

Abstract
Esophageal squamous cell carcinoma (ESCC) is more sensitive to radiation and chemotherapy than other cancers of the digestive system, and combined modality therapy may represent a promising treatment method. The radiation-sensitizing effect of docetaxel on ESCC cell lines was investigated. A colony formation assay was performed in which ESCC cell lines (TE2, TE3) and A431 were exposed to docetaxel (from 1.0×10−11 to 10−7 M) for 3 h to determine the concentration of docetaxel that was not able to kill individual cells (i.e., the non-cytocidal concentration). Individual cell lines were then exposed to the non-cytocidal concentration of docetaxel prior to, during, and after irradiation to determine whether the timing of docetaxel administration affected cell survival. In addition, flow-cytometry was performed, and the cell cycle was examined prior to and after docetaxel exposure to assess the mechanism of docetaxel as a radiation sensitizer. Docetaxel exhibited a concentration-dependent cytocidal effect, with a different IC50 for each cell type. Almost no cytocidal effect was observed at the following docetaxel concentrations: A431, ≤1.0×10−10 M; TE-2 and TE-3, ≤1.0×10−9 M. Concurrent treatment with docetaxel and radiation tended to decrease cell survival in all the cell lines compared with docetaxel or radiation alone. Cell survival was lowest when the cells were treated using X-ray irradiation after docetaxel exposure (p<0.05). Flow cytometry revealed that in all three cell lines, docetaxel exposure increased the G2/M cell fraction with a higher increase in the cell line that exhibited the highest radiosensitivity. This study demonstrated that the administration of docetaxel at a non-cytocidal concentration prior to radiotherapy produced a synergistic cell-killing effect in SCC cell lines.
Keywords: docetaxel, radiation-sensitizing effect, esophageal squamous cell carcinoma
Introduction
The surgical outcome of patients with esophageal squamous cell carcinoma (ESCC) has improved as a result of a progress in diagnostic methods, surgical procedures, and perioperative management. However, recent studies have emphasized the utility of chemoradiotherapy (CRTx) for patients with ESCC (1,2), since it enables a favorable therapeutic outcome comparable to that of radical surgery while avoiding surgical stress and maintaining a good quality of life (QOL) (3,4). The regimen of standard CRTx usually consists of the concurrent use of cisplatin/fluorouracil (CDDP/5FU) with radiation (5).
However, other anticancer agents for concurrent use with radiation therapy have not been examined thoroughly with regard not only to their cytocidal effects, but also their mechanisms of action.
Among the many agents assessed for therapeutic efficacy against ESCC, docetaxel has been introduced during the last decade. The anti-tumor mechanism of docetaxel is completely different from that of 5FU and CDDP (6). Docetaxel promotes the polymerization of tubulin and inhibits the disassembly of microtubules, thereby blocking cell division at the M phase during the cell cycle. In vitro colony formation assays have demonstrated the superior anti-tumor activity of docetaxel against many cell lines including ESCC (7,8). A phase II clinical trial of docetaxel monotherapy for the treatment of advanced/recurrent ESCC reported a response rate of 20.4%. These findings indicate that docetaxel may be a useful chemotherapeutic agent for the treatment of ESCC (9–12).
Concerning CRTx, previous studies have reported that the combined use of docetaxel with radiation therapy yielded excellent tumor-inhibition in patients with ESCC (13–15). It was also also reported that CRTx including docetaxel produced a response rate of 96% and a complete response rate of 50% in patients with head and neck cancer (16). These findings demonstrated that the combined use of docetaxel and radiation improved the tumor response, compared with docetaxel or radiation alone (17,18). Recent studies demonstrated the cell-killing effects of radiation and docetaxel on squamous cell carcinoma (SCC) cell lines in vitro, and also demonstrated the same effect on SCC cells in vivo (19–24). Although these studies described a significant anti-tumor effect under the concurrent use of docetaxel with radiation, the docetaxel solution that was used in the experiment was itself sufficient to kill the SCC cells, and the synergistic aspects of docetaxel used in combination with radiation were not reported (19–22). We performed CRTx using a very low concentration of etoposide that is not capable of killing the cancer cells by itself (i.e., a non-cytocidal concentration), and demonstrated a marked anti-tumor effect in SCC cells (25). This observation indicates a synergistic effect of anticancer agents used concurrently with radiation.
In the present study, a colony formation assay and flow cytometry were conducted to demonstrate the radiation-sensitizing effect of docetaxel at a concentration that did not exhibit cytotoxity in the SCC cell lines. Our hypothesis proposed that a low concentration of docetaxel acts as a radiation sensitizer, in the same manner as etoposide.
Materials and methods
SCC cells
Two ESCC cell lines (TE-2 and TE-3) were kindly provided by Dr T. Nishihira (Tohoku University, Sendai, Japan); vulvar carcinoma cells (A431) were also used in this study. Although A431 is a vulvar carcinoma cell line, it is a well-known SCC cell line and is easy to culture and handle. It was therefore used as the control in the experiment. All cells were grown in Dulbecco's modified Eagle's medium (DMEM) supplemented with 10% fetal calf serum and maintained in a humidified atmosphere of air containing 5% carbon dioxide at 37°C.
Colony formation assay
The colony formation assay was used to calculate the cell survival fraction. All cells were obtained at an exponential growth phase 2 days after seeding and incubation in flasks with a surface area of 25 cm2 and a cell concentration of 1×106 cells per flask. The cells used in the study had more than 70% of the plating efficiency. Prior to the experiment, the plating efficiency of A431, TE-1, TE-2, TE-3, TE-5, TE-8 and TE-10 was assessed. A431, TE-2, and TE-3 were selected for the study since these cell lines had a high plating efficiency. After individual experiments, the cells were rinsed twice in phosphate-buffered saline (PBS), trypsinized (0.05%), and seeded into culture dishes (US-11900, Sumitomo, Japan). After having been incubated for 1–3 weeks, the cells were stained with crystal violet and the colonies (>50 cells) were counted.
Docetaxel exposure
Docetaxel (Taxotere®, RP56976; Sanofi-Aventis, Tokyo, Japan) (6) was dissolved in serum-free DMEM medium, and a 10 mg/ml stock solution was prepared; this solution was diluted to the final concentration with DMEM medium at the time of use. The cells were then incubated with the docetaxel solution for 3 h to determine the effect of docetaxel. The diluted solutions were prepared immediately prior to the start of each experiment. Solutions that had been prepared 1 hour or more prior to the experiment were discarded. To plot the cell survival curves, the colonies were divided by the initial number of cells. Each experiment consisted of quintuplicate disks to minimize deviations in cell plating, and were repeated at least three times to confirm the results. The concentrations of docetaxel that did not kill individual cells (i.e., the non-cytocidal concentrations) were determined from the cell survival curves.
X-ray irradiation
X-ray irradiation was performed with an MBR-1520R X-ray machine (Hitachi, Tokyo, Japan) set at 150 kVp, and 20 mA, using 1.5-mm aluminum filtration with a dose rate of 1 Gy/min. Individual cells were irradiated with 2, 4, 6, or 8 Gy X-rays at room temperature. Cell survival curves were plotted as described in the docetaxel experiment.
Combination of docetaxel and radiation
Next, a combined assessment of docetaxel and X-ray radiation was performed. First, individual cell lines were exposed to non-cytocidal concentrations of docetaxel, as determined in the docetaxel exposure experiment, at time points prior to, during, or after irradiation with 2, 4, 6, or 8 Gy X-rays, to determine whether the timing of docetaxel administration would affect cell survival. A colony formation assay was performed using the method described above. The survival fraction (SF) was corrected by the plating efficiency obtained from the cell survival rate in the absence of radiation. Individual experiments were repeated at least two times, and were comprised of quintuplicate cultures.
Any changes in the shoulder and slope (D0) of the survival curves for docetaxel plus radiation and radiation alone were analyzed to evaluate the effect of docetaxel itself in individual cells. The cytocidal effects were determined to compare the survival rate between cells treated with docetaxel plus radiation and those treated with radiation alone for each radiation dose.
Determination of cell cycle
To analyze the action mechanism of docetaxel as a radiation sensitizer, flow cytometry was performed to assess the cell cycle prior to and after docetaxel exposure. A431, TE2, and TE3 cells were exposed to 10-10 M docetaxel for 3 h. To prepare isolated cell suspensions, the cells were trypsinized and then rinsed twice in PBS. The isolated cells were suspended in 1 ml of PI solution containing 50 μg/ml propidium iodide (Sigma-Aldrich, St. Louis, MO, USA), 0.25 mg/ml RNAse, 0.1% sodium citrate, and 0.2% Nonidet P-40, then stained at 4°C for 30 min. The cells were then passed through a 35-μm nylon mesh filter, and the nuclear DNA content was determined using an F1000 flow cytometer. The fluorescence of >10,000 nuclei was measured using an EPICS profile flow cytometer (Beckman Coulter, Fullerton, CA), and DNA histograms were obtained. The DNA histograms were analyzed using Cell FIT™ 2.0 (Becton Dickinson, Franklin Lakes, NJ, USA). The nuclear DNA content of each cell was measured prior to and after treatment with low concentrations of docetaxel, and the distribution of cells was calculated in different phases of the cell cycle (26–28).
Statistical analysis
A statistical analysis of the data was carried out using a one-factor ANOVA (Stat View 5.0). A two-sided p<0.05 was considered statistically significant.
Results
Docetaxel sensitivity
The cytocidal effect of docetaxel alone on cultured cells was evaluated. The cell survival curves following 3 h of treatment with docetaxel at concentrations ranging from 1.0×10−11 to 1.0×10−7 M are represented in Fig. 1. These cell survival curves clearly revealed a concentration-dependent cytocidal effect of docetaxel, with a different IC50 for each cell type. The IC50 for docetaxel treatment was 3.2×10−10 M for A431, 9.1×10−10 M for TE-3, and 1.3×10−9 M for TE-2; thus, the sensitivity to docetaxel among these cell lines increased according to this order. Moreover, almost no cytocidal effect was observed at specific concentrations. A431 cell viability decreased at docetaxel concentrations ≥1.0×10−9 M, whereas exposure to docetaxel concentrations ≤1.0×10−10 M produced very slight cytocidal effects. The viability of TE-2 and TE-3 cells decreased at docetaxel concentrations ≥1.0×10−8 M, whereas docetaxel concentrations ≤1.0×10−9 M had minimal effects. Based on these results, the maximum docetaxel concentrations yielding no cytocidal effects were arbitrarily designated as 1.0×10−11 M for A431, and 1.0×10−10 M for TE-2 and TE-3.
Figure 1.
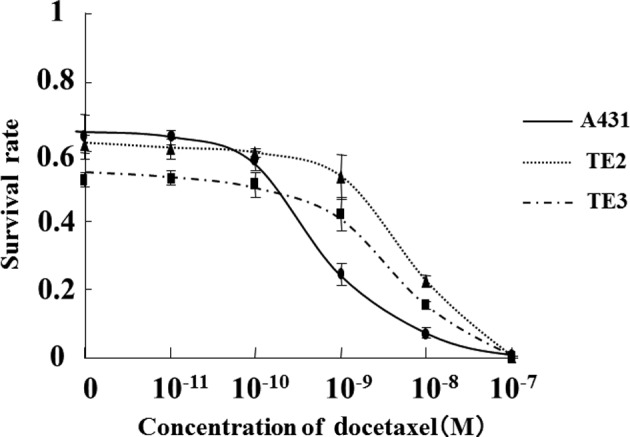
Cell survival curves following 3 hours of treatment with docetaxel at concentrations ranging from 1.0×10−11 to 1.0×10−7 M. The non-cytocidal concentration (M) was determined based on the survival curves: A431 cells, ≤1.0×10−11; TE2 cells, ≤1.0×10−10; TE3 cells, ≤1.0×10−10.
Radiosensitivity
The survival curves obtained after the X-ray irradiation of individual cell lines are shown in Fig. 2. The cell survival curves demonstrated that cell viability decreased in a radiation dose-dependent manner in each cell line and that the sensitivity to X-ray radiation differed among the cell lines. The TE-2 cell line had the highest radiosensitivity to irradiation (D0 value = 0.97 Gy), followed by TE-3 (D0 value = 1.1 Gy) and A431 (D0 value = 2.2 Gy). Notably, A431 exhibited a markedly high sensitivity to docetaxel, whereas TE-2 exhibited the lowest sensitivity. These findings indicate that the radiosensitivity of these cells was inversely correlated with the sensitivity to docetaxel.
Figure 2.
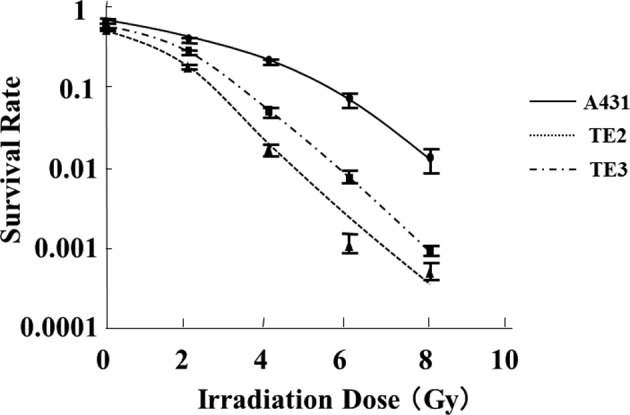
Survival curves obtained after X-ray irradiation of individual cells. The D0 (Gy) values were determined from the survival curves: TE-2, 0.97; TE-3, 1.1; A431, 2.2.
Combined effect of docetaxel and radiation
We then investigated whether docetaxel had a radiation-sensitizing effect on SCC cells. Almost no decrease in cell viability was observed after 3 h of treatment with docetaxel alone at a concentration of 1.0×10−11 M or lower in the A431 cells, and at a concentration of 1.0×10−10 M or lower in the TE-2 or TE-3 cells. Based on the above results, the changes in the cell survival curves following X-ray irradiation with docetaxel exposure at these non-cytocidal concentrations were analyzed (Fig. 3). We also analyzed whether the treatment timing of docetaxel (prior to, during, or after radiation) was correlated with cell survival.
Figure 3.

Cell survival curves obtained after concurrent X-ray irradiation and docetaxel exposure. Individual cell lines [(A) A431, (B) TE2, and (C) TE3] were exposed to docetaxel prior to, during, and after radiation. *Comparison between docetaxel exposure prior to radiation and radiation alone; p<0.01. **Comparison between docetaxel exposure at the same time as radiation and radiation alone; p<0.01.
Among the three different timings of docetaxel administration, cell survival was lowest when the cells were treated using X-ray radiation immediately after 3 h of exposure to docetaxel at a non-cytocidal concentration. Significant decreases in cell viability were observed compared with radiation alone (≥2 Gy in A431 and TE-2, and ≥4 Gy in TE-3). When the cells were treated with radiation (≥6 Gy in A431, ≥4 Gy in TE-2, and ≥8 Gy in TE-3) during docetaxel exposure, significant decreases in cell survival were also observed in all the cell lines. The cytocidal effects were lower than those obtained by irradiation immediately after docetaxel exposure, and the extent of the radiation-sensitizing effect was highest in TE-2 cells. On the other hand, no decreases in cell viability were observed in any of the cell lines treated with docetaxel immediately after X-ray irradiation at any radiation dose.
The correlation between the IC50 of docetaxel and the radiation-sensitizing effect was then assessed. The cells were treated with 8 Gy of radiation immediately after exposure to a non-cytocidal concentration of docetaxel, and the cell survival rates were compared. The cell viability of the concurrent use of radiation and docetaxel was 20.3% in A431, 69.2% in TE-2, and 21.7% in TE-3, compared with radiation alone, indicating that cell lines with a lower IC50 had a lower cell survival rate after concurrent treatment.
Determination of the cell cycle distribution in each cell line
The cell cycle profiles prior to and after 3 hours of treatment with docetaxel at a non-cytocidal concentration of 1.0×10−10 M were determined using flow cytometry (Fig. 4). The cell fraction in the G2/M stage had clearly increased by approximately 2 times in the A431 cells and 5 times in the TE-2 cells (Table I). Although the cell fraction in the G2/M stage had also increased in the TE-3 cells, the increase was not as obvious.
Figure 4.

Representation of flow cytometry (TE2) (A) prior to and (B) after 3 h of exposure to 10−10 M docetaxel. The cell fraction in the G2/M stage increased after docetaxel exposure (arrow).
Table I.
Changes in the cell cycle following exposure to 1×10−10 M of docetaxel, as determined using flow cytometry.
| Cell cycle (%)
|
||||
|---|---|---|---|---|
| Cell line | G0/G1 | S | G2/M | |
| A431 | Before treatment | 67.29 | 32.53 | 0.18 |
| After treatment | 66.85 | 32.22 | 0.93 | |
| TE2 | Before treatment | 74.79 | 21.59 | 3.63 |
| After treatment | 63.43 | 28.57 | 8.00 | |
| TE3 | Before treatment | 83.23 | 16.59 | 0.18 |
| After treatment | 77.95 | 21.75 | 0.30 | |
Discussion
CRTx has been widely applied to patients with ESCC due to its marked therapeutic effect, although its basic mechanism has not been thoroughly examined. In this study, the in vitro radiation-sensitizing effect of docetaxel was elucidated. It was observed that a non-cytocidal concentration of docetaxel may have affected the cell cycle at the G2/M stage and improved the anti-tumor effect of radiotherapy.
Although previous studies have revealed the utility of combined anticancer drug and radiation treatment, few studies have demonstrated the synergistic effect of anticancer agents with radiation (19–22). The majority of previous studies have used a high concentration of an anticancer agent capable of reducing the cell survival rate by itself; consequently, the slopes of the cell survival curves for combined CRTx and radiation alone were similar, indicating that the anticancer agents only had an additive effect. By contrast, the noncytocidal concentration of docetaxel was determined in the present study prior to any treatments; chemoradiotherapy using these very low concentrations of docetaxel was capable of reducing the cell survival rate, increasing the slope of the survival curve. These findings clearly indicated that docetaxel had a synergistic effect on radiation, i.e., a radiation-sensitizing effect. When the various cell lines were compared, the order of sensitivity to docetaxel was the inverse of the order of radiosensitivity among the cells used in the present study, and the cell-killing effect of combined chemoradiotherapy reflected the sensitivity of the cells to docetaxel. These findings also supported the hypothesis that docetaxel has a radiation-sensitizing effect on SCC cell lines.
We have previously used etoposide at a concentration that did not have a cell-killing effect and performed CRTx in vitro on Chinese hamster-related V79 cells, human bladder cancer-derived T24 cells, human breast cancer-derived MDA-MB231 cells, and human ovarian cancer-derived RGMT cells, and demonstrated that etoposide had a radiation-sensitizing effect among certain types of cell lines (25). These findings indicated that a low-concentration method was useful for assessing the synergistic effect of a chemotherapy agent on radiation. The present study was performed on the basis of these previous findings.
Significantly, the timing of docetaxel may affect the therapeutic efficacy of chemoradiotherapy. Previous studies have revealed a radiation-sensitizing effect after the contact of ESCC cells with CDDP. As we expected, radiation produced the strongest cell-killing effect immediately after contact with docetaxel. With regard to the action mechanism of this effect, intracellular and extracellular factors require further investigation. Since the cell cycle may be related to the radiation efficacy, flow cytometry was performed to assess the cell cycle distribution, and it was demonstrated that the administration of docetaxel increased the cell fraction in the G2/M stage. The G2/M phase is considered to be the most radiosensitive period, resulting in a high radiation-sensitizing effect after contact with docetaxel (26–28).
The pharmacological action of docetaxel is unique. Docetaxel mainly affects tubulin (especially β-tubulin), which is a protein that is suspended in cells; docetaxel promotes polymerization and arrests cell division by inhibiting microtubular depolymerization (6). This mechanism results in the synchronization of the cell cycle during G2/M phase, when radiosensitivity is at its highest, due to the large quantity of microtubes (26,27). Using flow cytometry, an increase in the G2/M cell fraction was observed even after contact with a non-cytocidal concentration of docetaxel, consistent with the basic pharmacological mechanism of docetaxel and indicating that this mechanism may be partly responsible for docetaxel's radiation-sensitizing effects.
In this study, three cells lines (TE-2, TE-3, and A431) with a high plating efficiency were selected. Plating efficiency is significant when conducting a colony formation assay where the assessment of cells with a lower cellular proliferation capability is insufficient. This may be clinically related to tumor aggressiveness, and further investigation is required.
With regard to preserving the esophagus and maintaining the patient's QOL, CRTx has several advantages to surgery; however, lethal adverse events have also been reported. Therapies with a marked local effect and fewer general effects are usually considered as being ideal, and CRTx is promising for this reason. Nevertheless, the frequency of adverse events affecting other organs is still being debated. Conventional FP therapy, which is a chemotherapy regimen combined with radiation for esophageal cancer, often requires hospitalization for renal preservation and involves a high treatment cost. Although the usual dose of docetaxel administration evokes adverse events at a rate of approximately 50% (9–12), it may be possible to decrease this rate by reducing the administered dose, since the occurrence of adverse events depends on the concentration of docetaxel. Our findings demonstrated radiation-sensitizing effects after the administration of a low concentration of docetaxel, which may establish a rationale for CRTx using an anticancer agent with a radiation-sensitizing effect that could increase the clinical response and decrease the risk of adverse events. Moreover, in addition to its clinical benefit, the administration of low concentrations of docetaxel might also facilitate administration of CRTx on an outpatient basis, enabling a cost benefit.
In conclusion, this study demonstrated that the administration of a low, non-cytocidal concentration of docetaxel prior to radiation exposure increases the cell-killing effect on SCC cell lines. The increase of the G2/M fraction as a result of the administration of docetaxel may affect this radiation-sensitizing effect.
References
- 1.Herskovic A, Martz K, Al-Sarraf M, et al. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N Engl J Med. 1992;326:1593–1598. doi: 10.1056/NEJM199206113262403. [DOI] [PubMed] [Google Scholar]
- 2.Al-Sarraf M, Martz K, Herskovic A, et al. Progress report of combined chemoradiotherapy versus radiotherapy alone in patients with esophageal cancer: an intergroup study. J Clin Oncol. 1997;15:277–284. doi: 10.1200/JCO.1997.15.1.277. [DOI] [PubMed] [Google Scholar]
- 3.Cooper JS, Guo MD, Herskovic A, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA. 1999;281:1623–1627. doi: 10.1001/jama.281.17.1623. [DOI] [PubMed] [Google Scholar]
- 4.Coia LR, Minsky BD, Berkey BA, et al. Outcomes of patients receiving radiation for cancer of the esophagus: results of the 1992–1994 patterns of care study. J Clin Oncol. 2000;18:455–462. doi: 10.1200/JCO.2000.18.3.455. [DOI] [PubMed] [Google Scholar]
- 5.Ando N, Iizuka T, Ide H, et al. Surgery plus chemotherapy compared with surgery alone for localized squamous cell carcinoma of the thoracic esophagus: A Japan Clinical Oncology Group Study-JCOG9204. J Clin Oncol. 2003;21:4592–4596. doi: 10.1200/JCO.2003.12.095. [DOI] [PubMed] [Google Scholar]
- 6.Ringel I, Horwitz SB. Studies with RP 56976 (Taxotere): a semisynthetic analogue of taxol. J Natl Cancer Inst. 1991;83:288–291. doi: 10.1093/jnci/83.4.288. [DOI] [PubMed] [Google Scholar]
- 7.Garcia P, Braguer D, Carles G, et al. Comparative effects of taxol and taxotere on two different human carcinoma cell lines. Cancer Chemother Pharmacol. 1994;34:335–343. doi: 10.1007/BF00686042. [DOI] [PubMed] [Google Scholar]
- 8.Hanauske AR, Degen D, Hilsenbeck SG, Bissery MC, von Hoff DD. Effects of taxotere and taxol on in vitro colony formation of freshly explanted human tumor cells. Anticancer Drugs. 1992;3:121–124. doi: 10.1097/00001813-199204000-00008. [DOI] [PubMed] [Google Scholar]
- 9.Catimel G, Verweij J, Mattijssen V, et al. Docetaxel (Taxotere): an active drug for the treatment of patients with advanced squamous cell carcinoma of the head and neck. EORTC Early Clinical Trials Group. Ann Oncol. 1994;5:533–537. doi: 10.1093/oxfordjournals.annonc.a058908. [DOI] [PubMed] [Google Scholar]
- 10.Couteau C, Chouaki N, Leyvraz S, et al. A phase II study of docetaxel in patients with metastatic squamous cell carcinoma of the head and neck. Br J Cancer. 1999;81:457–462. doi: 10.1038/sj.bjc.6690715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bang YJ, Kang WK, Kang YK, et al. Docetaxel 75 mg/m2 is active and well tolerated in patients with metastatic or recurrent gastric cancer: a Phase II Trial. Jpn J Clin Oncol. 2002;32:248–254. doi: 10.1093/jjco/hyf057. [DOI] [PubMed] [Google Scholar]
- 12.Dreyfuss AI, Clark JR, Norris CM, et al. Docetaxel: An active drug for squamous cell carcinoma of the head and neck. J Clin Oncol. 1996;14:1672–1678. doi: 10.1200/JCO.1996.14.5.1672. [DOI] [PubMed] [Google Scholar]
- 13.Mauer AM, Masters GA, Haraf DJ, et al. Phase I study of docetaxel with concomitant thoracic radiation therapy. J Clin Oncol. 1998;16:159–164. doi: 10.1200/JCO.1998.16.1.159. [DOI] [PubMed] [Google Scholar]
- 14.Matsuura M, Hasegawa M, Hayakawa K, et al. Experimental study of the effects on apoptosis of docetaxel alone and in combination with irradiation. Oncol Rep. 2000;7:289–293. [PubMed] [Google Scholar]
- 15.Kim ES, Khuri FR. Docetaxel and radiation as combined-modality therapy. Oncol (Williston Park) 2002;16(Suppl 6):97–105. [PubMed] [Google Scholar]
- 16.Fujii M, Tsukuda M, Sakata B, et al. Japan Cooperative Head and Neck Oncology Group (JCHNOG). Phase I/II trial of weekly docetaxel and concomitant radiotherapy for squamous cell carcinoma of the head and neck. Int J Clin Oncol. 2004;9:107–112. doi: 10.1007/s10147-003-0375-z. [DOI] [PubMed] [Google Scholar]
- 17.Koukourakis M, Kourousis C, Kamilaki M, et al. Weekly docetaxel and concomitant boost radiotherapy for non-small-cell lung cancer. A phase I/II dose escalation trial. Eur J Cancer. 1998;34:838–844. doi: 10.1016/s0959-8049(97)10101-0. [DOI] [PubMed] [Google Scholar]
- 18.Segawa Y, Kiura K, Takigawa N, et al. Phase III trial comparing docetaxel and cisplatin combination chemotherapy with mitomycin, vindesine, and cisplatin combination chemotherapy with concurrent thoracic radiotherapy in locally advanced non-small-cell lung cancer: OLCSG 0007. J Clin Oncol. 2010;28:3299–3306. doi: 10.1200/JCO.2009.24.7577. [DOI] [PubMed] [Google Scholar]
- 19.Choy H, Rodriguez F, Koester S, et al. Synergistic effect of taxol/taxotere on radiation sensitivity on human tumor cell lines. Int J Radiat Oncol Biol Phys. 1992;24(Suppl):274–275. [Google Scholar]
- 20.Pradier O, Rave-Fränk M, Lehmann J, et al. Effects of docetaxel in combination with radiation on human head and neck cancer cells (ZMK-1) and cervical squamous cell carcinoma cells (CASKI) Int J Cancer. 2001;91:840–845. doi: 10.1002/1097-0215(200002)9999:9999<::aid-ijc1142>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 21.Hennequin C, Giocanti N, Favaudon V. Interaction of ionizing radiation with paclitaxel (Taxol) and docetaxel (Taxotere) in HeLa and SQ20B cells. Cancer Res. 1996;56:1842–1850. [PubMed] [Google Scholar]
- 22.Creane M, Seymour CB, Colucci S, Mothersill C. Radiobiological effect of docetaxel (Taxotere): a potential radiation sensitizer. Int J Radiat Biol. 1999;75:731–737. doi: 10.1080/095530099140078. [DOI] [PubMed] [Google Scholar]
- 23.Mason KA, Hunter NR, Milas M, Abbruzzese JL, Milas L. Docetaxel enhances tumor radioresponse in vivo. Clin Cancer Res. 1997;3:2431–2438. [PubMed] [Google Scholar]
- 24.Mason KA, Kishi K, Hunter N, et al. Effect of docetaxel on the therapeutic ratio of fractionated radiotherapy in vivo. Clin Cancer Res. 1999;5:4191–4198. [PubMed] [Google Scholar]
- 25.Shigematsu N, Kawata T, Ihara N, et al. Effect of combined treatment with radiation and low dose etoposide on cell survival. Anticancer Res. 2001;21:325–328. [PubMed] [Google Scholar]
- 26.Withers HR, Mason K, Reid BO, et al. Response of mouse intestine to neutrons and gamma rays in relation to dose fractionation and division cycle. Cancer. 1974;34:39–47. doi: 10.1002/1097-0142(197407)34:1<39::aid-cncr2820340107>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 27.Hartwell LH, Weinert TA. Checkpoints: controls that ensure the order of cell cycle events. Science. 1989;246:629–634. doi: 10.1126/science.2683079. [DOI] [PubMed] [Google Scholar]
- 28.Dolbeare F, Beisker W, Pallavicini MG, Vanderlaan M, Gray JW. Cytochemistry for bromodeoxyuridine/DNA analysis: stoichiometry and sensitivity. Cytometry. 1985;6:521–530. doi: 10.1002/cyto.990060606. [DOI] [PubMed] [Google Scholar]