
Fig. 5.
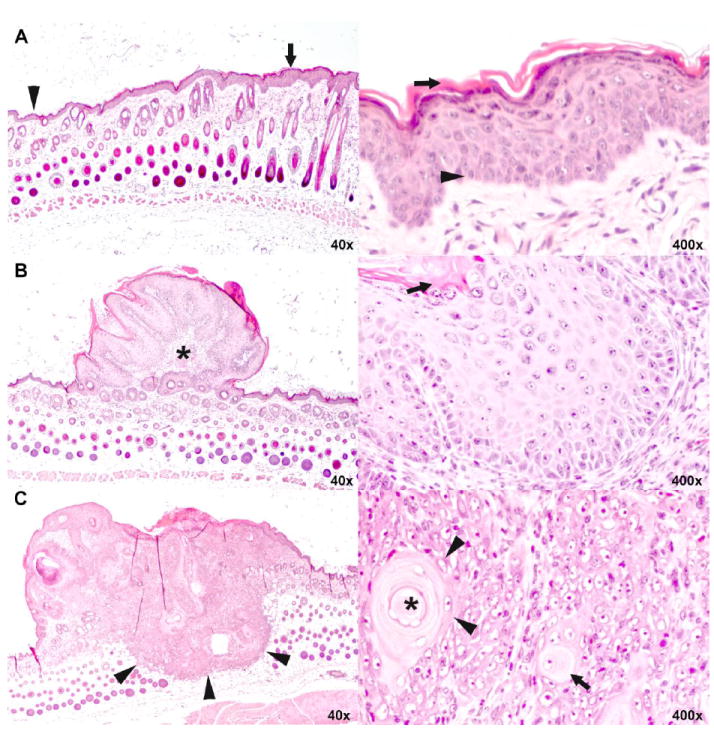
Histopathology of epidermal hyperplasia, squamous papilloma and squamous cell carcinoma of the skin.
A. Low (left) and high (right) magnification of skin with epidermal hyperplasia. In the low magnification, normal thickness of the epidermis is shown on the left (arrow head) and increased thickness of the hyperplastic epidermis on the right (arrow). While the number of cell layers is increased, keratinocytes progress in the same orderly manner from basal cells (arrow head) at bottom to fully keratinized cells (arrow) at top as they do in normal epidermis.
B. Low (left) and high (right) magnification of skin with squamous papilloma. At lower magnification, the small, protruding mass is bordered by epidermis of normal (left) to slightly increased thickness (right). It comprises a fibrovascular core (asterisk) covered with very thick epithelium that, at high magnification, recapitulates orderly keratinization of basal cells (arrow head) to fully keratinized cells (arrow) of normal and hyperplastic epidermis shown in A.
C. Low (left) and high (right) magnification of skin with squamous cell carcinoma. At low magnification, the plaque-like mass has a flat to umbilicated top (asterisk) and deeply infiltrates into the subcutis (arrow heads). At higher magnification, keratinocytes are arranged in solid nests. Individual keratinocytes (arrow) and groups of keratinocytes (arrow heads) haphazardly keratinize without orderly progression. A concentrically layered keratin pearl is present at the upper right (asterisk in center). Note that high magnification is not the same as in A and B.