

Sir,
Menkes kinky hair disease is a rare X-linked recessive disorder of copper metabolism.[1,2] In 1962, Menkes first described the syndrome and Drank et al. noted the association with copper metabolism.[3] In Menkes kinky hair disease, intestinal copper uptake is normal, but copper transport to other tissues is affected. The defective protein is a copper-binding ATPase, ATP7A, responsible for distribution and metabolism of copper in tissues. A defect in intestinal copper transport with associated low serum copper and ceruloplasmin levels results in defective functioning of copper-dependent enzymes like lysyl oxydase, cytochrome c oxidase, dopamine β-hydroxylase, tyrosinase, and superoxide dismutase with subsequent clinical manifestations. Depigmentation of hair and skin pallor are due to tyrosinase deficiency, hypothermia is due to cytochrome c oxidase deficiency, and lysyl oxidase deficiency causes tortuous arteries in brain, and progressive vascular changes predispose to thrombosis and deficient blood supply to the developing brain.[2,4,5] Individuals with Menkes kinky hair disease typically have hypotonia and seizures when they are infants. Although development initially appears normal, marked developmental delays are noted within the patient's first year of life. Hair abormalities are the most striking signs in this syndrome. Scalp hair become hypopigmented, sparse, short, and brittle. Skin may become hypopigmented, pale, mottled, and doughy. Examination under microscope reveals a variety of abnormalities, most often pili torti (twisted hair), monilethrix (varying diameter of hair shafts), and trichorrhexis nodosa (fractures of the hair shaft at regular intervals).[6]
A 6-month-old male infant born of nonconsanguineous marriage, admitted in the hospital with the complaint of recurrent respiratory difficulty. The mother informed that the child's social smile was absent and he was not able to recognize her. History of convulsions was not present. He was born at term with normal birth weight. The pregnancy was uneventful. He was the first child of the parents. The head circumference and body weight were 40 cm and 4.7 kg, respectively. Eye contact was absent; the child was not responding to any stimuli. There was no fixation. Ophthalmic examination findings were suggestive of cortical blindness. Fundus examination was within normal limits. He had poor head control and no rollover response, no social smile suggesting developmental delay. The child was referred to skin OPD for hair and cutaneous examination. On clinical examination, the child was irritable with fair complexion, chubby cheeks and depressed nasal bridge [Figures 1a and b]. The most striking finding was the appearance of the scalp hair. Hair were hypopigmented, short, sparse, thin, brittle and kinky [Figure 2]. The scalp hair were fragile and fractured easily, resulting in apparent generalized alopecia [Figure 1]. MRI of brain showed delayed myelination of white matter corresponding to myelination at birth. Demyelination involving optic radiation and occipital lobe was noted. Serum copper and ceruloplasmin levels were lower than normal values; with 54 μg/dl (ref. 70-155) and 8.3 mg/dl (ref. 187-320 mg/l) respectively. Light microscopic examination of the scalp hair showed pili torti (twisted hair shafts) [Figures 3 and 4]. There were no metaphyseal changes of long bones on X-rays. Routine blood investigations and abdominal ultrasonography were within normal limits. The child was treated symptomatically for acute lower respiratory tract infection and was put on B-complex and mineral supplements. The child was advised to come for monthly follow-ups.
Figure 1a.

Child with fair complexion, chubby cheeks, and depressed nasal bridge. Note the generalized alopecia of scalp
Figure 1b.
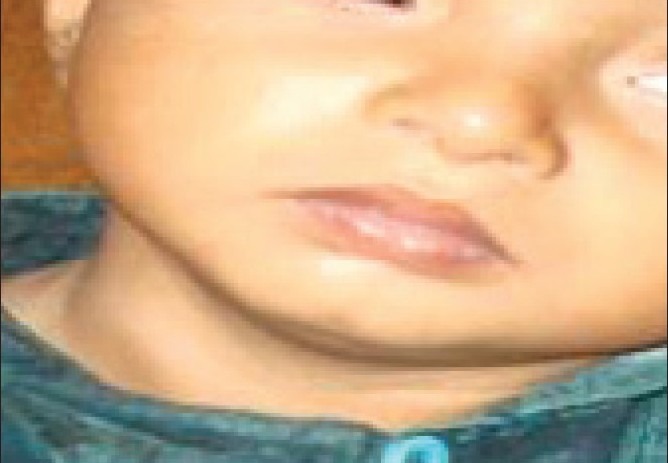
Child with fair complexion, chubby cheeks, and depressed nasal bridge
Figure 2.

Hypopigmented, short, sparse, thin, brittle, and kinky scalp hair
Figure 1.

a: Child with fair complexion, chubby cheeks, and depressed nasal bridge. Note the generalized alopecia of scalp. b: Child with fair complexion, chubby cheeks, and depressed nasal bridge
Figure 3.
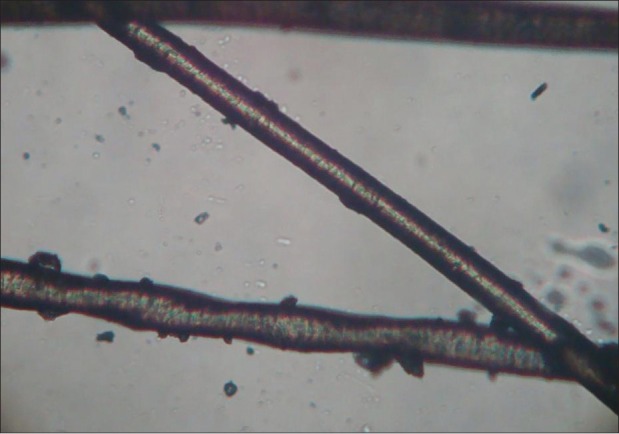
Light microscopic examination of the scalp hair showing pili torti
Figure 4.

Light microscopic examination of the scalp hair showing pili torti
Menkes disease almost exclusively affects males and females are the carrier. There is no race predilection. The disease becomes evident at the age of 2-3 months; patients die by the time they are 3-4 years old usually because of pneumonia, although some patients with Menkes disease may die suddenly.[7] Our patient was a male child presented at the age of 6 months. The clinical spectrum of Menkes disease encompasses several distinct variants. Individuals with the mild variant are developmentally delayed with cerebellar ataxia, dysarthria and pili torti, and no seizures. In our case the child was evaluated for delayed developmental milestones by paediatricians and was sent to us for hair examination. There was no history of seizure in our case. The absence of social smile, poor head control, and no rollover response suggest developmental delay in our case. The characteristic facial appearance with fair complexion, chubby cheeks, and depressed nasal bridge in our case was similar to the reported cases in the past.[8–10] The scalp hair may appear normal at birth, but at approximately 3 months of age the hair on the scalp and eyebrows becomes kinky, coarse, and lightens in color.[1,4,5] Our case also had hypopigmented, short, sparse, thin, brittle, and kinky hair on the scalp and normal eyebrows and eyelashes. Microscopic examination of the hair is very helpful even in a mild case. Several hair shaft abnormalities have been documented, with pili torti being the most common; trichorrehexis nodosa, trichoclasis, and trichoptilosis have also been reported.[6,11] In our case light microscopic examination of scalp hair revealed pili torti. Low levels of serum copper and ceruloplasmin will usually confirm the diagnosis.[5] The early neuroimaging record shows extensive lesions in white matter that seem secondary to a progressive brain destruction and collapse of the myelination process.[12–15]
With the history and clinical findings of developmental delay, characteristic facial appearance and microscopic hair examination findings, we further investigated the case keeping in mind the diagnosis of Menkes kinky hair disease. The diagnosis was confirmed by low serum copper and ceruloplasmin levels and neuroimaging finding of defective myelination of the brain white matter.
We report a case of Menkes kinky hair disease for its classical presentation and rarity.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
References
- 1.Menkes JH. Kinky hair disease. Pediatrics. 1972;50:181–3. [PubMed] [Google Scholar]
- 2.Danks DM, Campbel PE, Walker-Smith J. Menkes kinky-hair syndrome. Lancet. 1972;1:1100–2. doi: 10.1016/s0140-6736(72)91433-x. [DOI] [PubMed] [Google Scholar]
- 3.Drank DM, Cartwright E, Stevens BJ, Townley RR. Menke's kinkey hair disease: Further definition of the defect in copper transport. Science. 1973;1:1140–2. doi: 10.1126/science.179.4078.1140. [DOI] [PubMed] [Google Scholar]
- 4.Menkes JH. Kinky hair disease: Twenty-five years later. Brain Dev. 1998;10:77–9. doi: 10.1016/s0387-7604(88)80074-3. [DOI] [PubMed] [Google Scholar]
- 5.Menkes JH, Wilcox WR. Child Neurology. 7th ed. Philadelphia: Lippincott Williams and Wilkins; 2006. Inherited metabolic disease of the nervous system; pp. 115–7. [Google Scholar]
- 6.Smith VV, Anderson G, Malone M. Light microscopic examination of scalp hair samples as an aid in the diagnosis of pediatric disorders: Retrospective review of more than 300 cases from a single centre. J Clin Pathol. 2005;58:1294–8. doi: 10.1136/jcp.2005.027581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sfaello I, Castelnau P, Blanc N, Ogier H, Evrard P, Arzimanoglou A. Infantile spasms and Menkes disease. Epileptic Disord. 2000;2:227–30. [PubMed] [Google Scholar]
- 8.Tumer Z, Horn N. Menkes disease: Recent advances and new aspects. J Med Genet. 1997;34:265–74. doi: 10.1136/jmg.34.4.265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Menkes JH, Alter M, Steigleder GK. A sex-linked recessive disorder with retardation of growth, peculiar hair, and focal cerebral and cerebellar degeneration. Pediatr. 1962;29:764–79. [PubMed] [Google Scholar]
- 10.Grover WD, Johnson WC, Henkin RI. Clinical and biochemical aspect of Trichopoliody strophy. Ann Neurol. 1979;5:65–71. doi: 10.1002/ana.410050110. [DOI] [PubMed] [Google Scholar]
- 11.Whiting DA. Structural abnormalities of the hair shaft. J Am Acad Dermatol. 1987;16:1–25. doi: 10.1016/s0190-9622(87)70001-2. [DOI] [PubMed] [Google Scholar]
- 12.Blaser SI, Berns DH, Ross JS, Lanska MJ, Weissman BM. Serial MR studies in Menkes disease. J Comput Assist Tomogr. 1989;13:113–5. doi: 10.1097/00004728-198901000-00024. [DOI] [PubMed] [Google Scholar]
- 13.Tumer Z, Horn N. Menkes disease: Recent advances and new aspects. J Med Genet. 1997;34:265–74. doi: 10.1136/jmg.34.4.265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ichihashi K, Yano S, Kobayashi S, Miyao M, Yanagisawa M. Serial imaging of Menkes disease. Neuroradiology. 1990;32:56–9. doi: 10.1007/BF00593944. [DOI] [PubMed] [Google Scholar]
- 15.Geller TJ, Pan Y, Martin DS. Early neuroradiologic evidence of degeneration in Menkes disease. Pediatr Neurol. 1997;17:255–8. doi: 10.1016/s0887-8994(97)00092-1. [DOI] [PubMed] [Google Scholar]