
Figure 5.
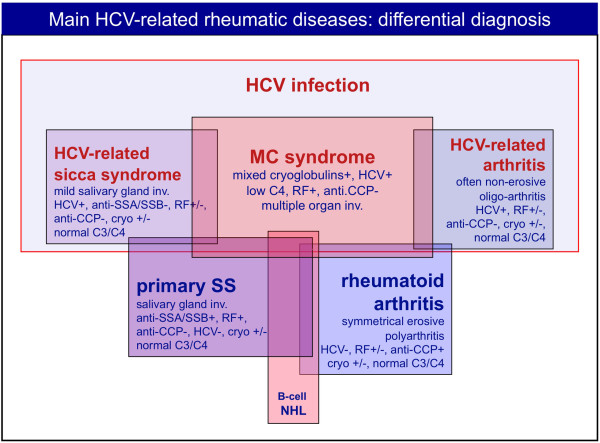
Differential diagnosis between some important hepatitis C virus-associated rheumatic manifestations and classical diseases such as primary Sjögren's syndrome and rheumatoid arthritis is possible on the basis of clinico-serological and pathological features. Some important findings may be usefully employed for a correct diagnosis: the histopathological characteristics and severity of salivary gland involvement and specific autoantibodies (anti-SSA/SSB) are rarely found in hepatitis C virus (HCV)-associated sicca syndrome or mixed cryoglobulinemia syndrome (MCs) patients. Conversely, cutaneous leukocytoclastic vasculitis, visceral organ involvement (hepatitis, membranoproliferative- glomerulonephritis), abnormally low complement C4, and HCV infection, typically found in MCs, are very uncommon in primary Sjögren's syndrome (pSS). Both MCs and pSS may be complicated by B-cell non-Hodgkin's lymphoma (B-cell NHL), and less frequently also rheumatoid arthritis patients. Finally, erosive symmetrical polyarthritis and serum anti-cyclic citrullinated peptide (anti-CCP) antibodies are specific diagnostic findings of classical rheumatoid arthritis, but generally absent in HCV-associated arthritis. However, there is a gray area of clinical overlap between different disorders. RF, rheumatoid factor.