

From 2002–2010, the epidemiology of invasive group A streptococcal disease changed dramatically in Utah. The incidence of invasive disease rose from 3.5 to 9.8 cases/100 000 persons, while the incidence of acute rheumatic fever decreased from 6.1 to 3.7 cases/100 000.
Abstract
Background. Invasive group A Streptococcus (GAS) infections are associated with substantial morbidity and mortality. Recent national surveillance data report stable rates of invasive GAS disease, although these may not capture geographic variation.
Methods We performed a population-based, retrospective laboratory surveillance study of invasive GAS disease among Utah residents from 2002–2010. We used Intermountain Healthcare's electronic medical records and data warehouse to identify patients from whom GAS was isolated by culture. We defined clinical syndromes of invasive GAS disease on the basis of International Classification of Diseases, Ninth Revision codes. We abstracted demographic information, comorbidities, and microbiologic and laboratory findings.
Results. From 2002–2010, we identified 1514 cases of invasive GAS disease among Utah residents. The estimated mean annual incidence rate was 6.3 cases/100 000 persons, which was higher than the national rate of 3.6 cases/100 000 (P < .01). The incidence of invasive GAS disease in Utah rose from 3.5 cases/100 000 persons in 2002 to 9.8 cases/100 000 persons in 2010 (P = .01). Among children aged <18 years, the incidence of invasive GAS increased from 3.0 cases/100 000 children in 2002 to 14.1 cases/100 000 children in 2010 (P < .01). The increase in the pediatric population was due, in part, to an increase in GAS pneumonia (P = .047). The rate of invasive GAS disease in adults aged 18–64 years increased from 3.4 cases/100 000 persons in 2002 to 7.6 cases/100 000 persons in 2010 (P = .02). Rates among those aged ≥65 years were stable. The incidence of acute rheumatic fever declined from 6.1 to 3.7 cases/100 000 (P = .04).
Conclusions The epidemiologic characteristics of invasive GAS disease in Utah has changed substantially over the past decade, including a significant increase in the overall incidence of invasive disease—driven primarily by increasing disease in younger persons—that coincided temporally with a decrease in the incidence of acute rheumatic fever.
(See the Editorial Commentary by Kaplan, on pages 488–90.)
Infection by Streptococcus pyogenes (group A streptococci [GAS]) causes a wide range of syndromes ranging from localized illness, such as pharyngitis, to invasive disease, such as bacteremia, pneumonia, necrotizing fasciitis, and streptococcal toxic shock syndrome [1, 2]. Invasive GAS infection causes significant morbidity and mortality in both children and adults [3].
The epidemiologic characteristics of GAS disease are complex. An apparent increase in invasive GAS and streptococcal toxic shock syndrome was reported in the United States during the 1980s and 1990s [4–6]. This was temporally associated with the emergence of M protein (encoded by the emm gene) types 1, 18, and 28 [7–11]. However, more recent sentinel site, population-based surveillance from the Centers for Disease Control and Prevention's (CDC's) Active Bacterial Core surveillance (ABCs) Emerging Infections Program Network reported that the incidence of invasive GAS disease was stable from 1996 through 1999 and from 2002 through 2009 [1, 12].
The incidence of invasive GAS disease and clinical syndromes associated with GAS varies considerably by region and year [1, 13]. During the period of national increases in streptococcal toxic shock syndrome during the 1980s and late 1990s, there were outbreaks of both invasive GAS disease [4] and acute rheumatic fever [14, 15] in Utah and other states in the intermountain west region of the United States. The objective of our population-based study was to describe the incidence, epidemiologic features, and clinical syndromes associated with invasive GAS disease in Utah during a recent 9-year period (2002–2010).
METHODS
Surveillance
This study was approved and granted a waiver of informed consent by the University of Utah and Intermountain Healthcare (Intermountain) institutional review boards.
We performed a retrospective study of case of invasive GAS disease that were reported from January 2002 through December 2010. Cases of invasive GAS disease in Utah were identified using Intermountain's electronic database, the enterprise data warehouse. Intermountain is a large, vertically integrated nonprofit healthcare system that owns and operates 22 hospitals in Utah and other states in the intermountain west (ie, Idaho, Wyoming, Nevada, and Montana). The enterprise data warehouse is an electronic repository of clinical, financial, laboratory, and microbiologic records of all hospital encounters at Intermountain facilities. Over the study period, Intermountain's market share of statewide hospital admissions was approximately 70%, ranging from 75% to 85% among Utah children and 55% to 60% among adults (data kindly provide by Jim Bradshaw, Director of Strategic Planning, Intermountain Healthcare, Salt Lake City, UT).
A case of invasive GAS was defined as a Utah resident in whom GAS was isolated in culture from a usually sterile site (ie, blood, abscess, cerebrospinal fluid, joint fluid, pleural fluid, or peritoneal fluid) [1]. We excluded any patient who had S. pyogenes detected by polymerase chain reaction (PCR) alone. Patients who had GAS isolated from nonsterile sites and an International Classification of Diseases, Ninth Revision (ICD-9) diagnosis of streptococcal toxic shock syndrome, necrotizing fasciitis, or puerperal sepsis were included. Cases of acute rheumatic fever were identified using ICD-9 discharge codes (390–392). Case-fatality rates were calculated on the basis of the proportion of patients dying before hospital discharge.
In addition to microbiologic data, patient demographic characteristics, clinical syndromes, and underlying comorbidities were abstracted from the enterprise data warehouse. Comorbidities were classified according to an algorithm of chronic medical conditions, developed by Feudtner et al [16] for pediatric subjects, or the Elixhauser comorbidity index, developed by Elixhauser et al [17] for adults, both of which use ICD-9 coding at hospital discharge to identify comorbidities (Supplementary Table 1).
Definition of Clinical Syndromes
We used the definition of invasive GAS clinical syndromes reported by O'Brien et al [13]. Clinical syndromes were classified according to ICD-9 discharge codes recorded anywhere in the list of discharge diagnoses (Supplementary Table 2). Patients who had GAS bacteremia but no other clinical syndrome were classified as having only isolated bacteremia; all other patients could have >1 syndrome. Patients with skin and soft tissue infections included those with cellulitis, abscess, infected ulcers, erisipelas, wound infection, lymphangitis, and lymphadenitis with isolation of GAS from a normally sterile site but excluded those with necrotizing fasciitis, which was classified separately. Patients with pneumonia included those with uncomplicated bacteremic pneumonia and complicated pneumonia, defined as pneumonia with parapneumonic effusion, empyema, or lung abscess.
Statistical Analysis
We calculated overall and age-specific rates of invasive GAS disease, using annual intercensus population estimates for Utah, which are reported per 100 000 persons per year. We present unadjusted incidence estimates, which do not incorporate adjustments for Intermountain's market share of statewide hospital admissions. Categorical variables were compared using the χ2 test or the Fisher exact test, as appropriate. An extension of the Wilcoxon rank-sum test was performed to assess for a trend in proportions across calendar years and age groups. All statistical analyses were performed using Stata 11.2 (StataCorp, College Station, TX).
RESULTS
Descriptive Epidemiology and Disease Incidence
From January of 2002 through December of 2010, we identified 1514 patients meeting the case definition of invasive GAS disease. A total of 568 patients (38%) were <18 years of age, 761 (50%) were aged 18–64 years, and 185 (12%) were >65 years (Table 1). The mean age was 31 years (range, 0–97 years). Compared with the Utah population, patients with invasive GAS disease were more likely to be Native Hawaiian/Pacific Islander (3.3% vs 1.2%; P < .001) and less likely to be white (76% vs 86%; P < .001). Invasive GAS disease showed a winter seasonal peak from December through March.
Table 1.
Patient Demographic and Clinical Characteristics of 1514 Patients With Invasive Group A Streptococcal Infection, Utah, 2002–2010
| Parameter | Patients, No. (%) |
|---|---|
| Year of isolation | |
| 2002 | 83 (5.5) |
| 2003 | 138 (9.1) |
| 2004 | 116 (7.7) |
| 2005 | 132 (8.7) |
| 2006 | 177 (11.7) |
| 2007 | 200 (13.2) |
| 2008 | 175 (11.6) |
| 2009 | 215 (14.2) |
| 2010 | 278 (18.4) |
| Patient age, years | |
| <5 | 258 (17.0) |
| 5–17 | 310 (20.5) |
| 18–34 | 322 (21.3) |
| 35–49 | 270 (17.8) |
| 50–64 | 169 (11.2) |
| ≥65 | 185 (12.2) |
| Sex | |
| Male | 715 (53.2) |
| Race | |
| American Indian/Alaskan Native | 21 (1.6) |
| Asian | 15 (1.1) |
| Black | 24 (1.8) |
| Native Hawaiian/Pacific Islander | 43 (3.2) |
| White | 1013 (75.7) |
| Other | 8 (0.6) |
| Unknown | 32 (2.4) |
| Ethnicity | |
| Hispanic | 182 (13.6) |
| Source of isolate | |
| Totala | 1982 (100.0) |
| Abscess | 676 (34.1) |
| Blood alone | 415 (20.9) |
| Other invasive site | 230 (11.6) |
| Nonsterile siteb | 188 (9.5) |
| Wound specimens | 147 (7.4) |
| Peritoneal fluid | 126 (6.4) |
| Surgical specimens (eg, tissue) | 80 (4.0) |
| Pleural fluid | 74 (3.7) |
| Joint fluid | 26 (1.3) |
| Cerebrospinal fluid | 12 (0.6) |
| Bone | 7 (0.4) |
| Pericardial fluid | 1 (0.1) |
aA total of 415 patients had specimens from ≥2 sites that grew group A streptococci (GAS) on culture.
bIsolation from a nonsterile site was considered invasive GAS disease if accompanied by an ICD-9-coded diagnosis of streptococcal toxic shock syndrome, necrotizing fasciitis, or puerperal sepsis.
Over the 9-year period, the mean annual incidence of invasive GAS disease was 6.3 cases/100 000 persons. The incidence increased significantly, from 3.5 cases/100 000 persons in 2002 to 9.8 cases/100 000 persons in 2010 (P = .01). During the study period, the incidence of acute rheumatic fever decreased from 6.1 cases/100 000 persons in 2002 to 3.7 cases/100 000 persons in 2010 (P = .04) (Figure 1A).
Figure 1.
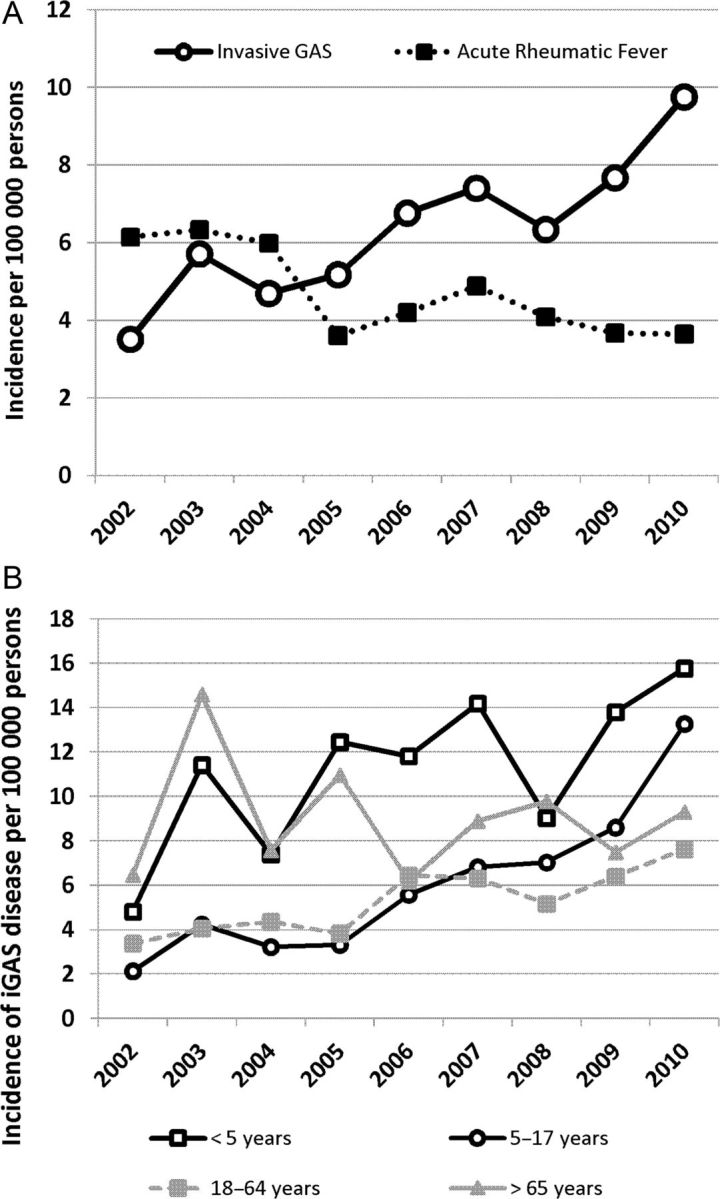
A, Incidence of invasive group A streptococcal (GAS) disease and acute rheumatic fever in Utah, 2002–2010. B, Incidence of invasive GAS disease in Utah, 2002–2010, by age.
The mean annual incidence was highest among children aged <5 years (11.2 cases/100 000 children) and individuals aged ≥65 years (9.0 cases/100 000 persons) and was lowest among individuals aged 18–64 years (5.3 cases/100 000 persons) (Figure 2). Among children <18 years old, the incidence of invasive GAS disease increased from 3.0 cases/100 000 children in 2002 to 14.1 cases/100 000 children in 2010 (P < .01). The incidence of invasive GAS disease also increased among adults aged 18–64 years, from 3.8 to 7.9 cases/100 000 persons in 2002 and 2010, respectively (P = .02). Rates were stable among adults aged >65 years. (Figure 1B)
Figure 2.

Incidence of invasive group A streptococcal infection, incidence of intensive care unit admission, and case-fatality rate (calculated as the proportion of patients with group A streptococci who died before hospital discharge), by age, 2002–2010. Abbreviation: ICU, intensive care unit.
Clinical Syndromes
Of the 1514 patients with invasive GAS disease, 674 (45%) had a blood culture performed. Of these, 415 (62%) were culture positive. A total of 135 (33%) had primary bacteremia; the remainder had bacteremia in conjunction with another clinical syndrome. Other sources of GAS isolates are shown in Table 1.
The most common clinical syndromes among adults and children were skin and soft tissue infection (70%), pneumonia (10%), and primary bacteremia without focus (9%) (Table 2). Pregnancy-related invasive GAS disease accounted for 3% of cases.
Table 2.
Clinical Syndromes of Patients With Invasive Group A Streptococcal Disease, Utah, 2002–2010
| Clinical Syndromea | <5 Years (n = 258) | 5–17 Years (n = 310) | 18–34 Years (n = 322) | 35–49 Years (n = 270) | 50–64 Years (n = 169) | ≥65 Years (n = 185) | Overall (n = 1514) |
|---|---|---|---|---|---|---|---|
| Skin and soft tissue infection | |||||||
| No. (%) of case patients | 175 (67.8) | 239 (77.1) | 232 (72.1) | 186 (68.9) | 108 (63.9) | 125 (67.6) | 1065 (70.3) |
| No. of deaths (CFR) | 0 (0.0) | 0 (0.0) | 2 (1.0) | 1 (0.6) | 1 (1.0) | 16 (13.3) | 20 (2.1) |
| Pneumonia | |||||||
| No. (%) of case patients | 35 (13.6) | 21 (6.8) | 21 (6.5) | 26 (9.6) | 21 (12.4) | 31 (16.8) | 155 (10.2) |
| No. of deaths (CFR) | 1 (2.9) | 2 (10.5) | 1 (5.3) | 2 (8.3) | 3 (16.7) | 7 (22.6) | 16 (11.0) |
| Primary bacteremia (no other site of infection) | |||||||
| No. (%) of case patients | 35 (13.6) | 21 (6.8) | 12 (3.7) | 30 (11.1) | 19 (11.2) | 22 (11.9) | 139 (9.2) |
| No. of deaths (CFR) | 0 (0.0) | 0 (0.0) | 1 (11.1) | 2 (8.0) | 2 (13.3) | 4 (26.7) | 9 (7.6) |
| Abdominal/peritoneal | |||||||
| No. (%) of case patients | 15 (5.8) | 24 (7.7) | 25 (7.8) | 38 (14.1) | 25 (14.8) | 11 (6.0) | 138 (9.1) |
| No. of deaths (CFR) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (6.3) | 0 (0.0) | 2 (25.0) | 4 (3.5) |
| Septic arthritis | |||||||
| No. (%) of case patients | 5 (1.9) | 18 (5.8) | 10 (3.1) | 15 (5.6) | 14 (8.3) | 15 (8.1) | 77 (5.1) |
| No. of deaths (CFR) | 0 (0.0) | 1 (5.6) | 1 (10.0) | 0 (0.0) | 1 (7.1) | 4 (26.7) | 7 (9.1) |
| Necrotizing fasciitis | |||||||
| No. (%) of case patients | 1 (0.4) | 6 (1.9) | 10 (3.1) | 19 (7.0) | 12 (7.1) | 13 (7.0) | 61 (4.0) |
| No. of deaths (CFR) | 0 (0.0) | 1 (16.7) | 1 (10.0) | 0 (0.0) | 1 (8.3) | 5 (38.5) | 8 (13.1) |
| Streptococcal toxic shock syndrome | |||||||
| No. (%) of case patients | 5 (1.9) | 5 (1.6) | 13 (4.0) | 10 (3.6) | 10 (5.9) | 10 (5.4) | 53 (3.5) |
| No. of deaths (CFR) | 1 (20.0) | 0 (0.0) | 1 (7.7) | 3 (30.0) | 1 (10.0) | 4 (40.0) | 10 (18.9) |
| Pregnancy-related (eg, puerperal sepsis) | |||||||
| No. (%) of case patients | 0 (0.0) | 0 (0.0) | 41 (12.7) | 7 (2.6) | 0 (0.0) | 0 (0.0) | 48 (3.2) |
| No. of deaths (CFR) | 0 (0.0) | 0 (0.0) | 1 (2.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.1) |
| Osteomyelitis | |||||||
| No. (%) of case patients | 8 (3.1) | 11 (3.6) | 6 (1.9) | 6 (2.2) | 6 (3.6) | 2 (1.1) | 39 (2.6) |
| No. of deaths (CFR) | 0 (0.0) | 0 (0.0) | 1 (16.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.6) |
| Endocarditis/pericarditis | |||||||
| No. (%) of case patients | 2 (0.8) | 2 (0.7) | 3 (0.9) | 5 (1.9) | 3 (1.8) | 13 (7.0) | 28 (1.9) |
| No. of deaths (CFR) | 0 (0.0) | 1 (50.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (15.4) | 3 (10.7) |
| Meningitis | |||||||
| No. (%) of case patients | 4 (1.6) | 4 (1.3) | 0 (0.0) | 1 (0.4) | 3 (1.8) | 3 (1.6) | 15 (1.0) |
| No. of deaths (CFR) | 0 (0.0) | 1 (25.0) | 0 (0.0) | 0 (0.0) | 1 (33.3) | 2 (66.7) | 4 (26.7) |
Case-fatality rates are calculated as the proportion of case patients who died before hospital discharge.
Abbreviation: CFR, case-fatality rate.
aPatients may appear in more than one category with the exception of primary bacteremia.
The distribution of invasive GAS clinical syndromes varied by age (Table 2). Skin and soft tissue infection (excluding necrotizing fasciitis), the most common clinical syndrome among all age groups, was present in 70% of subjects. Pneumonia was present in 10% of case patients overall, in 14% of children aged <5 years, and in 17% of adults aged >65 years.
Fifty-three patients (4%) developed streptococcal toxic shock syndrome. The median age of patients with toxic shock syndrome (30 years) was not different from the median age of those with other clinical syndromes (29 years) (P = .5). Persons with streptococcal toxic shock syndrome were more likely to have underlying medical conditions (81%) than those with other invasive infections (35%) (P < .001). Among adults, these included heart disease (58% vs 18%; P < .001), liver disease (45% vs 12%; P < .001), depression (21% vs 9%; P = .01), diabetes (19% vs 10%; P = .04), kidney disease (13% vs 5%; P = .01), alcohol abuse (9% vs 2%; P < .001), and drug abuse (13% vs 5%; P = .02). Children with toxic shock syndrome were more likely to have metabolic disorders (4% vs 0.4%; P = .02). Additionally, patients with toxic shock syndrome were more likely than those with other invasive infections to have bacteremia (53% vs 29%; P < .001). Of the 53 patients who developed streptococcal toxic shock, 17 (32%) also had necrotizing fasciitis.
The mean overall and age-specific incidence rates of invasive GAS-associated clinical syndromes over the study period are shown in Table 3. From 2002 through 2010, the incidence of skin and soft tissue infections increased from 2.4 to 7.3 cases/100 000 persons (P = .01), and the incidence of pneumonia increased from 0.1 to 1.2 cases/100 000 persons (P = .048). Among children, the rate of GAS pneumonia increased from 0.0 and 0.8 cases/100 000 persons in 2002 and 2003, respectively, to 2.2 cases/100 000 persons in 2010 (P = .047). Rates of streptococcal toxic shock syndrome and necrotizing fasciitis remained stable.
Table 3.
Mean Age-Specific and Overall Incidence of Invasive Group A Streptococcus Clinical Syndromes, Utah, 2002–2010
| Clinical Syndrome | <5 Years | 5–17 Years | 18–34 Years | 35–49 Years | 50–64 Years | ≥65 Years | Overall |
|---|---|---|---|---|---|---|---|
| All invasive GAS disease | 11.2 | 6.0 | 4.7 | 6.2 | 5.3 | 9.0 | 6.3 |
| Skin and soft tissue infection | 7.6 | 4.6 | 3.4 | 4.3 | 3.4 | 6.1 | 4.4 |
| Pneumonia | 1.5 | 0.5 | 0.3 | 0.6 | 0.7 | 1.5 | 0.6 |
| Abdominal/peritoneal | 0.7 | 0.5 | 0.4 | 0.9 | 0.8 | 0.5 | 0.6 |
| Primary bacteremia (no other site of infection) | 1.6 | 0.4 | 0.2 | 0.7 | 0.6 | 1.1 | 0.6 |
| Necrotizing fasciitis | 0.0 | 0.1 | 0.1 | 0.4 | 0.4 | 0.7 | 0.3 |
| Septic arthritis | 0.2 | 0.4 | 0.1 | 0.3 | 0.5 | 0.8 | 0.3 |
| Streptococcal toxic shock syndrome | 0.2 | 0.1 | 0.2 | 0.2 | 0.3 | 0.5 | 0.2 |
| Osteomyelitis | 0.4 | 0.2 | 0.1 | 0.1 | 0.2 | 0.1 | 0.2 |
| Pregnancy-related (eg, puerperal sepsis) | 0.0 | 0.0 | 0.6 | 0.2 | 0.0 | 0.0 | 0.2 |
| Meningitis | 0.2 | 0.1 | 0.0 | 0.0 | 0.1 | 0.1 | 0.1 |
| Endocarditis/pericarditis | 0.1 | 0.0 | 0.0 | 0.1 | 0.1 | 0.6 | 0.1 |
Data are no. of cases per 100 000 persons per year.
Underlying Disease
Underlying comorbidities were present in 51% of adults and 11% of children (P < .001). The most frequently reported comorbidities among adults were hypertension (29%); liver disease (21%); heart disease (20%), including atherosclerotic cardiovascular disease and heart failure; pulmonary disease (14%); and diabetes (10%). In children, the most common underlying conditions included heart disease (6%), neuromuscular disorders (3%), congenital and genetic anomalies (3%), and pulmonary disease (2%).
Intensive Care Unit Admission and Death
Overall, 285 patients (19%) with invasive GAS disease were admitted to an intensive care unit (ICU). Skin and soft tissue infections accounted for 46% of ICU admissions, followed by pneumonia (29%), streptococcal toxic shock syndrome (16%), and necrotizing fasciitis (15%). Fifty-three patients (4%) with invasive GAS disease died.
The proportion of patients admitted to an ICU was stable over the study period. The overall incidence of GAS disease, the incidence of ICU admission, and overall case-fatality rates varied by age group (Figure 2). The incidence of invasive GAS disease was highest among children aged <5 years and adults aged >65 years, and the case-fatality rate increased with age.
The proportion of patients admitted to ICU, by age and clinical syndrome, are shown in Table 4. ICU admission was more common among adults >18 years of age (23% vs 13%; P < .001). Similarly, underlying medical conditions were more common among adults requiring intensive care (P < .001). Skin and soft tissue infections accounted for 52% of ICU admissions among adults and 27% among children (P < .001). Conversely, pneumonia accounted for 44% of ICU admissions among children, compared with 24% among adults (P = .001).
Table 4.
Clinical Syndromes Among Intensive Care Unit Patients With Invasive Group A Streptococcal Disease, Utah, 2002–2010, by Age
| Patients, No. (%) |
|||
|---|---|---|---|
| Clinical Syndromea | <18 Years (n = 71) | ≥18 Years (n = 214) | P |
| Skin and soft tissue infection | 19 (26.8) | 112 (52.3) | <.001 |
| Pneumonia | 31 (43.7) | 51 (23.8) | .001 |
| Streptococcal toxic shock syndrome | 10 (14.1) | 36 (16.8) | .587 |
| Necrotizing fasciitis | 6 (8.5) | 36 (16.8) | .085 |
| Primary bacteremia (no other site of infection) | 10 (14.0) | 22 (10.3) | .379 |
| Abdominal/peritoneal | 8 (11.3) | 23 (10.8) | .903 |
| Septic arthritis | 3 (4.2) | 18 (8.4) | .242 |
| Pregnancy-related (eg, puerperal sepsis) | 0 (0.0) | 16 (7.5) | .018 |
| Osteomyelitis | 4 (5.6) | 7 (3.3) | .370 |
| Endocarditis/pericarditis | 3 (4.2) | 11 (5.1) | .757 |
| Meningitis | 3 (4.2) | 4 (1.9) | .266 |
| Underlying medical condition | 20 (28.2) | 192 (89.7) | <.001 |
aPatients may appear in more than one category with the exception of primary bacteremia.
Among adults, 6% of patients with invasive GAS disease died, compared with 1% of children (P < .001). Case-fatality rates varied by clinical syndrome, with the highest rates among patients with meningitis (27%) and streptococcal toxic shock syndrome (19%).
DISCUSSION
In this 9-year study of laboratory-confirmed invasive GAS disease, we observed an average of 168 cases and 6 deaths each year in Utah from 2002 through 2010. The mean annual incidence of invasive GAS disease was 6.3 cases/100 000 persons during the study period and increased from 3.5 cases/100 000 persons in 2002 to 9.8 cases/100 000 persons in 2010. The burden of disease was highest among children aged <5 years and persons aged >65 years. Pneumonia emerged as a prominent clinical syndrome and was associated with 44% of ICU admissions among children <18 years old. The incidence of skin and soft tissue infection also increased, from 2.4 cases/100 000 persons in 2002 to 7.3 cases/100 000 persons in 2010, because of increasing disease among younger persons.
GAS infection continues to cause significant morbidity and mortality in Utah, as well as in the United States, Europe, and countries in other areas [1, 18–22]. In a population-based study that used data from the CDC's ABCs network, O'Brien et al. estimated the incidence of invasive GAS disease as 3.5 cases/100 000 persons between 1995 and 1999 [13]. In a follow up study, O'Loughlin et al. used similar sentinel site population-based surveillance methods and reported an identical mean incidence of 3.5 cases/100 000 persons from 2000 to 2004 [1]. However, the incidence varied by site, from 2.0 to 5.9 cases/100 000 persons. Other studies from North America (Canada), Europe (the Netherlands), and Australasia (New Zealand) reported invasive GAS disease incidence rates ranging from 1.5 to 8.1 cases/100 000 persons [18, 19, 21]. In our study, the mean incidence of invasive GAS disease was 6.3 cases/100 000 persons from 2002 through 2010—higher than the national average but within the range reported for other sites [1, 13].
The incidence of invasive GAS disease in Utah increased throughout the study period and was primarily attributable to rising rates of skin and soft tissue infection (eg, cellulitis/abscess) and pneumonia, largely among children <18 years of age. While increases in the incidence of invasive GAS disease were reported in the United States in the 1980s and 1990s [2, 4, 6], recent data from ABCs sites in the United States do not demonstrate a consistent trend [13]. Local variation has long been recognized and is thought to reflect periodic changes in the prevalence of specific emm types [9, 23]. Coincident with the emergence of M-type 1 streptococci, Martin et al. reported that GAS isolates from sterile-site specimens increased from <1% during 1980–1986 to 6% in 1988–1989 and 8% in 1990 [24]. We did not systematically type strains of GAS in this study, but from 2002 through 2004, isolates from Primary Children's Medical Center were emm typed as part of a different study. Among 63 isolates from children with invasive disease, the most common emm types were 1 (19%), 12 (17%), 3 (13%), and 118 (11%) (kindly provided by Nancy Augustine, senior laboratory specialist, Division of Clinical Pathology, University of Utah Health Sciences Center, personal communication). In contrast, O'Brien et al. reported that the incidence of invasive disease in Georgia fell from 5.2 cases/100 000 persons in 1994–1995 to 2.2 cases/100 000 persons in 1995–1999, demonstrating that variations in the incidence of invasive GAS disease can occur over relatively short periods [13]. Cyclic increases in the incidence of invasive GAS disease have been described previously in Utah and Sweden [25, 26].
Although the primary aim of this study was to explore invasive GAS disease, we also evaluated the incidence of acute rheumatic fever in Utah. In 1985 and 1998, there were 2 resurgences of acute rheumatic fever in Utah that were temporally associated with mucoid strains of GAS, predominantly M-type 18 [25]. During the period described in this study, the incidence of acute rheumatic fever declined, while the incidence of invasive GAS disease increased. This suggests that the prevalence of rheumatogenic strains of GAS may have decreased during the study period, while the prevalence of invasive strains may have increased.
Several risk factors have been associated with invasive GAS disease. These include the presence of children living in the home, the number of persons in the home, new use of nonsteroidal anti-inflammatory drugs in children aged <18 years, exposure to >1 child with a sore throat, human immunodeficiency virus infection, history of injection drug use in adults 18–44 years, and certain medical conditions (diabetes, heart disease, and cancer) in adults ≥45 years of age [27, 28]. Utah's population is the youngest in the United States: 31% of the population is <18 years of age, compared with 24% nationally [29, 30]. Among all US states, Utah has the highest rate of household crowding and the greatest number of households with children [31, 32]. Furthermore, Utah's elementary and secondary schools have the largest classroom size [33]. Together, the crowded conditions in school and at home may contribute to increased transmission of GAS among children and their parents, caretakers, grandparents, and extended family members and may partially explain the unusual epidemiologic characteristics of GAS disease in Utah.
The increase in the incidence of invasive GAS disease is unlikely to be explained by changes in diagnostic methods or practices. Cases were included on the basis of traditional microbiologic criteria, and newer molecular techniques were not used. Skin and soft tissue infections attributed to GAS increased over time, perhaps reflecting a heightened awareness among clinicians of methicillin-resistant Staphylococcus aureus in the community that led to increased diagnostic testing. However, the proportion admitted to the ICU and the case-fatality rates remained stable, arguing against increased detection of milder cases.
Clinical syndromes associated with invasive GAS disease in the United States vary from year to year. From 1997 through 1999, bacteremia without focus, cellulitis, and septic arthritis were reported as the most common invasive GAS–associated clinical syndromes in both children and adults [27, 28]. During 2000–2004, skin and soft tissue infections, followed by bacteremia without focus and pneumonia, were the most common clinical syndromes among adults and children [1]. A similar distribution was reported in a study of adults with invasive GAS disease admitted to an ICU in 2002 [34]. In our study, skin and soft tissue infection, pneumonia, and bacteremia without focus were the most common clinical presentations associated with invasive GAS disease. Although the clinical syndromes seen in Utah were similar to other descriptions, the case-fatality rate of 4% in our study was lower than that reported elsewhere [1, 19]. One explanation may be that most of our patients (76%) were <50 years old, and the case-fatality rate in this group is low. The observed case-fatality rate among persons aged >65 years in our cohort (17%) is similar to the rate observed among older persons in the ABCs studies [1, 13].
In our study, pneumonia was present in 10% of patients, with higher rates among children <5 years old and adults >65 years old. In a study of 2611 cases of invasive GAS disease in the United Kingdom in 2003–2004, pneumonia was diagnosed in 309 patients (12%) [35]. From 2002 through 2010, the incidence of GAS pneumonia increased substantially among children aged <18 years. In a network study conducted at 8 academic medical centers in Canada, GAS was the second most frequently isolated organism by culture among children with complicated pneumonia from 2000 through 2003 [36]. In a separate study, in which we examined pleural fluid by culture and PCR in children with complicated pneumonia during 2009, 5% had S. pyogenes detected by culture, and 11% had S. pyogenes detected by PCR, suggesting an increased frequency of invasive GAS pneumonia [37]. Further studies are needed to determine the emm types responsible for the increasing burden of GAS pneumonia among children.
Our study has a number of limitations. Clinical syndromes were classified using ICD-9 discharge codes rather than medical record abstraction. This may lead to misclassification, potentially incorrectly ascribing clinical syndromes. Cases of invasive GAS disease diagnosed at non-Intermountain facilities were not included in our surveillance system, and thus our results likely underestimate the true incidence of invasive GAS disease among Utah residents. Patients hospitalized at Intermountain hospitals were generally similar to the population of all patients hospitalized in Utah, but there may be unmeasured characteristics that impact invasive GAS disease. We were unable to emm type a collection of longitudinally archived invasive GAS isolates. Last, our study was based in a single geographic region that has previously reported high rates of rheumatic fever, and thus our findings may not be generalizable [25].
In conclusion, rates of invasive GAS disease are higher in Utah than in other surveillance sites. The incidence of invasive GAS disease increased primarily among younger people and was associated with increases in skin and soft tissue infections and pneumonia, while the incidence of acute rheumatic fever decreased. Continued surveillance, including performance of emm typing, may lead to a better understanding of the complex epidemiologic characteristics of invasive GAS disease and aid in the development of prevention strategies.
Supplementary Data
Supplementary materials are available at Clinical Infectious Diseases online (http://cid.oxfordjournals.org). Supplementary materials consist of data provided by the author that are published to benefit the reader. The posted materials are not copyedited. The contents of all supplementary data are the sole responsibility of the authors. Questions or messages regarding errors should be addressed to the author.
Notes
Acknowledgments. We thank Dr Lloyd Tani for providing data on the incidence of acute rheumatic fever in Utah.
Financial support. This work was supported by grants from the National Institute of Allergy and Infectious Diseases (U01A1082482 to K. A. and C. L. B.; U01 AI074419-01 to C. L. B., A. J. B., and A. T. P.; U01AI082184-01 to A. T. P. and A. J. B.; and 1K23-AI079401-01A1 to A. J. B.), the National Institute of Child Health and Human Development (K-24 HD047249-01A1 to C. L. B.), and the CDC (U18-IP000303-01 to C. S., K. A., C. L. B., A. T. P., and A. J. B.). This project was further supported by the University of Utah, Department of Pediatrics, through the Children's Health Research Center, and by the Pediatric Clinical and Translational Research Scholars Program, the H. A. and Edna Benning Presidential Endowment, and the Primary Children's Medical Center Foundation.
Potential conflicts of interest. All authors: No reported conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
References
- 1.O'Loughlin RE, Roberson A, Cieslak PR, et al. The epidemiology of invasive group A streptococcal infection and potential vaccine implications: United States, 2000–2004. Clin Infect Dis. 2007;45:853–62. doi: 10.1086/521264. [DOI] [PubMed] [Google Scholar]
- 2.Kaplan EL. The resurgence of group A streptococcal infections and their sequelae. Eur J Clin Microbiol Infect Dis. 1991;10:55–7. doi: 10.1007/BF01964407. [DOI] [PubMed] [Google Scholar]
- 3.Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis. 2005;5:685–94. doi: 10.1016/S1473-3099(05)70267-X. [DOI] [PubMed] [Google Scholar]
- 4.Wheeler MC, Roe MH, Kaplan EL, Schlievert PM, Todd JK. Outbreak of group A Streptococcus septicemia in children. Clinical, epidemiologic, and microbiological correlates. JAMA. 1991;266:533–7. [PubMed] [Google Scholar]
- 5.Givner LB, Abramson JS, Wasilauskas B. Apparent increase in the incidence of invasive group A beta-hemolytic streptococcal disease in children. J Pediatr. 1991;118:341–6. doi: 10.1016/s0022-3476(05)82144-4. [DOI] [PubMed] [Google Scholar]
- 6.Hoge CW, Schwartz B, Talkington DF, Breiman RF, MacNeill EM, Englender SJ. The changing epidemiology of invasive group A streptococcal infections and the emergence of streptococcal toxic shock-like syndrome. A retrospective population-based study. JAMA. 1993;269:384–9. [PubMed] [Google Scholar]
- 7.Stevens DL, Tanner MH, Winship J, et al. Severe group A streptococcal infections associated with a toxic shock-like syndrome and scarlet fever toxin A. N Engl J Med. 1989;321:1–7. doi: 10.1056/NEJM198907063210101. [DOI] [PubMed] [Google Scholar]
- 8.Schwartz B, Elliott JA, Butler JC, et al. Clusters of invasive group A streptococcal infections in family, hospital, and nursing home settings. Clin Infect Dis. 1992;15:277–84. doi: 10.1093/clinids/15.2.277. [DOI] [PubMed] [Google Scholar]
- 9.Johnson DR, Stevens DL, Kaplan EL. Epidemiologic analysis of group A streptococcal serotypes associated with severe systemic infections, rheumatic fever, or uncomplicated pharyngitis. J Infect Dis. 1992;166:374–82. doi: 10.1093/infdis/166.2.374. [DOI] [PubMed] [Google Scholar]
- 10.Gaworzewska E, Colman G. Changes in the pattern of infection caused by Streptococcus pyogenes. Epidemiol Infect. 1988;100:257–69. doi: 10.1017/s095026880006739x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Green NM, Zhang S, Porcella SF, et al. Genome sequence of a serotype M28 strain of group a streptococcus: potential new insights into puerperal sepsis and bacterial disease specificity. J Infect Dis. 2005;192:760–70. doi: 10.1086/430618. [DOI] [PubMed] [Google Scholar]
- 12.Centers for Disease Control and Prevention. Active Bacterial Core Surveillance Report, Emerging Infections Program Network, group A Streptococcus, 2009. 2010 [Google Scholar]
- 13.O'Brien KL, Beall B, Barrett NL, et al. Epidemiology of invasive group a streptococcus disease in the United States, 1995–1999. Clin Infect Dis. 2002;35:268–76. doi: 10.1086/341409. [DOI] [PubMed] [Google Scholar]
- 14.Veasy LG, Wiedmeier SE, Orsmond GS, et al. Resurgence of acute rheumatic fever in the intermountain area of the United States. N Engl J Med. 1987;316:421–7. doi: 10.1056/NEJM198702193160801. [DOI] [PubMed] [Google Scholar]
- 15.Veasy LG, Tani LY, Hill HR. Persistence of acute rheumatic fever in the intermountain area of the United States. J Pediatr. 1994;124:9–16. doi: 10.1016/s0022-3476(94)70247-0. [DOI] [PubMed] [Google Scholar]
- 16.Feudtner C, Silveira MJ, Christakis DA. Where do children with complex chronic conditions die? Patterns in Washington State, 1980–1998. Pediatrics. 2002;109:656–60. doi: 10.1542/peds.109.4.656. [DOI] [PubMed] [Google Scholar]
- 17.Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27. doi: 10.1097/00005650-199801000-00004. [DOI] [PubMed] [Google Scholar]
- 18.Safar A, Lennon D, Stewart J, et al. Invasive group A streptococcal infection and vaccine implications, Auckland, New Zealand, 2005–2006. Emerg Infect Dis. 2011;17:983–9. doi: 10.3201/eid1706.100804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Davies HD, McGeer A, Schwartz B, et al. Invasive group A streptococcal infections in Ontario, Canada. Ontario Group A Streptococcal Study Group. N Engl J Med. 1996;335:547–54. doi: 10.1056/NEJM199608223350803. [DOI] [PubMed] [Google Scholar]
- 20.Lamagni TL, Efstratiou A, Vuopio-Varkila J, Jasir A, Schalen C. The epidemiology of severe Streptococcus pyogenes associated disease in Europe. Euro Surveill. 2005;10:179–84. [PubMed] [Google Scholar]
- 21.Vlaminckx BJ, van Pelt W, Schouls LM, et al. Long-term surveillance of invasive group A streptococcal disease in The Netherlands, 1994–2003. Clin Microbiol Infect. 2005;11:226–31. doi: 10.1111/j.1469-0691.2004.01068.x. [DOI] [PubMed] [Google Scholar]
- 22.Lepoutre A, Doloy A, Bidet P, et al. Epidemiology of invasive Streptococcus pyogenes infections in France in 2007. J Clin Microbiol. 2011;49:4094–100. doi: 10.1128/JCM.00070-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Schwartz B, Facklam RR, Breiman RF. Changing epidemiology of group A streptococcal infection in the USA. Lancet. 1990;336:1167–71. doi: 10.1016/0140-6736(90)92777-f. [DOI] [PubMed] [Google Scholar]
- 24.Martin DR, Single LA. Molecular epidemiology of group A streptococcus M type 1 infections. J Infect Dis. 1993;167:1112–7. doi: 10.1093/infdis/167.5.1112. [DOI] [PubMed] [Google Scholar]
- 25.Veasy LG, Tani LY, Daly JA, et al. Temporal association of the appearance of mucoid strains of Streptococcus pyogenes with a continuing high incidence of rheumatic fever in Utah. Pediatrics. 2004;113(3 Pt 1):e168–72. doi: 10.1542/peds.113.3.e168. [DOI] [PubMed] [Google Scholar]
- 26.Eriksson BK, Andersson J, Holm SE, Norgren M. Epidemiological and clinical aspects of invasive group A streptococcal infections and the streptococcal toxic shock syndrome. Clin Infect Dis. 1998;27:1428–36. doi: 10.1086/515012. [DOI] [PubMed] [Google Scholar]
- 27.Factor SH, Levine OS, Schwartz B, et al. Invasive group A streptococcal disease: risk factors for adults. Emerg Infect Dis. 2003;9:970–7. doi: 10.3201/eid0908.020745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Factor SH, Levine OS, Harrison LH, et al. Risk factors for pediatric invasive group A streptococcal disease. Emerg Infect Dis. 2005;11:1062–6. doi: 10.3201/eid1107.040900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.US Census Bureau. 2010 census summary file 1 Utah: Prepared by the US Census Bureau. 2011 [Google Scholar]
- 30.US Census Bureau, Population Division. Table 1. Preliminary annual estimates of the resident population for the United States, regions, states, and Puerto Rice: April 1, 2000 to July 1, 2010 (NST-PEST2010-01). US Census Bureau, Population Division. 2011 [Google Scholar]
- 31.Haddad MB, Porucznik CA, Joyce KE, et al. Risk factors for pediatric invasive pneumococcal disease in the Intermountain West, 1996–2002. Ann Epidemiol. 2008;18:139–46. doi: 10.1016/j.annepidem.2007.09.006. [DOI] [PubMed] [Google Scholar]
- 32.U.S. Census Bureau. 2010 Census Summary File 1. Available at: http://www.census.gov/prod/cen2010/briefs/c2010br-03.pdf. Accessed 18 June 2011. [Google Scholar]
- 33.U.S. Department of Education, National Center for Education Statistics. State nonfiscal survey of public elementary/secondary education, 2000–01 through 2006–07. Available at: http://nces.ed.gov/programs/digest/d08/tables/dt08_066.asp. Accessed 14 June 2011. [Google Scholar]
- 34.Mulla ZD. Invasive group A streptococcal disease and intensive care unit admissions. Intensive Care Med. 2002;28:1822–4. doi: 10.1007/s00134-002-1538-5. [DOI] [PubMed] [Google Scholar]
- 35.Lamagni TL, Neal S, Keshishian C, et al. Severe Streptococcus pyogenes infections, United Kingdom, 2003–2004. Emerg Infect Dis. 2008;14:202–9. doi: 10.3201/eid1402.070888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Langley JM, Kellner JD, Solomon N, et al. Empyema associated with community-acquired pneumonia: a Pediatric Investigator's Collaborative Network on Infections in Canada (PICNIC) study. BMC Infect Dis. 2008;8:129. doi: 10.1186/1471-2334-8-129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Blaschke AJ, Heyrend C, Byington CL, et al. Molecular analysis improves pathogen identification and epidemiologic study of pediatric parapneumonic empyema. Pediatr Infect Dis J. 2011;30:289–94. doi: 10.1097/INF.0b013e3182002d14. [DOI] [PMC free article] [PubMed] [Google Scholar]