

Abstract
INTRODUCTION
With the advent of laparoscopic cholecystectomy we have seen a “disease of medical progress” (DOMP). Herein we report a complication that developed 7 years after laparoscopic cholecystectomy.
PRESENTATION OF CASE
A 42 year old woman presented with worsening right-sided pain and tenderness. Seven years prior she underwent a laparoscopic cholecystectomy. Computed tomography demonstrated a subhepatic retroperitoneal inflammatory mass. On open exploration a 4 cm × 6 cm retroperitoneal mass was excised. The mass contained purulent material and gallstones.
DISCUSSION
Laparoscopic cholecystectomy has become the “gold standard” for the treatment of symptomatic gallstones. Prior to laparoscopic cholecystectomy there was no body of literature about lost gallstones thus making this a DOMP. In contrast, it is reported that as many as 5.4–19% of laparoscopic cholecystectomies have stones spilled with variable rates of retrieval. Our case demonstrates an extreme example of a complication resulting seven years after a laparoscopic cholecystectomy with gallstones left behind.
CONCLUSION
Recognizing that gallstones will be lost during some cases of laparoscopic cholecystectomy, we must remain vigilant and make a full attempt to retrieve all stones to prevent such rare but not insignificant potential complications.
Keywords: Gallstone abscess, Laparoscopic cholecystectomy
1. Introduction
Gallstone abscess following spilled gallstones is an extremely rare delayed complication of laparoscopic cholecystectomy.1,2 Common locations of the abscess are in the abdominal wall followed by intra-abdominal cavity usually in the sub-hepatic or retroperitoneum inferior to sub-hepatic space.3 We report a rare case of abscess formation due to spilled gallstones occurring 7 years after laparoscopic cholecystectomy.
2. Case report
A 42 year old female presented to the emergency department with a 1 month history of worsening right sided cramp and constant abdominal. The pain radiated to the back and was associated with low grade fevers, night chills and a 50 pound weight loss over 5 months. Due to the weight loss, imaging studies such as endoscopy and colonoscopies were performed 2 months prior to presentation and revealed no pathology. Her surgical history was significant for a laparoscopic cholecystectomy approximately 7 years ago. She had mild right sided tenderness and a soft palpable mass in the right flank. Laboratory workup revealed white blood cell count of 17,000 mm−3 and all other laboratory findings including liver function tests, amylase and lipase were within the normal limits. Our differential diagnosis included a retroperitoneal sarcoma or a lymphoma. Computed tomography (CT) scan of the abdomen and pelvis revealed a 5 cm × 5 cm right retroperitoneal mass invading the muscle wall with surrounding inflammation (Fig. 1). No biopsies were performed prior to the operation.
Fig. 1.
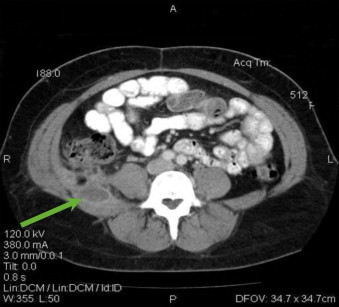
Computed tomography (CT) scan of a retroperitoneal mass. The arrow depicts the retroperitoneal mass invading the adjacent muscle.
Exploratory laparotomy revealed a 4 cm × 6 cm mass which was found to contain purulent material and gallstones (Fig. 2). During the procedure the bowel was easily mobilized and the dissection was not difficult, however the mass was quite adherent to the posterior muscular wall. The retroperitoneal mass was excised along with a small segment of attached liver. 4 ml of pus was found in the center and drained. We excised part of the muscle and approximately 1 cm margin was obtained in case of malignant neoplasm. Pathology examination showed multifaceted gallstones, fibroadipose tissue with chronic granulomatous inflammation, giant cell reaction and focal abscess without malignant cells. It was determined that a frozen section was not necessary as the diagnosis was evident and the mass contained gallstones, pus with surrounding inflammatory tissues. Prior to the procedure the patient underwent complete bowel clean up. At presentation she was noted to have elevated temperature and leukocytosis, she was empirically started on ampicillin/sulbactam, a broad spectrum antibiotic. After the operation and intra-operative findings of the inflammatory mass and pus, metronidazole was added to cover anaerobic bacteria. The pus was sent to the microbiology laboratory and it returned positive for klebsiella and E. coli both sensitive to ampicillin/sulbactam.
Fig. 2.
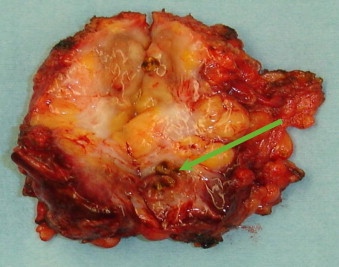
Excised retroperitoneal mass. The arrow indicates a gallstone with surrounding fibroadipose tissue.
On eight months follow up of the patient, this 42 year old lady had gone back to her baseline weight and was completely pain free.
3. Discussion
Since its introduction in 1985 by Erich Mühe of Germany, laparoscopic cholecystectomy has become the gold standard of treatment for symptomatic gallstone disease.4 With morbidity rates ranging from 2% to 11% for laparoscopic cholecystectomy compared to 4–6% for elective open cholecystectomy, laparoscopic cholecystectomy measures reasonably well in comparison.1,2
The benefits of laparoscopic cholecystectomy for gallbladder surgery are significant; however it carries some major complications mainly due to its laparoscopic nature. It minimizes mortality rates in the perioperative period, reduces the length of stay in the hospital and allows for patients to return to their normal activities sooner; when compared to open cholecystectomy.5 The complications however include damage to the biliary system, blood vessels and gastrointestinal tract.6 Additionally, gallbladder perforation by trocars in laparoscopic cholecystectomy leads to bile and gallstone spillage with a reported incidence of 5.4–19%.7 Spilled gallstones are removed with relative ease in open cholecystectomy by irrigating the abdominal cavity and suctioning with a large suction tube or by collecting the stones with a sponge.1 However, this way of retrieving the spilled stones are difficult to achieve in laparoscopic cholecystectomy.1,2,7
Theoretically, spilled gallstones can be displaced to any part of the abdominal cavity leading to several complications. The authors, Zehetner et al. reported many complications due to spilled gallstones during laparoscopic cholecystectomy. Among these complications are notably abdominal wall and intra-abdominal abscesses. The intra-abdominal abscesses are commonly located in the subhepatic space or in its retroperitoneal region. Fistula formations, hernia sacs, ovary and fallopian tubes containing lost gallstones are among some of the rare complications noted for gallstone abscess.3
The diagnosis of gallstone abscess is usually not an obvious one to make upon patient presentation. Abscess formation from dropped stones after laparoscopic cholecystectomy has been reported to have an average duration of 4 months to 10 years.8,9 Physicians involved in the patient care must have a high index of suspicion for gallstone abscess as a complication not only limited to the months following surgery but also including the subsequent years.7,10,11 Surgical history along with imaging studies such as the abdominal ultrasound and CT scan, combine to make the diagnosis of gallstone abscess possible.12
4. Conclusion
Gallstone abscess resulting from spilled gallstones is a rare complication following laparoscopic cholecystectomy. In our case, the history of laparoscopic cholecystectomy 7 years prior, along with the finding of a retroperitoneal mass containing gallstones at surgery and the pathological confirmation made the difficult diagnosis possible. The case highlights the importance of considering the complication of gallstone abscess when an abscess or fistula formation occurs even years after laparoscopic cholecystectomy. It is important that we remain vigilant about such possibility of lost gallstones during surgery. Every effort should be made to retrieve the spilled stones during laparoscopic cholecystectomy in order to prevent such a rare but significant complication.
Conflict of interest statement
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Kuldeep Singh and Ming L. Wang collected the data and wrote the manuscript. Emmanuel Ofori and Aziz Alemi wrote the manuscript. Warren Widmann collected the data and revised the manuscript. Miles Nakaska wrote and submitted the manuscript.
References
- 1.Horton M., Florence G. Unusual abscess pattern following dropped gallstones during laparoscopic cholecystectomy. American Journal of Surgery. 1998;175:375–379. doi: 10.1016/S0002-9610(98)00048-8. [DOI] [PubMed] [Google Scholar]
- 2.Frola C., Cannici F., Cantoni S., Tagliafico E., Luminati T. Peritoneal abscess formation a late complication of gallstone spilled during laparoscopic cholecystectomy. British Journal of Radiology. 1999;72:201–203. doi: 10.1259/bjr.72.854.10365074. [DOI] [PubMed] [Google Scholar]
- 3.Zehetner J., Shamiyeh A., Wayand W Lost gallstones in laparoscopic cholecystectomy: all possible complications. American Journal of Surgery. 2007;193:73–78. doi: 10.1016/j.amjsurg.2006.05.015. [DOI] [PubMed] [Google Scholar]
- 4.Kalid M., Rashid M. Gallstone abscess: a delayed complication of spilled gallstone after laparoscopic cholecystectomy. Emergency Radiology. 2009;16:227–229. doi: 10.1007/s10140-008-0730-5. [DOI] [PubMed] [Google Scholar]
- 5.Schol F.P.G., Go P.M.N.Y.H., Gouma D.J. Risk factors for bile duct injury in laparoscopic cholecystectomy: analysis of 49 cases. The British Journal of Surgery. 1994;81:1786–1788. doi: 10.1002/bjs.1800811225. [DOI] [PubMed] [Google Scholar]
- 6.Deziel D.J., Millikan K.W., Economou S.G., Doolas A., Ko S.T., Airan M.C. Complications of laparoscopic cholecystectomy; a national survey of 4292 hospitals and an analysis of 77,604 cases. American Journal of Surgery. 1993;165:9–14. doi: 10.1016/s0002-9610(05)80397-6. [DOI] [PubMed] [Google Scholar]
- 7.Offiah C., Robinson P., Keeling-Roberts C.S. The one that got away. British Journal of Radiology. 2002;75:393–394. doi: 10.1259/bjr.75.892.750393. [DOI] [PubMed] [Google Scholar]
- 8.Morrin M., Kruskal J., Saldinger P., Kane R. Radiological features of complication arising from dropped gallstone in laparoscopic cholecystectomy patients. American Journal of Roentgenology. 2000;174:1441–1445. doi: 10.2214/ajr.174.5.1741441. [DOI] [PubMed] [Google Scholar]
- 9.Van Brunt P.H., Lanzafame R.J. Subhepatic inflammatory mass after laparoscopic cholecystectomy: a delayed complication of spilled gallstone. Archives of Surgery. 1994;129:882–893. doi: 10.1001/archsurg.1994.01420320108021. [DOI] [PubMed] [Google Scholar]
- 10.McGanan J.P., Stein M. Complication of laparoscopic cholecystectomy: imaging and intervention. American Journal of Roentgenology. 1995;165:1089–1097. doi: 10.2214/ajr.165.5.7572482. [DOI] [PubMed] [Google Scholar]
- 11.Mahale A., Hegde V., Shetty R., Venugopal A., Kumar A. Dropped calculus post laparoscopic cholecystectomy. Indian Journal of Radiology and Imaging. 2001;11(2):81–82. [Google Scholar]
- 12.Whiting J., Welch N.T., Hallissey M.T. Subphrenic abscess caused by gallstones “lost” at laparoscopic cholecystectomy one year previously: management by minimally invasive techniques. Surgical Laparoscopy & Endoscopy. 1997;7:77–78. [PubMed] [Google Scholar]