

Abstract
Context:
Vitamin D is a potent secosteroid hormone that provides many skeletal and extraskeletal health benefits. Musculoskeletal injury prevention and recovery are potentially affected by sufficient circulating levels of the storage form of vitamin D: 25-hydroxyvitamin D3, or 25(OH)D. Vitamin D deficiency can exist among young, active, and healthy people, which may put them at increased risk for injury and prolonged recovery.
Evidence Aquisition:
PubMed was searched using vitamin D and skeletal muscle, vitamin D and athletic performance, and vitamin D review articles. Studies from the 1930s to 2012 were used for the review.
Results:
There is strong correlation between vitamin D sufficiency and optimal muscle function. Increasing levels of vitamin D reduce inflammation, pain, and myopathy while increasing muscle protein synthesis, ATP concentration, strength, jump height, jump velocity, jump power, exercise capacity, and physical performance. 25(OH)D levels above 40 ng/mL are required for fracture prevention, including stress fractures. Optimal musculoskeletal benefits occur at 25(OH)D levels above the current definition of sufficiency (> 30 ng/mL) with no reported sports health benefits above 50 ng/mL.
Conclusions:
Vitamin D deficiency is common in athletes. For athletes presenting with stress fractures, musculoskeletal pain, and frequent illness, one should have a heightened awareness of the additional likely diagnosis of vitamin D deficiency. Correction of this deficiency is completed by standardized and supervised oral supplementation protocols producing significant musculoskeletal sports health benefits.
Keywords: vitamin D, vitamin D deficiency, musculoskeletal, 25-hydroxyvitamin D, vitamin D supplementation
Vitamin D is a necessary nutrient that must be obtained from the diet when sufficient quantities cannot be synthesized. Vitamin D3 is primarily produced following incidental skin exposure to ultraviolet B irradiation, with very little derived from dietary sources (Figure 1).40 Cutaneous production can be absent or dramatically reduced due to skin coloration and sunblock use.2,40 Melanin in the skin of Africans or African Americans blocks nearly 99% of vitamin D production, with similar decreases in cutaneous synthesis achieved following application of SPF 15 sunblock.2,40 Indoor activities, pollution, time of day, increasing age, latitude, and seasonal changes all affect cutaneous vitamin D production.40 As mentioned, very little vitamin D is obtained from dietary sources, including D2 (ergocalciferol, plant) and D3 (cholecalciferol, human) forms. Of note, vitamin D3 is more potent than D2 and should be used for supplementation.3,68 Unfortunately, the average American diet supplies very little of the 4000 to 5000 IU of vitamin D3 used per day, even diets with significant amounts of wild-caught fatty fish.18,36,40,54 The accepted definition of vitamin D sufficiency is 25-hydroxyvitamin D3, (25(OH)D) above 30 ng/mL.21,33,43,44 Based on this definition, vitamin D deficiency affects all age groups and demographics. Fifty to seventy percent of children and adolescents are vitamin D deficient.21,46 Over 75% of whites and 90% of African Americans and Latinos are vitamin D deficient, with increasing age increasing the likelihood of deficiency.10,27,76 In addition, deficiency rates have doubled from 1994 to 2004 with multiple factors responsible, including sun avoidance, sunblock use, and increasing obesity rates causing sequestration of this fat-soluble vitamin.27,51,75 Vitamin D deficiency is associated with numerous health effects, with the musculoskeletal system affected by both genomic and nongenomic mechanisms.
Figure 1.

Production of active vitamin D3. The storage form of vitamin D, calcidiol, or 25(OH)D (black box) is made following liver hydroxylation of vitamin D3 following dietary ingestion or skin synthesis from ultraviolet B exposure (peak skin production follows a 5- to 10-minute exposure of summertime sun between 10 am and 3 pm [produces about 10 000 IU of vitamin D3]). Active vitamin D produced either locally or through the kidney endocrine pathway has its biological effect by altering gene expression through a specific vitamin D response element.
Vitamin D is a secosteroid hormone. Upon activation to 1,25 hydroxyvitamin D3—1,25(OH)D, or calcitriol—vitamin D–responsive gene expression is altered, with over 1000 vitamin D–responsive genes identified (Figure 1).67 These genes affect muscle protein synthesis, muscle strength, muscle size, reaction time, balance, coordination, endurance, inflammation, and immunity—all important to sports health and athletic performance.14,58 Optimal functioning of these sports-related biological processes occurs when vitamin D storage levels approach those obtained by natural, full-body, summer sun exposure.14,29
Vitamin D Deficiency in Elite Athletes
There is no known threshold for optimal sports health benefits of vitamin D; however, peak neuromuscular performance is associated with 25(OH)D levels of 50 ng/mL (Figure 2), well above those considered sufficient.11,34,43 In athletics, the only demographic group that can normally achieve 25(OH)D levels in this range is lifeguards, following a full summer of sun exposure (average 64.4 ng/mL).14,29,43 At present, there is no comprehensive cross-athletic comparison of vitamin D levels; however, the incidence of vitamin D deficiency in elite indoor athletes is up to 94% of basketball players and 83% of gymnasts.52,74 One would assume that participation in outdoor sports provides an advantage for vitamin D production. However, recent reports including testing of New York Giants (football players) during spring practice showed that 81% were vitamin D deficient.64 In this National Football League study, 25(OH)D in white players averaged 30.3 ng/mL, and African Americans averaged 20.4 ng/mL.64 Additionally, a study of elite female soccer players showed that they had an average intake of vitamin D of 163 IU per day. However, results showed that average 25(OH)D levels in the same athletes were 30 ng/mL, possibly owing to the effects of sun exposure.26 Seasonal variations are expected, and current recommendations are for testing athletes in early autumn.24 One example of a seasonal difference in 25(OH)D was in female gymnasts and runners. Sixty-seven percent of participants had levels below 15 ng/mL in winter, with mean levels of 25 ng/mL in summer.50 A study out of Israel looking at athletes between 10 and 30 years old found that 73% had 25(OH)D levels < 30 ng/mL. This study also revealed a significant difference in vitamin D levels in indoor athletes compared with outdoor athletes, with 80% vs 48% being insufficient.19 At present, there is no study to evaluate the relationship of 25(OH)D level and athletic performance enhancement.
Figure 2.
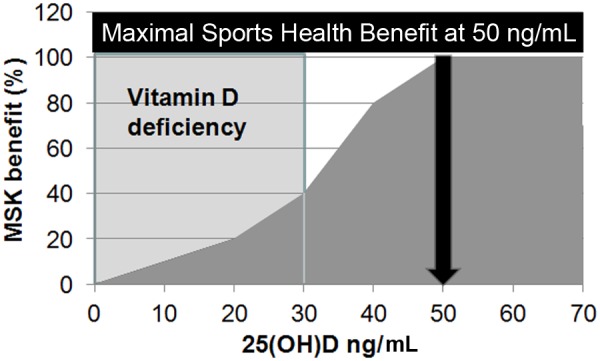
Diagram of sports health benefits of vitamin D. An increase in the storage form of vitamin D is associated with incremental improved musculoskeletal performance. Maximum benefit is achieved in those who are vitamin D deficient (< 30 ng/mL, shaded box). At present, there does not appear to be any added sports health benefit to increasing vitamin D stores above 50 ng/mL.
The concept of performance enhancement with ultraviolet irradiation is not new. It was previously used in Russian and German athletes in the 1930s and 1940s.14 Numerous effects have been reported with improved 100-m times; significant reductions in pain associated with sports injuries; and improved strength, reaction times, speed, and endurance following even a single dose of ultraviolet exposure.14,17,28,36,57,61,65 Application of this technology is difficult because of current opinion on appropriate sun exposure and skin coloration differences. African Americans require 10 times–longer ultraviolet B exposure to generate similar 25(OH)D levels compared with fair-skinned athletes.40 There is also evidence emerging showing the relationship of appropriate vitamin D levels and injury prevention and recovery.64 To highlight the previous football study, players with musculoskeletal injury had 25(OH)D levels substantially lower (average 19.9 ng/mL) than noninjured peers.64
Musculoskeletal Injury and Recovery: A Vitamin D–Regulated Process
Vitamin D is critical to many biological processes in the musculoskeletal system, with a strong correlation noted between vitamin D sufficiency and optimal muscle function.6,16,15,23,31,41 In vitamin D–deficient states, like rickets (Figure 3), generalized musculoskeletal pain is noted with profound myopathy, including muscle weakness, hypotonia, and resultant gait abnormalities.16,77 Physiologically, these deficient states produce muscle fiber atrophy, slow peak muscle contraction, prolonged time to muscle relaxation, and increased risk of chronic musculoskeletal pain.‡ It is important to note that type II, fast-twitch muscle fibers are particularly sensitive to the effects of vitamin D deficiency.58,77 Type II muscle fibers are extremely important in many of the burst activities necessary for peak athletic performance and fall avoidance.6 With vitamin D deficiency, atrophy of type II fibers is noted with fatty infiltration and fibrosis.58,77 Clinically, lower levels of 25(OH)D directly correlate with fatty degeneration of rotator cuff muscles on magnetic resonance imaging.56 It is not known whether vitamin D supplementation can reverse the process of rotator cuff muscle fatty degeneration, but supplementation can reverse the atrophy seen in type II fibers.77 Additionally, reversal of type II fiber atrophy is thought to be responsible for the 20% lower risk of falling with appropriate vitamin D supplementation.9,20 Supplementation with doses < 600 IU per day are ineffective in fall risk reduction, with the minimal level of 25(OH)D required for benefit being 24 ng/mL (Figure 3).9,20
Figure 3.
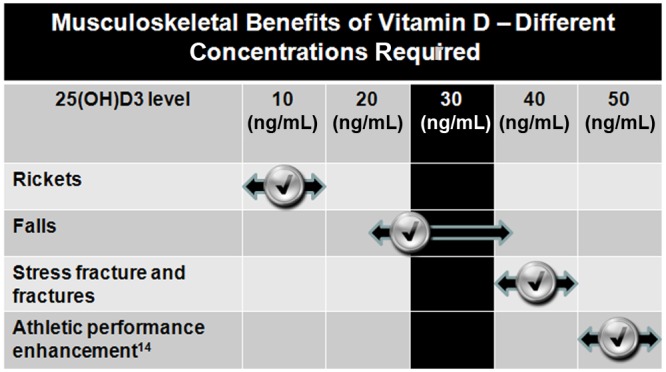
Benefits are concentration dependent. Rickets is easily corrected/prevented with low levels of 25(OH)D. Emerging research indicates that additional sports health benefits require higher concentrations of 25(OH)D than 30 ng/mL, defined as sufficiency (shaded column). These higher levels can be achieved with appropriate supplementation protocols.
Increasing vitamin D levels provides multiple musculoskeletal benefits. Increases in muscle protein synthesis, ATP concentration, strength, jump height, jump velocity, jump power, exercise capacity, and physical performance are achieved with increased vitamin D levels.§ Additionally, increased levels of vitamin D decrease muscle protein degeneration and reverse myalgias.1,8,71 Benefits of supplementation are not limited to muscle alone. It is well known that vitamin D plays an important role in bone health and fracture prevention. In a meta-analysis of randomized controlled trials in older persons, higher dose vitamin D (700-800 IU per day) reduced the relative risk of hip fracture by 26% and nonvertebral fractures by 23% compared with calcium and placebo.13 Optimal fracture prevention occurred at 25(OH)D levels of 40 ng/mL, with identical levels important for stress fracture prevention (Figure 3).12,47,62,69 In a randomized control study evaluating vitamin D and calcium in female military recruits, the subjects received 2000 mg of calcium and 800 IU of vitamin D or placebo, and those receiving the supplements had a 20% reduction in fracture injury.47
Finally, recent studies have shown that vitamin D has immunomodulatory effects, with increased vitamin D levels reducing inflammation.74 Also, proinflammatory cytokines such as TNF-alpha and interleukin-6 are increased with lower levels of serum 25(OH)D, especially after intense periods of exercise.73 This period of increased inflammation has been theorized as one of the potential causes of “overtraining” or “overreaching” syndrome.49 Theoretically, if athletes increased their levels of vitamin D by supplementation, inflammation would be reduced, and training could be resumed more quickly.
Increased levels of vitamin D are correlated with numerous musculoskeletal and immune system benefits, including reductions in the reported incidence of colds and flu.49 Vitamin D status in the spring was correlated with frequency of illness (r = −0.40, P = 0.05) in division I collegiate athletes.30 Athletes, especially those injured or those with frequent infections, should have vitamin D levels measured and deficiencies corrected.30 Additionally, identification and treatment of vitamin D deficiency are important because of the expanding role of vitamin D in reducing the risk and impact of diabetes, multiple sclerosis, certain cancers, cardiovascular diseases and hypertension, cerebrovascular diseases, infectious diseases, asthma, depression, and other autoimmune and chronic inflammatory disorders.22,41
Supplementation
Vitamin D supplementation has already been widely accepted for musculoskeletal health benefits and disease prevention. 25(OH)D levels below 5 ng/mL are associated with a high prevalence of rickets.5,7 Initial milk supplementation programs began in the 1930s to prevent rickets, with an 8-oz serving of milk providing 98 IU of vitamin D.38 Ingestion of 100 IU of vitamin D3 per day is expected to increase serum levels of 25(OH)D by only 1 ng/mL.48 Rickets is therefore easily prevented by low-level ingestion or incidental cutaneous synthesis of vitamin D, with up to 99% prevention by 25(OH)D levels of 18 ng/mL and 50% prevention at 7 ng/mL.4,25 Much higher levels of 25(OH)D are needed to obtain sports health benefits (Figure 3).
Recommendations for Athletes
There are no recommended screening guidelines for vitamin D deficiency. Vitamin D deficiency is diagnosed with a simple 25(OH)D blood test. There appears to be no clinical utility in measuring D2 and D3 levels separate from total 25(OH)D levels.12,21,33 Musculoskeletal benefits may be derived from diagnosis and correction of a deficient state. There is no apparent benefit from 25(OH)D levels above 50 ng/mL.11,34,43 Testing and supplementation protocols should be under the direct supervision of a health care professional, especially since there is variation in response.
If an athlete is vitamin D deficient, 25(OH)D < 30 ng/mL, supplementation protocols require 50 000 IU of vitamin D3 per week for 8 weeks.40 A steady state level of 25(OH)D is achieved after about 90 days of supplementation.36 Once supplementation is completed, retesting is recommended at 3 months. If 25(OH)D remains below 30 ng/mL, repeating the supplementation protocol for another 8 weeks, and retesting is recommended.40 Once sufficiency is documented, continued supplementation as directed by the National Academy of Science should be used.55
The National Academy of Science has commented on upper levels (4000 IU of vitamin D3 for adolescents and adults) of intake for vitamin D and calcium (Figure 4).55 With sufficient 25(OH)D levels, it is unnecessary to exceed intake 4000 to 5000 IU vitamin D3 per day.18,36,40,54 Sun exposure does have an advantage over vitamin D supplementation because cutaneous synthesis has a negative feedback loop preventing vitamin D accumulation and toxicity (Figure 1).2,39 Cutaneous synthesis is difficult to achieve with current opinion on appropriate sun exposure.2 Dietary supplementation therefore may be necessary. Extended oral dosing studies have been completed, and 10 000 IU per day is defined as the tolerable upper-intake level without toxicity reported.32,36,35 Even with a 5-month supplementation protocol of 10 000 IU per day, no adverse events were reported without toxicity at 25(OH)D levels below 200 ng/mL.32,35 Taking 10000 IU per day is not recommended with incremental increases in 25(OH)D by 70 ng/ml; well over the amount of 50ng/ml needed for optimal sports health benefits (Figure 2).36 Another alternative and easily accomplished approach to maintain long-term vitamin D sufficiency is by taking 50 000 IU of vitamin D once or twice a month.42
Figure 4.
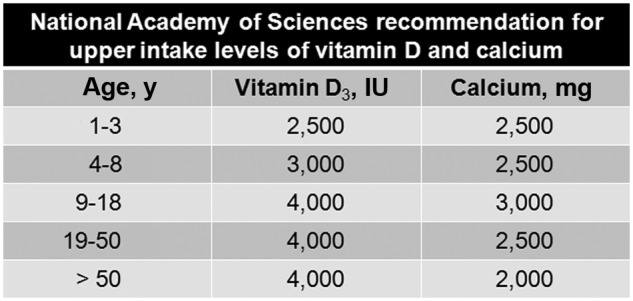
National Academy of Sciences upper limits. “Upper intake levels represent the upper safe boundary and should not be misunderstood as amounts people need or should strive to consume.” Adapted from http://www8.nationalacademies.org/onpinews/newsitem.aspx?RecordID=13050.
Conclusions
There appears to be health and performance benefits of adequate vitamin D levels in athletes.11,12,34,43,47,62,69 Because vitamin D deficiency is common in athletes52,74 the diagnosis of vitamin D deficiency in athletes presenting with stress fractures, musculoskeletal pain, and frequent illness should be considered.11,12,34,43,47,62,69 This deficiency can be corrected by standardized, generally safe and effective oral supplementation protocols.40

Footnotes
References
- 1. Ahmed W, Kahn N, Glueck CJ, et al. Low serum 25(OH) vitamin D levels (<32ng/ml) are associated with reversible myositis-myalgia in statin-treated patients. Transl Res. 2009;153(1):11-16 [DOI] [PubMed] [Google Scholar]
- 2. Armas LA, Dowell S, Akhter M, et al. Ultraviolet-B radiation increases serum 25-hydroxyvitamin D levels: the effect of UVB dose and skin color. J Am Acad Dermatol. 2007;57(4):588-593 [DOI] [PubMed] [Google Scholar]
- 3. Armas LA, Hollis BW, Heaney RP. Vitamin D2 is much less effective than vitamin D3 in humans. J Clin Endocrinol Metab. 2004;89(11):5387-5391 [DOI] [PubMed] [Google Scholar]
- 4. Arnaud SB, Stickler GB, Haworth JC. Serum 25-hydroxyvitamin D in infantile rickets. Pediatrics. 1976;57(2):221-225 [PubMed] [Google Scholar]
- 5. Barger-Lux MJ, Heaney RP, Dowell S, Chen TC, Holick MF. Vitamin D and its major metabolites: serum levels after graded oral dosing in healthy men. Osteoporos Int. 1998;8(3):222-230 [DOI] [PubMed] [Google Scholar]
- 6. Bartoszewska M, Kamboj M, Patel DR. Vitamin D, muscle function, and exercise performance. Pediatr Clin North Am. 2010;57(3):849-861 [DOI] [PubMed] [Google Scholar]
- 7. Bikle DD. Vitamin D: newly discovered actions require reconsideration of physiologic requirements. Trends Endocrinol Metab. 2010;21(6):375-384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Birge SJ, Haddad JG. 25-hydroxycholecalciferol stimulation of muscle metabolism. J Clin Invest. 1975;56(5):1100-1107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Bischoff HA, Stähelin HB, Dick W, et al. Effects of vitamin D and calcium supplementation on falls: a randomized controlled trial. J Bone Miner Res. 2003;18(2):343-351 [DOI] [PubMed] [Google Scholar]
- 10. Bischoff-Ferrari HA, Dietrich T, Orav EJ, Dawson-Hughes B. Positive association between 25-hydroxy vitamin D levels and bone mineral density: a population-based study of younger and older adults. Am J Med. 2004;116(9):634-639 [DOI] [PubMed] [Google Scholar]
- 11. Bischoff-Ferrari HA, Dietrich T, Orav EJ, et al. Higher 25-hydroxyvitamin D concentrations are associated with better lower-extremity function in both active and inactive persons aged > or = 60 y. Am J Clin Nutr. 2004;80(3):752-758 [DOI] [PubMed] [Google Scholar]
- 12. Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr. 2006;84(1):18-28 [DOI] [PubMed] [Google Scholar]
- 13. Bischoff-Ferrari HA, Willett WC, Wong JB, Giovannucci E, Dietrich T, Dawson-Hughes B. Fracture prevention with vitamin D supplementation: a meta-analysis of randomized controlled trials. JAMA. 2005;293(18):2257-2264 [DOI] [PubMed] [Google Scholar]
- 14. Cannell JJ, Hollis BW, Sorenson MB, Taft TN, Anderson JJ. Athletic performance and vitamin D. Med Sci Sports Exerc. 2009;41(5):1102-1110 [DOI] [PubMed] [Google Scholar]
- 15. Ceglia L. Vitamin D and its role in skeletal muscle. Curr Opin Clin Nutr Metab Care. 2009;12(6):628-633 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Ceglia L. Vitamin D and skeletal muscle tissue and function. Mol Aspects Med. 2008;29(6):407-414 [DOI] [PubMed] [Google Scholar]
- 17. Cheatum BA. Effects of a single biodose of ultraviolet radiation upon the speed of college women. Res Q. 1968;39(3):482-485 [PubMed] [Google Scholar]
- 18. Chen TC, Chimeh F, Lu Z, et al. Factors that influence the cutaneous synthesis and dietary sources of vitamin D. Arch Biochem Biophys. 2007;460(2):213-217 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Constantini NW, Arieli R, Chodick G, Dubnov-Raz G. High prevalence of vitamin D insufficiency in athletes and dancers. Clin J Sport Med. 2010;20(5):368-371 [DOI] [PubMed] [Google Scholar]
- 20. Dawson-Hughes B. Serum 25-hydroxyvitamin D and muscle atrophy in the elderly. Proc Nutr Soc. 2012;71(1):46-49 [DOI] [PubMed] [Google Scholar]
- 21. Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R. Estimates of optimal vitamin D status. Osteoporos Int. 2005;16(7):713-716 [DOI] [PubMed] [Google Scholar]
- 22. de Torrenté de la Jara G, Pécoud A, Favrat B. Female asylum seekers with musculoskeletal pain: the importance of diagnosis and treatment of hypovitaminosis D. BMC Fam Pract. 2006;7:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Dirks-Naylor AJ, Lennon-Edwards S. The effects of vitamin D on skeletal muscle function and cellular signaling. J Steroid Biochem Mol Biol. 2011;125(3-5):159-168 [DOI] [PubMed] [Google Scholar]
- 24. Galan F, Ribas J, Sánchez-Martinez PM, Calero T, Sánchez AB, Muñoz A. Serum 25-hydroxyvitamin D in early autumn to ensure vitamin D sufficiency in mid-winter in professional football players. Clin Nutr. 2012;31(1):132-136 [DOI] [PubMed] [Google Scholar]
- 25. Garland CF, Baggerly CA. Disease incidence prevention by serum 25(OH)D level. http://www.grassrootshealth.net/media/download/disease_incidence_prev_chart_101608.pdf Accessed January 22, 2012
- 26. Gibson JC, Stuart-Hill L, Martin S, Gaul C. Nutrition status of junior elite Canadian female soccer athletes. Int J Sport Nutr Exerc Metab. 2011;21(6):507-514 [DOI] [PubMed] [Google Scholar]
- 27. Ginde AA, Liu MC, Camargo CA. Demographic differences and trends of vitamin D insufficiency in the US population, 1988-2004. Arch Intern Med. 2009;169(6):626-632 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Gorkin Z, Gorkin MJ, Teslenko NE. The effect of ultraviolet irradiation upon training for 100m sprint. Fiziol Zh USSR. 1938;25:695-701 [Google Scholar]
- 29. Haddad JG, Chyu KJ. Competitive protein-binding radioassay for 25-hydroxycholecalciferol. J Clin Endocrinol Metab. 1971;33(6):992-995 [DOI] [PubMed] [Google Scholar]
- 30. Halliday TM, Peterson NJ, Thomas JJ, Kleppinger K, Hollis BW, Larson-Meyer DE. Vitamin D status relative to diet, lifestyle, injury, and illness in college athletes. Med Sci Sports Exerc. 2011;43(2):335-343 [DOI] [PubMed] [Google Scholar]
- 31. Hamilton B. Vitamin D and human skeletal muscle. Scand J Med Sci Sports. 2010;20(2):182-190 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Hathcock JN, Shao A, Vieth R, Heaney RP. Risk assessment for vitamin D. Am J Clin Nutr. 2007;85(1):6-18 [DOI] [PubMed] [Google Scholar]
- 33. Heaney RP. Functional indices of vitamin D status and ramifications of vitamin D deficiency. Am J Clin Nutr. 2004;80(6):1706S-1709S [DOI] [PubMed] [Google Scholar]
- 34. Heaney RP. Vitamin D: criteria for safety and efficacy. Nutr Rev. 2008;66(10)(suppl 2):S178-S181 [DOI] [PubMed] [Google Scholar]
- 35. Heaney RP, Armas LA, Shary JR, Bell NH, Binkley N, Hollis BW. 25-Hydroxylation of vitamin D3: relation to circulating vitamin D3 under various input conditions. Am J Clin Nutr. 2008;87(6):1738-1742 [DOI] [PubMed] [Google Scholar]
- 36. Heaney RP, Davies KM, Chen TC, Holick MF, Barger-Lux MJ. Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am J Clin Nutr. 2003;77(1):204-210 [DOI] [PubMed] [Google Scholar]
- 37. Hicks GE, Shardell M, Miller RR, et al. Associations between vitamin D status and pain in older adults: the Invecchiare in Chianti study. J Am Geriatr Soc. 2008;56:785-791 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Higdon J, Drake VJ, DeLuca HF, Vitamin D. [Accessed January 22, 2012]. http://lpi.oregonstate.edu/infocenter/vitamins/vitaminD/
- 39. Holick MF. Sunlight “D”ilemma: risk of skin cancer or bone disease and muscle weakness. Lancet. 2001;357(9249):4-6 [DOI] [PubMed] [Google Scholar]
- 40. Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266-281 [DOI] [PubMed] [Google Scholar]
- 41. Holick MF. The vitamin D deficiency pandemic and consequences for nonskeletal health: mechanisms of action. Mol Aspects Med. 2008;29(6):361-368 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Holick MF. Vitamin D deficiency: what a pain it is. Mayo Clin Proc. 2003;78(12):1457-1459 [DOI] [PubMed] [Google Scholar]
- 43. Hollis BW. Circulating 25-hydroxyvitamin D levels indicative of vitamin D sufficiency: implications for establishing a new effective dietary intake recommendation for vitamin D. J Nutr. 2005;135(2):317-322 [DOI] [PubMed] [Google Scholar]
- 44. Hollis BW, Wagner CL, Drezner MK, Binkley NC. Circulating vitamin D3 and 25-hydroxyvitamin D in humans: an important tool to define adequate nutritional vitamin D status. J Steroid Biochem Mol Biol. 2007;103(3-5):631-634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Houston DK, Cesari M, Ferrucci L, et al. Association between vitamin D status and physical performance: the InCHIANTI Study. J Gerontol A Biol Sci Med Sci. 2007;62(4):440-446 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Kumar J, Muntner P, Kaskel FJ, Hailpern SM, Melamed ML. Prevalence and associations of 25-hydroxyvitamin D deficiency in US children: NHANES 2001-2004. Pediatrics. 2009;124(3):362-370 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Lappe J, Cullen D, Haynatzki G, Recker R, Ahlf R, Thompson K. Calcium and vitamin D supplementation decreases incidence of stress fractures in female navy recruits. J Bone Miner Res. 2008;23(5):741-749 [DOI] [PubMed] [Google Scholar]
- 48. Lappe JM. The role of vitamin D in human health: a paradigm shift. J Evid Based Comp Alt Med. 2011;16:58-72 [Google Scholar]
- 49. Larson-Meyer DE, Willis KS. Vitamin D and athletes. Curr Sports Med Rep. 2010;9(4):220-226 [DOI] [PubMed] [Google Scholar]
- 50. Lehtonen-Veromaa M, Möttönen T, Irjala K, et al. Vitamin D intake is low and hypovitaminosis D common in healthy 9- to 15-year-old Finnish girls. Eur J Clin Nutr. 1999;53(9):746-751 [DOI] [PubMed] [Google Scholar]
- 51. Looker AC, Pfeiffer CM, Lacher DA, Schleicher RL, Picciano MF, Yetley EA. Serum 25-hydroxyvitamin D status of the US population: 1988-1994 compared with 2000-2004. Am J Clin Nutr. 2008;88(6):1519-1527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Lovell G. Vitamin D status of females in an elite gymnastics program. Clin J Sport Med. 2008;18(2):159-161 [DOI] [PubMed] [Google Scholar]
- 53. Mowé M, Haug E, Bøhmer T. Low serum calcidiol concentration in older adults with reduced muscular function. J Am Geriatr Soc. 1999;47(2):220-226 [DOI] [PubMed] [Google Scholar]
- 54. Nesby-O’Dell S, Scanlon KS, Cogswell ME, et al. Hypovitaminosis D prevalence and determinants among African American and white women of reproductive age: third National Health and Nutrition Examination Survey, 1988-1994. Am J Clin Nutr. 2002;76(1):187-192 [DOI] [PubMed] [Google Scholar]
- 55. News from the National Academies IOM report sets new dietary intake levels for calcium and vitamin D to maintain health and avoid risks associated with excess. http://www8.nationalacademies.org/onpinews/newsitem.aspx?RecordID=13050 Accessed January 22, 2012
- 56. Oh JH, Kim SH, Kim JH, Shin YH, Yoon JP, Oh CH. The level of vitamin D in the serum correlates with fatty degeneration of the muscles of the rotator cuff. J Bone Joint Surg Br. 2009;91(12):1587-1593 [DOI] [PubMed] [Google Scholar]
- 57. Parade GW, Otto H. Effect of sunlamp on performance. Zeitschrift fur Klinische Medizin. 1940;137:17-21 [Google Scholar]
- 58. Pfeifer M, Begerow B, Minne HW. Vitamin D and muscle function. Osteoporos Int. 2002;13(3):187-194 [DOI] [PubMed] [Google Scholar]
- 59. Plotnikoff GA, Quigley JM. Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin Proc. 2003;78(12):1463-1470 [DOI] [PubMed] [Google Scholar]
- 60. Rodman JS, Baker T. Changes in the kinetics of muscle contraction in vitamin D-depleted rats. Kidney Int. 1978;13(3):189-193 [DOI] [PubMed] [Google Scholar]
- 61. Rosentsweig J. The effect of a single suberythemic biodose of ultraviolet radiation upon the strength of college women. J Assoc Phys Ment Rehabil. 1967;21(4):131-133 [PubMed] [Google Scholar]
- 62. Ruohola JP, Laaksi I, Ylikomi T, et al. Association between serum 25(OH)D concentrations and bone stress fractures in Finnish young men. J Bone Miner Res. 2006;21(9):1483-1488 [DOI] [PubMed] [Google Scholar]
- 63. Sato Y, Iwamoto J, Kanoko T, Satoh K. Low-dose vitamin D prevents muscular atrophy and reduces falls and hip fractures in women after stroke: a randomized controlled trial. Cerebrovasc Dis. 2005;20(3):187-192 [DOI] [PubMed] [Google Scholar]
- 64. Shindle MK, Voos JE, Gulotta L, et al. Vitamin D status in a professional American football team [ID 46-9849]. AOSSM Annual Meeting; San Diego, CA; 2011 [Google Scholar]
- 65. Sigmund R. Effect of ultraviolet rays on reaction time in man. Strahlentherapie. 1956;101(4):623-629 [PubMed] [Google Scholar]
- 66. Sørensen OH, Lund B, Saltin B, et al. Myopathy in bone loss of ageing: improvement by treatment with 1 alpha-hydroxycholecalciferol and calcium. Clin Sci (Lond). 1979;56(2):157-161 [DOI] [PubMed] [Google Scholar]
- 67. Tavera-Mendoza LE, White JH. Cell defenses and the sunshine vitamin. Sci Am. 2007;297(5):62-65, 68,-70, 72 [DOI] [PubMed] [Google Scholar]
- 68. Trang HM, Cole DE, Rubin LA, Pierratos A, Siu S, Vieth R. Evidence that vitamin D3 increases serum 25-hydroxyvitamin D more efficiently than does vitamin D2. Am J Clin Nutr. 1998;68(4):854-858 [DOI] [PubMed] [Google Scholar]
- 69. Välimäki VV, Alfthan H, Lehmuskallio E, et al. Vitamin D status as a determinant of peak bone mass in young Finnish men. J Clin Endocrinol Metab. 2004;89(1):76-80 [DOI] [PubMed] [Google Scholar]
- 70. Ward KA, Das G, Berry JL, et al. Vitamin D status and muscle function in post-menarchal adolescent girls. J Clin Endocrinol Metab. 2009;94(2):559-563 [DOI] [PubMed] [Google Scholar]
- 71. Wassner SJ, Li JB, Sperduto A, Norman ME. Vitamin D deficiency, hypocalcemia, and increased skeletal muscle degradation in rats. J Clin Invest. 1983;72(1):102-112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Wicherts IS, van Schoor NM, Boeke AJ, et al. Vitamin D status predicts physical performance and its decline in older persons. J Clin Endocrinol Metab. 2007;92(6):2058-2065 [DOI] [PubMed] [Google Scholar]
- 73. Willis KS. Vitamin D Status and Immune System Biomarkers in Athletes. Laramie, WI: University of Wyoming; 2008:85 [Google Scholar]
- 74. Willis KS, Peterson NJ, Larson-Meyer DE. Should we be concerned about the vitamin D status of athletes? Int J Sport Nutr Exerc Metab. 2008;18(2):204-224 [DOI] [PubMed] [Google Scholar]
- 75. Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr. 2000;72(3):690-693 [DOI] [PubMed] [Google Scholar]
- 76. Yetley EA. Assessing the vitamin D status of the US population. Am J Clin Nutr. 2008;88(2):558S-564S [DOI] [PubMed] [Google Scholar]
- 77. Young A, Edwards RHT, Jones DA, Brenton DP. Quadriceps muscle strength and fibre size during treatment of osteomalacia. In: Stokes IAF, ed. Mechanical Factors and the Skeleton. Vol 12 London, UK: John Libbey, 1981:137-145 [Google Scholar]