
Figure 1.
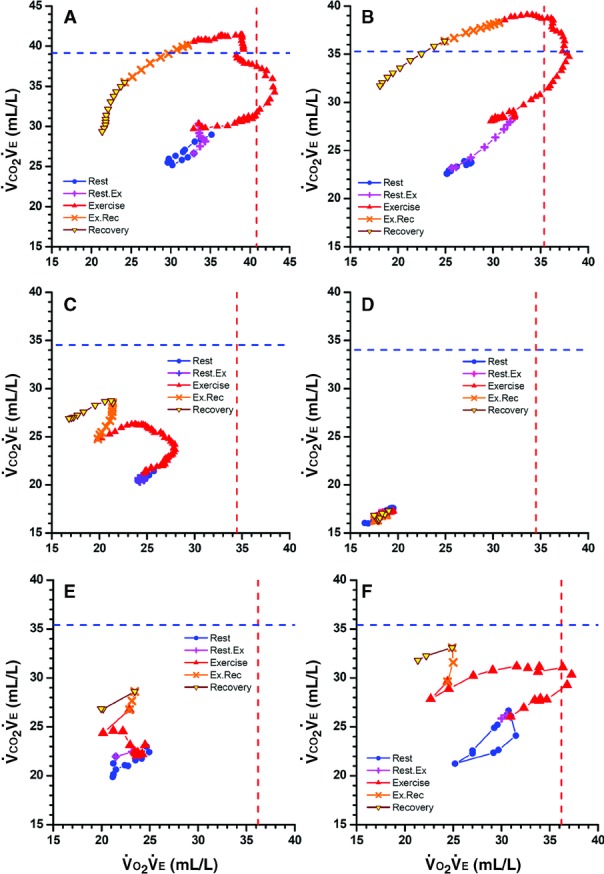
Displays of concurrent 90-s averages of O2 uptake and CO2 output, both divided by exhaled ventilation ( –versus–
–versus– ) during cardiopulmonary exercise testing from rest through early recovery, with “+” and “×” showing transitions between rest and exercise and exercise and recovery. Vertical and horizontal dashed lines are reference highest
) during cardiopulmonary exercise testing from rest through early recovery, with “+” and “×” showing transitions between rest and exercise and exercise and recovery. Vertical and horizontal dashed lines are reference highest  and highest
and highest  . A, Healthy 38-year-old man with peak
. A, Healthy 38-year-old man with peak  106% of predicted. B, Healthy 52-year-old woman with peak
106% of predicted. B, Healthy 52-year-old woman with peak  101% of predicted. Note that with exercise, both numerators increase more than denominators until reaching highest
101% of predicted. Note that with exercise, both numerators increase more than denominators until reaching highest  and then highest
and then highest  before rapid declines, especially in
before rapid declines, especially in  values, during high-intensity exercise and recovery. C, Fifty-seven-year-old woman (NYHA Class II) with moderate left heart failure, oscillatory breathing, and peak
values, during high-intensity exercise and recovery. C, Fifty-seven-year-old woman (NYHA Class II) with moderate left heart failure, oscillatory breathing, and peak  63% of predicted. The shape of the early exercise pattern is reasonable, but the highest
63% of predicted. The shape of the early exercise pattern is reasonable, but the highest  and
and  are well below normal. The rise in
are well below normal. The rise in  during the transition to recovery is abnormal. D, Seventy-three-year-old man (NYHA class IV) with peak
during the transition to recovery is abnormal. D, Seventy-three-year-old man (NYHA class IV) with peak  21% of predicted who died several weeks later. All values are very low. The resting, exercise, and recovery values overlay each other and on magnification can be seen to oscillate. Immediate movement to the lower left at the onset of exercise is an ominous pattern. E and F, Left heart failure in 64-year-old man before and after treatment. Raw data were obtained every 30 s rather than 10 s. In E, values move to the left (
21% of predicted who died several weeks later. All values are very low. The resting, exercise, and recovery values overlay each other and on magnification can be seen to oscillate. Immediate movement to the lower left at the onset of exercise is an ominous pattern. E and F, Left heart failure in 64-year-old man before and after treatment. Raw data were obtained every 30 s rather than 10 s. In E, values move to the left ( is decreasing) and upward with exercise. After treatment, peak
is decreasing) and upward with exercise. After treatment, peak  values increased from 45% to 66% of predicted. In F, resting values start higher and move upward and to the right (indicating
values increased from 45% to 66% of predicted. In F, resting values start higher and move upward and to the right (indicating  is also increasing) before moving leftward. In both studies, the highest
is also increasing) before moving leftward. In both studies, the highest  occurred when
occurred when  ≈21 L/min, at which time
≈21 L/min, at which time  was 25×21=≈520 mL/min (E) and
was 25×21=≈520 mL/min (E) and  was 370×21=≈780 mL/min (F). Thus, this 50% increase in
was 370×21=≈780 mL/min (F). Thus, this 50% increase in  from E to F was primarily due to increased perfusion, not increased ventilation.
from E to F was primarily due to increased perfusion, not increased ventilation.