA from the RHA, as in our case, is important for radiologists and surgeons for successful cannulation.
The variations in the course of RHA, in relation to the bile duct, are very rare. Earlier, few reports have showed the presence of the tortuous RHA forming the caterpillar hump which is also called as Moynihan's hump.[5,6] In their study, the loop was formed around the common hepatic duct. In the present case, we report a rare case of tortuous common hepatic artery and the tortuous RHA forming caterpillar hump, winding around the bile duct. The characteristic sinuousness of the RHA is more susceptible to injury following the surgical procedures such as resection of tumor of the pancreatic head and other invasive interventions such celiacography and chemoembolisation of pancreatic and liver tumors and during cholecystectomy.[6,12] Further, GDA arose from this artery close to its loop. While performing hepatic arterial chemotherapy, the aberrant origin of GDA from the looped course of RHA invites injury unless it is carefully recognized and dissected.
Conclusions
Though hepatosplenic trunk is not a rare finding, tortuous course of both the CHA and RHA is not common. Further, the origin of GDA from the RHA close to the looped course has immense importance in the procedure of hepatic arterial chemotherapy.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, Healy JC, et al. 40th ed. Vol. 1198. London: Elsevier, Churchill Livingstone; 2008. Gray's Anatomy: The Anatomical Basis of Clinical Practice; p. 1073. [Google Scholar]
- 2.Cavdar S, Sehirli U, Pekin B. Celiacomesenteric trunk. Clin Anat. 1997;10:231–4. doi: 10.1002/(SICI)1098-2353(1997)10:4<231::AID-CA2>3.0.CO;2-V. [DOI] [PubMed] [Google Scholar]
- 3.Vandamme JP, Bonte J. The branches of the coeliac trunk. Acta Anat (Basel) 1985;122:110–4. doi: 10.1159/000145991. [DOI] [PubMed] [Google Scholar]
- 4.Mburu KS, Alexander OJ, Hassan S, Bernard N. Variations in the branching pattern of the celiac trunk in a Kenyan population. Int J Morphol. 2010;28:199–204. [Google Scholar]
- 5.Johnston EV, Anson BJ. Variations in the formation and vascular relationships of bile ducts. Surg Gynecol Obstet. 1952;94:669–86. [PubMed] [Google Scholar]
- 6.Priti LM, Lakshmi R. Variant right hepatic artery forming Moynihan's hump- clinical relevance. Int J Anat Var (IJAV) 2010;3:144–5. [Google Scholar]
- 7.Rajesh BA, Urvi HD. Uncommon branching pattern of the celiac trunk: Origin of seven branches. Int J Anat Var (IJAV) 2011;4:83–5. [Google Scholar]
- 8.Chitra R. Clinically relevant variations of the coeliac trunk. Singapore Med J. 2010;51:216. [PubMed] [Google Scholar]
- 9.Huu N, Tam NT, Minh NK. Gastro-duodenal artery arising from the superior mesenteric artery. Bull Assoc Anat (Nancy) 1976;60:779–86. [PubMed] [Google Scholar]
- 10.Rawat KS. CT angiography in evaluation of vascular anatomy and prevalence of vascular variants in upper abdomen in cancer patients. Indian J Radiol Imaging. 2005;16:457–61. [Google Scholar]
- 11.Nishida S, Kadono J, DeFaria W, Levi DM, Moon JI, Tzakis AG, et al. Gastroduodenal artery steal syndrome during liver transplantation: Intraoperative diagnosis with Doppler ultrasound and management. Transpl Int. 2005;18:350–3. doi: 10.1111/j.1432-2277.2004.00065.x. [DOI] [PubMed] [Google Scholar]
- 12.Nahrwold DL. The Biliary System. In: Sabiston DC, editor. Textbook of Surgery. The Biological Basis of Modern Surgical Practice. 15th ed. Philadelphia: WB Saunders and Company; 1997. pp. 1117–25. [Google Scholar]