

Abstract
Background:
Cardiovascular diseases are becoming the major cause of morbidity and mortality in most of the developing countries including India. Various behavioral risk factors are the major risk factors for coronary artery disease. Present study was carried out to study the role of various behavioral risk factors in the occurrence of coronary artery disease.
Materials and Methods:
Present study was a hospital-based paired-matched case-control study, carried out at civil hospital, Ahmedabad. A total of 135 newly-diagnosed cases of coronary artery disease and 135 controls were studied after taking an informed written consent. Data was analyzed by using Epi-info version 3.5.1 computer package, Chi -square test, Z test and Odds ratio was calculated.
Results:
Among the total 135 cases, 70.4% were male and 29.6% were female, most of the cases (40%) belong to the age group of 51-60 years. Smokers, smokeless tobacco users, and alcoholic were significantly higher among the cases as compared to controls. Significant association was also observed between current smokers, smokeless tobacco users, and coronary artery disease. Dose-response relationship was observed between the frequency of smoking per day and coronary artery disease (OR = 3.72). Significant association was also observed between obesity, physical inactivity, and coronary artery disease. Salt and oil intake per day were significantly higher among the cases as compared to controls.
Conclusion:
Modifiable and preventable behavioral risk factors are major etiology behind the occurrence of coronary artery disease, which highlights the need of appropriate control strategies and measures.
Keywords: Behavioral risk factors, case- control study, coronary artery disease
INTRODUCTION
Studies show that at the beginning of the 20th century, coronary heart disease (CHD) accounted for less than 10% of all deaths worldwide. At the beginning of the 21st century, CHD accounts for nearly 50% of all deaths in the developed world and 25% in developing countries, such as India.[1] Overall prevalence has increased from 2.06% in 1970 to 5% in 2002 in rural area and 1.04% in early 1960 to 13.02% in 2004 in urban area.[2]
Coronary artery disease (CAD) has been defined as “impairment of heart function due to inadequate blood flow to the heart compared to its needs, caused by obstructive changes in the coronary circulation to the heart.” CAD manifests itself in many presentations like: Angina pectoris of effort, myocardial infarction, irregularities of the heart, cardiac failure, and sudden death.[3]
Coronary artery disease is a multifactorial disease. Various behavioral risk factors like smoking, smokeless tobacco consumption, physical inactivity, unhealthy diet, and alcohol consumption are known to be the important risk factors for CAD. Most of the behavioral risk factors are potentially modifiable ones.[4] We can significantly decrease the premature morbidity and mortality due to coronary artery disease by controlling these modifiable behavioral risk factors. Taking into consideration of these facts, the present case-control study was carried out at civil hospital Ahmedabad to study the role of various behavioral risk factors in the occurrence of coronary artery disease.
MATERIALS AND METHODS
The present study was paired-matched case-control study, carried out at civil hospital Ahmedabad, a tertiary care teaching hospital, for 1 year from March 2009 to April 2010. Permission was taken from the ethical committee, of the institute before carrying out the study. An informed written consent was taken from all the enrolled subjects after a full explanation of the purpose of study and liberty to drop out. This was done in Gujarati, Hindi, and English languages for an easy comprehension. All the patients were interviewed and examined while in hospital, all the information was filled up in a specially-designed pretested questioner.
Sample size
The sample size of the study was calculated after conducting the pilot study by using the following formula.[5]
Where,
α = 0.05 (allowed type I error)
β = 0.02 (allowed type II error)
So for these values of type I and type II errors, the values of power of detecting these errors are as under;
Z1-α/2 = 1.96 and
Z1-β = 0.84
P 1 = 0.55 proportion of smokers among the cases in pilot study
P 2 = 0.38 proportion of smokers among the controls in pilot study
p = (P 1 + P 2)/2 = 0.465
q = 1- p = 0.535
r = ratio of number of controls to cases, here it was 1.
Putting all these values to the above-mentioned equation, the desired sample size was found to be 134.97 ≅135. As the case: control ratio was kept 1: 1, the final total sample size of study was 270 (135 cases and 135 controls).
Selection of cases
Definition of case
Present study includes newly-diagnosed cases of CAD. CAD patients were diagnosed as per the Monica criteria: (1) 2 or more ECG showing specific changes; (2) an ECG showing probable changes plus abnormal cardiac injury enzymes; or (3) typical symptoms such as a retrosternal pain plus abnormal enzymes.[6]
Eligibility criteria for cases
The patient who was diagnosed first time as a suffering from CAD to avoid bias arising from recall memory.
Well conscious, co-operative, and well-oriented with time, place and person, to avoid bias from respondent's answers.
Selection of control
Definition of control
A control was defined as an individual who was admitted in civil hospital Ahmedabad on the same day or within 7 days for conditions other than angina pectoris and myocardial infarction. For the selection of proper control, person's prior history regarding CAD was asked and it was assured that the control had never been admitted to hospital or taken treatment for acute myocardial infarction and angina pectoris.
Eligibility criteria for control
Well-conscious, co-operative, and well-oriented with time, place, and person, who voluntary agree to participate in the study to avoid bias from respondent's answers.
Matching
For each case, 1 age- and sex-matched control was selected; age matching was done with the liability of ± 2 years of age.
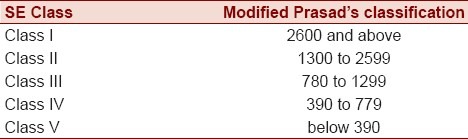
Socio-economic classes were define according to modified Prasad's classification with Consumer Price Index of mid study period (530).[7] Accordingly, the following classification was used [Table 1].
Table 1.
Socio-economic classification
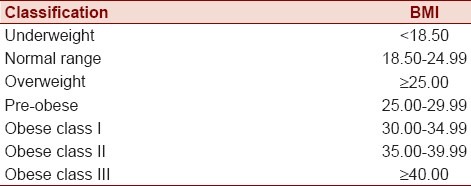
Body mass index (BMI) was used to classify the weight status of subjects. It was derived by dividing the weight in kilograms by the square of the height in meters (kg/ m2). Classification of overweight and obesity was done according to WHO classification [Table 2].[8]
Table 2.
Classification of adults according to BMI
Time spend for moderate physical activity like brisk walking, cycling was calculated for each subject, and accordingly, they were classified as a physically inactive if physical activity was <30 minutes/day.[9]
Association of the risk factors under study was assessed by applying Chi-Square test and Z test. To assess the strength of association, the odds ratio was calculated. For all these statistical analysis, Epi- info version 3.5.1 computer package was used.
RESULTS
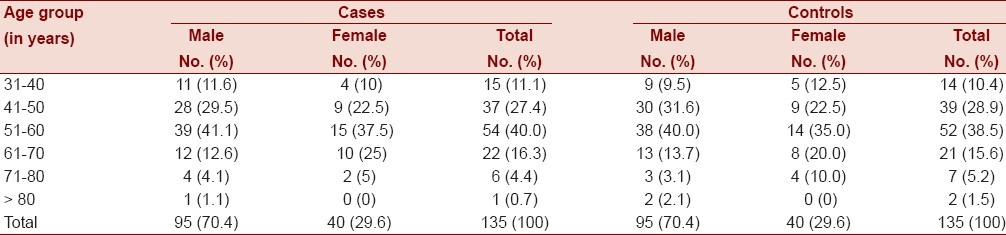
A total of 135 cases of coronary artery disease and 135 matched controls were analyzed. Among the cases, 70.4% were males and 29.6% were females.
The Largest numbers of cases were in the age group of 51-60 years (40%). The mean age of cases and controls were 54 ± 10.50 years and 53.83 ± 10.66 years, respectively, and this difference was not statistically significant (Z = 0.13, P > 0.05) [Table 3].
Table 3.
Age and sex-wise distribution of cases and controls
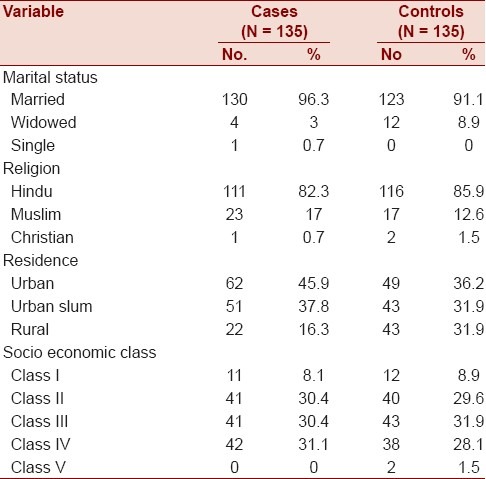
Study of socio-demographic characteristics revealed that predominance of Hindus in both cases and controls. Family characteristics did not reveal any significant difference between cases and controls. Majority of the cases 45.9% were from urban area while controls were equally distributed in urban, urban slum, and rural area, and this difference was statistically significant (χ2 = 8.99, P < 0.01).
Distribution as per social class stated that middle socio-economic class was predominant (91.9%) among the cases while only 8.1% of cases were from socio-economic class I, and similar distribution was also observed among the controls. This is because most of the patients come to the civil hospital, Ahmedabad were belongs to the lower or middle socio-economic class. Overall literacy rate of cases and controls was 75.5% and 66.7%, respectively [Table 4].
Table 4.
Socio demographic characteristic of cases and controls
Majority of men in cases (48.41%) were engaged in either some sort of service or business while majority of men in controls (51.6%) were working as a laborer or farmer. Most of females in both cases and controls (80% and 62.5%, respectively) were engaged in household work.
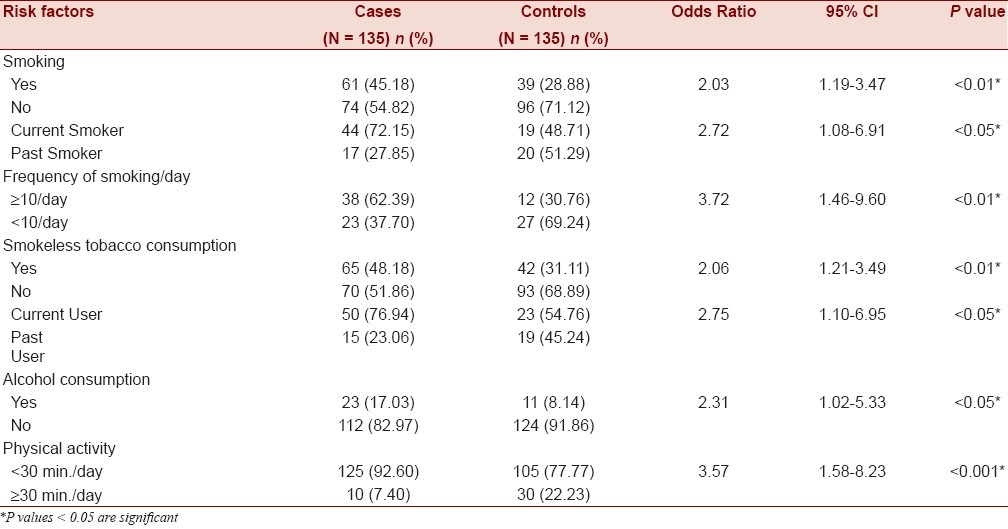
Smokers, smokeless tobacco consumers, and alcoholic were more among the cases (45.18%, 48.14%, and 17.03%) as compared to controls (28.88%, 31.11%, and 8.14%), and these differences were also statistically significant.
Most of the smokers (98.36% and 97.43%) and smokeless tobacco consumers (84.61% and 83.33%) were males in both cases and controls. Alcohol consumption was observed among the males only in both cases and controls.
It was seen that current smokers and smokeless tobacco consumers were significantly higher among the cases (72.15% and 76.94%, respectively) as compared to controls (48.71% and 54.76%, respectively). Among most of the smokers (93.44% and 87.19% from cases and controls, respectively), the most common method of smoking was through bidi. There were higher proportions of heavy smokers (³10 bidis or cigarettes/day) among the cases (62.30%) as compared to controls (30.76%), and this difference was statistically significant. Significant association was observed between physical inactivity and CAD (OR = 3.57) [Table 5].
Table 5.
Distributions of study subjects according to their addiction and physical activity
While doing sex-wise analysis, strong association was observed between physical inactivity and CAD among males (OR = 3.38) while no significant association was observed between physical inactivity and CAD among females [Table 6].
Table 6.
Sex-wise distribution of cases and controls according to their physical activity

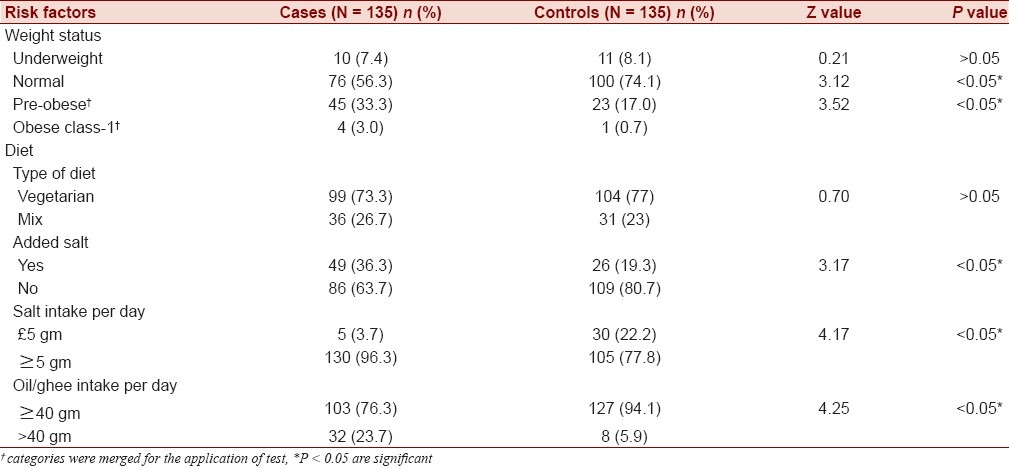
In present study, the mean BMI of cases (23.73 ± 3.41) was significantly higher than of the controls (22.38 ± 2.60) (Z = 3.66, P < 0.05).
Among the total 135 cases, 36.3% of the cases were either pre obese or obese class 1 as compared to 17.7% of the controls, and this difference was statistically significant. Most of the cases (73.3%) and controls (77%) were vegetarian. Salt and oil/ghee intake per day as well as intake of extra salt in the diet were significantly higher among the cases as compared to controls [Table 7].
Table 7.
Distribution of study subjects according to their weight status and dietary pattern
DISCUSSION
The present study was designed as hospital-based case-control study to assess the role of various behavioral risk factors in the occurrence of coronary artery disease. A total of 270 subjects (135 cases and 135 controls) were studied. Among the total 135 cases, 70.4% were males and 29.6% were females, male predominance has been also reported by Zodpay et al.[10] Singh RB et al. also observed that prevalence of CAD was significantly (P < 0.001) higher in men as compared to women in both urban (11% Vs. 6.9%) and rural (3.9% Vs. 2.6%), areas respectively.[11]
The mean age of cases was 54 ± 10.50 years, largest number of cases were present in the age group of 51-60 years (40%), followed by 41-50 years (27.4%), whereas 11.1% of the cases had faced their first attack of CAD before crossing the 40 of their life, which is well-correlated with the findings of Zodpay et al.[10] Significantly higher numbers of cases were belongs to urban area as compared to rural area, similar urban rural difference was also observed by Singh R. B. et al.[11] The high prevalence of CAD among urban dwellers might be due to accumulation of various risk factors.
There is incontrovertible evidence that tobacco, in any form (smoked or chewed), is a major risk factor of CAD.[12] In present study, significant associations were observed between smoking, current smoking and coronary artery disease (OR=2.03 and 2.72 respectively), and a dose-response relationship was also observed between the frequency of smoking per day and CAD (OR = 3.72), which are well-correlated with the observations of Prem Pais et al.[13] in their study.
In our study significant association was observed between smokeless tobacco consumption and coronary artery disease (OR=2.06) which is well correlated with the findings of Rahman MA et al.[14] Significant association was also observed between alcohol drinking and CAD, which is similar with the findings of Subrata Bagchi et al[15] In present study, unhealthy behavior like smoking, smokeless tobacco consumption, and alcohol consumption were more among the males as compared to females in both cases and controls, similar findings were also observed by Waldron I[16] in their study. Possible reason may be that these types of unhealthy behaviors are more socially acceptable for males than for females.
In present study, 92.6% of the cases were physically inactive (<30 min/day), this was significantly higher than controls (83.7%), and this finding is also correlated with the finding of study conducted by Thompson PD et al.[17]
While doing sex-wise analysis, strong association was observed between physical inactivity and CAD among males (OR = 3.38), no significant association was observed between physical inactivity and CAD among females. There is general agreement that physical inactivity is associated with an increased risk of heart disease in men. In contrast, studies of women have produced mixed results. Blair et al.[18] also found increasing level of exercise to be associated with a decrease the risk of heart disease in men but not in women. Possible explanations for this difference are most women's physical activity is too low to show a benefit, women's were incorrectly classified as a sedentary because even sedentary group does housework.
Obesity has been identified as a risk factor for CAD in study conducted by Zodpay et al.[10]; in present study, significant association was also observed between obesity and CAD. WHO stated that salt is an independent risk factor for hypertension, and an intake of salt should be up to or less than 5 gm/day to prevent CAD.[3] In current study, consumption of salt more than 5 gm/day was found to be more among the cases as compared to controls. WHO stated that high fat intake (dietary fat representing 40% or over of the energy supply and containing a higher proportion of saturated fats) is a major risk factor for CAD.[3] In present study, significantly higher numbers of the cases (23.7%) were consumed more than 40 g. oil/ghee per day than the controls (5.9%).
Present study was conducted at civil hospital, Ahmedabad, and most of patients admitted in civil hospital belong to middle or lower socio-economic class; therefore, in present study, significant association was not observed between socio-economic class and CAD.
To conclude, findings of our study suggest that modifiable and preventable various behavioral risk factors are important etiology behind the occurrence of CAD. Public health remedial measures, therefore, be urgently needed to minimize the significant proportion of premature morbidity and mortality due to CAD.
ACKNOWLEDGMENT
The authors acknowledge all the staff of Medicine department, Civil hospital, Ahmedabad for their valuable guideline in this study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.World Health Report: Reducing risks, promoting healthy life. Geneva: World Health Organization; 2002. World Health Organization. [Google Scholar]
- 2.Gupta R. Burden of coronary heart disease in India. Indian Heart J. 2004;57:632–8. [PubMed] [Google Scholar]
- 3.Report of a WHO Expert Committee. Vol. 678. Geneva: WHO; 1982. Prevention of coronary heart disease; p. 8. Tech. Rep. Ser. [Google Scholar]
- 4.Park K. Textbook of, preventive and social medicine. 20th ed. 06. Jabalpur, India: Bhanot; 2009. pp. 318–58. [Google Scholar]
- 5.Kleinbaum DG, Sullivan KM, Barker ND. Active Epi companion textbook: A supplement for use with active Epi CD-ROM [Google Scholar]
- 6.Tunstall-Pedoe H, Kuulasmaa K, Amouyel P, Arveiler D, Rajakangas AM, Pajak A. Myocardial infarction and coronary deaths in the World Health Organization MONICA Project. Registration procedures, event rates, and case-fatality rates in 38populations from 21countries in four continents. Circulation. 1994;90:583–612. doi: 10.1161/01.cir.90.1.583. [DOI] [PubMed] [Google Scholar]
- 7.Kumar P. Social classification need for constant updating. Indian J Commun Med. 1993;18:60–1. [Google Scholar]
- 8.Report of a WHO consultation. Vol. 894. Geneva: World Health Organ; 2000. Obesity: Preventing and managing the global epidemic; pp. 8–9. Tech Rep Ser, [Information: same as in the reference no.3] [PubMed] [Google Scholar]
- 9.Battly GD, Lee IM. Physical activity and coronary heart disease. BMJ. 2004;328:1089–90. doi: 10.1136/bmj.328.7448.1089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zodpey SP, Kulkarni HR, Vasudeo ND, Kulkarni SW. Risk factors for coronary heart disease: A case control study. Indian J Commun Med. 1998;23:7–14. [Google Scholar]
- 11.Singh RB, Sharma JP, Rastogi V, Raghuvanshi RS, Moshiri M, Verma SP, et al. Prevalence of coronary artery disease and coronary risk factors in rural and urban population of north India. Eur Heart J. 1997;18:1728–35. doi: 10.1093/oxfordjournals.eurheartj.a015167. [DOI] [PubMed] [Google Scholar]
- 12.Fichenberg CM, Glantz SA. Association of California Tobacco Control Progarm with declines in cigarette consumption and mortality from heart disease. N Engl J Med. 2000;343:1772–7. doi: 10.1056/NEJM200012143432406. [DOI] [PubMed] [Google Scholar]
- 13.Pais P, Pogue J, Gerstein H, Zachariah E, Savitha D, Jayprakash S, et al. Risk factors for acute myocardial infarction in Indians: A case-control study. Lancet. 1996;348:358–63. doi: 10.1016/s0140-6736(96)02507-x. [DOI] [PubMed] [Google Scholar]
- 14.Rahman MA, Zaman MM. Smoking and smokeless tobacco consumption: Possibale risk factors for coronary heart disease among young patients attending a tertiary care cardiac hospital in Bangladesh. Public Health. 2008;122:1331–8. doi: 10.1016/j.puhe.2008.05.015. [DOI] [PubMed] [Google Scholar]
- 15.Subrata Bagchi, Ranadeb Biswas, Bhadra UK, Aniruddha Roy, Malay Mundle, Dutta PK. Smoking, alcohol consumption and coronary heart disease- A Risk factor study. Indian J Commun Med. 2001;26:208–11. [Google Scholar]
- 16.Waldron I. Why do women live longer than men? Soc Sci Med. 1976;10:349–62. doi: 10.1016/0037-7856(76)90090-1. [DOI] [PubMed] [Google Scholar]
- 17.Thompson PD, Buchner D, Pinal I, Balady GJ, Williams MA, Marcus BH, et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease. Circulation. 2003;107:3109–16. doi: 10.1161/01.CIR.0000075572.40158.77. [DOI] [PubMed] [Google Scholar]
- 18.Blair SN, Kohl HW, III, Paffenbarger RS, Jr, Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality: A prospective study of healthy men and women. JAMA. 1989;262:2395–401. doi: 10.1001/jama.262.17.2395. [DOI] [PubMed] [Google Scholar]