

Abstract
Background
The patient handoff process can be a highly variable and unstructured period at risk for communication errors. The morning sign-in process used by resident physicians at teaching hospitals typically involves less rigorous handoff protocols than the resident evening sign-out process. Little research has been conducted on best practices for handoffs during morning sign-in exchanges between resident physicians. Research must evaluate optimal protocols for the resident morning sign-in process.
Methods
Three morning handoff protocols consisting of written, electronic, and face-to-face methods were implemented over 3 study phases during an academic year. Study participants included all interns covering the internal medicine inpatient teaching service at a tertiary hospital. Study measures entailed intern survey-based interviews analyzed for failures in handoff protocols with or without missed pertinent information. Descriptive and comparative analyses examined study phase differences.
Results
A scheduled face-to-face handoff process had the fewest protocol deviations and demonstrated best communication of essential patient care information between cross-covering teams compared to written and electronic sign-in protocols.
Conclusion
Intern patient handoffs were more reliable when the sign-in protocol included scheduled face-to-face meetings. This method provided the best communication of patient care information and allowed for open exchanges of information.
Keywords: Communication errors, interns, patient handoffs, patient information, teaching hospital
INTRODUCTION
The Accreditation Council for Graduate Medical Education (ACGME) initiated resident duty-hour restrictions in 20031 and made them more stringent in 2011.2 Since the implementation of resident duty-hour limits, many residency programs have struggled to optimize coverage for inpatient teaching services and have had to deal with an increased number of patient handoffs. These additional exchanges of information can increase the opportunities for breakdowns in the communication of patient information.3 As many as 15 handoffs per patient may occur over a 5-day hospitalization,4 and approximately 18 million patients are discharged from teaching hospitals each year.5
Studies have confirmed that the patient handoff process can be a highly variable and unstructured period at high risk for communication errors6-10 that result in documented adverse patient outcomes, prolonged hospitalizations, and increased medical costs from unnecessary tests and procedures.7 Although some of the studies predate duty-hour restrictions, others were conducted after the change, providing a source of continued concern regarding errors in teaching hospitals.
The risk of inadequate exchange of patient information during resident coverage requires an examination of patient handoff methods. In particular, the morning sign-in process has historically been a period of less rigorous protocols. Little research has been conducted on best handoff methods during this time period.11-13 Poor patient exchanges in the morning may leave resident physicians ill informed and unprepared, thus potentially affecting patient care and outcomes. Our study evaluated morning handoff methods to determine which resulted in the most consistent and effective exchange of patient information between on-call and primary team interns.
METHODS
Study Design
We conducted a longitudinal study at a medium-sized tertiary hospital. This university-affiliated hospital has a teaching service that employs a primary team of interns who provide patient care during the day and a single on-call intern who covers all teaching service patients overnight. These interns are appropriately supervised by senior residents and staff physicians. The hospital had developed a standardized patient handoff form to be used by all primary interns during evening patient handoffs. In response to the lack of a formal morning sign-in protocol at the institution, we designed, implemented, and examined study interventions to determine the best method of information exchange from the on-call intern to the primary team interns in the morning.
We implemented 3 morning handoff methods and individually evaluated them during 3 respective phases of gradually increasing duration (Figure). We hypothesized that fewer protocol deviations for morning sign-ins would occur during the adoption of the more rigorous patient handoff methods. We conducted the study during the academic year starting July 1, 2010, and ending June 30, 2011. The hospital's institutional review board granted the study exempt status.
Figure.

Illustration of morning handoff processes per study phase.
Study Participants
We invited all interns working on the inpatient internal medicine teaching service during the 12-month period to participate in the study. Eligible interns included all first-year residents from the internal medicine, family medicine, and transitional-year residency programs.
Study Intervention
During Phase I (months 1-3), the on-call intern recorded handwritten notes summarizing any overnight patient concerns or changes on a printed patient handoff form. The on-call intern was instructed to return the handoff form to a designated area so the primary interns could access the completed form when they returned to the hospital in the morning. The on-call intern was not required to provide face-to-face exchange of information.
In Phase II (months 4-7), the on-call intern used an electronic version of the standardized handoff form located on a secure intranet site. The on-call intern was required to type notes about overnight patient concerns or changes into the electronic patient handoff form instead of hand writing notes. The primary interns could then access this information electronically from the intranet site when they returned to the hospital in the morning. The on-call intern was not required to provide face-to-face exchange of information.
For phase III (months 8-12), formal sign-in rounds were scheduled each morning for a face-to-face handoff of information about overnight patient concerns or changes given by the on-call intern to the primary interns. The on-call intern was no longer required to complete handwritten or electronic versions of the patient handoff form.
During these 3 phases, interns did not change the standard protocol during evening sign-out rounds. Required sign-out information included patient demographics, room location, code status, principal diagnoses, key medications/active treatment interventions, follow-up to-do items for the on-call intern to complete, and potential issues the on-call intern might encounter. Subsequent morning sign-in processes during the study period had interns report information on any changes in the items reported during the prior evening sign-out rounds plus any overnight patient concerns or changes addressed by the on-call intern.
Standardized Questionnaire and Study Data
At the end of each month, the principal investigator (SRC) conducted structured interviews using a standardized questionnaire with each of the on-call interns and primary interns working on the inpatient internal medicine teaching service that month. Participation in monthly interviews was voluntary, with implied consent acquired at the time of interview.
The principal investigator used the standardized questionnaire to guide the interviews, individually and confidentially asking participants to recall patient handoffs during the prior month. The interviewer asked interns if any protocol failures by the on-call intern during morning handoffs occurred over the prior month. If the intern answered yes to the question, we asked the intern to elaborate on the communication issues involved and then recorded this information on the questionnaire in free-text format. The interviewer then asked interns if the on-call intern had not shared any patient changes or concerns. Again, if the intern answered yes, he or she was asked to elaborate on the concerns. This information was also recorded on the questionnaire in free-text format.
Two independent study team members (SRC, AMD) dually entered the deidentified standardized questionnaire data into a study database, converting free-text responses into categorical data based on key themes and study team consensus. Breakdowns in communication and/or deviations in handoffs reported in the free text were identified as protocol failures. These failures were further classified as either a deviation from protocol without an event or a deviation from protocol with an event. An intern could have responded yes for the presence of both types of protocol failures during the prior month.
Deviation from protocol included any recalled incident where sign-in did not occur in a manner consistent with the study phase. In Phase I, any occurrence where sign-in information was not made available (ie, handwritten notes were not on the printed patient handoff form) or was provided verbally was considered a deviation in protocol. Phase II deviations included any occurrences where sign-in information was not made available (ie, notes were not recorded in the electronic patient handoff form on the secure intranet site) or was provided verbally. In Phase III, any failure to provide information at formal face-to-face morning sign-in rounds or a sign-in that occurred outside of the scheduled sign-in rounds was considered a deviation in protocol.
Events were defined as any changes in patient status or treatment not properly reported to the primary interns by the on-call intern per the study protocol for the phase. Examples of events were problems with current treatment or the initiation of new medications, as well as admissions, discharges, or transfers of patients.
Statistical Analysis
We conducted descriptive statistical analyses for facility- and resident-level characteristics and survey-based interview data. Data were reported in counts and means. Interrater agreements for dually entered and categorized survey data were examined using kappa coefficients, with discrepancies remediated by consensus of study team members during a final data review session. Categorical interview data were examined using a one-sided Cochran-Armitage trend test for negative trends in the number of deviations with or without an event over the 3 study phases. A 1-sided Fisher exact test and relative risks with 95% confidence intervals (CIs) were also calculated for these data. Based on the study design, there was a possibility that interns could have been interviewed in multiple months during a study phase or during multiple study phases. Because interns were strictly asked to recall the past study month, each intern interview was treated as an independent observation. Study tests were based on a 0.05 significance level, and study analyses were conducted with SAS, version 9.2 (SAS Institute, Cary, NC).
RESULTS
Hospital and Intern Characteristics
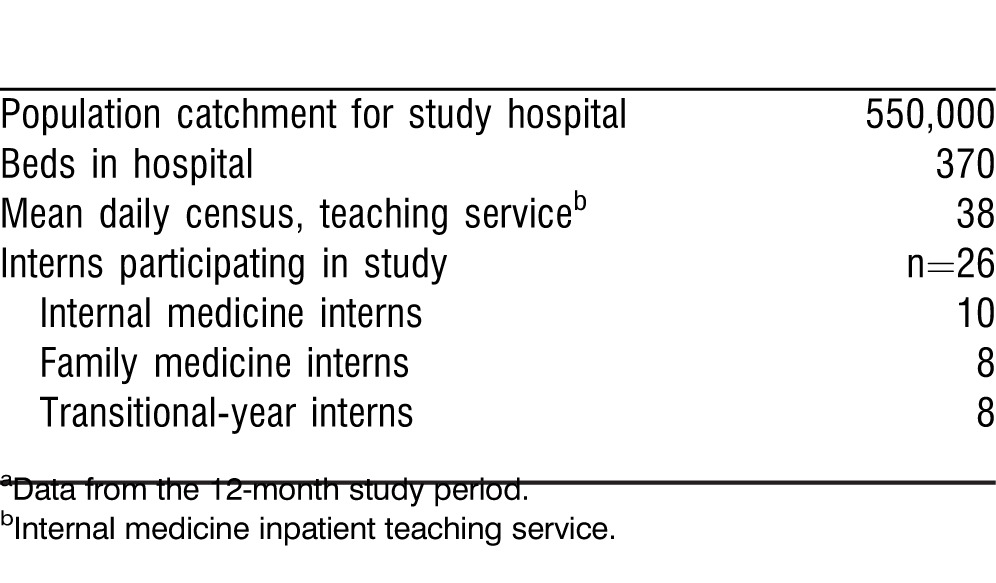
The study was conducted at a 370-bed hospital serving the central third of Iowa. Two handoffs per patient occurred in every 24-hour period. The 26 participants in the study included internal medicine, family medicine, and transitional-year interns who rotated through the inpatient internal medicine teaching service during the study period. Additional hospital and participating intern characteristics are presented in Table 1.
Table 1.
Hospital and Intern Program Characteristicsa
Study Data
We conducted a total of 47 structured intern interviews: Phase I, 12 interns (3 on-call and 9 primary team interns); Phase II, 17 interns (4 on-call and 13 primary team interns); Phase III, 18 interns (5 on-call and 13 primary team interns). All eligible interns participated in the study, and differences in the numbers of interns interviewed per study phase resulted from normal variations in the number of patients on the teaching service and the increasing lengths of the 3 study phases.
Protocol Failures
Primary and on-call intern responses during interviews about the patient sign-in process for the prior month revealed 43 failures out of a possible 94 opportunities for protocol failures with or without an event (Table 2). Of these failures, 16 occurred in Phase I, 17 in Phase II, and 10 in Phase III.
Table 2.
Number of Interns Reporting Patient Handoff Protocol Deviations Without an Event and/or With an Event per Study Phase
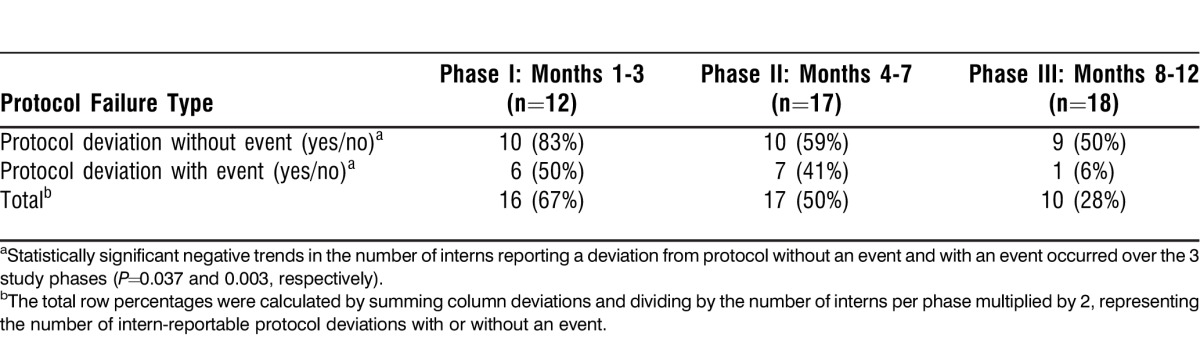
In Phase I, 10 out of 12 interns reported protocol failures without events, in which the on-call intern did not complete the handwritten patient handoff form and/or had not placed it in its proper location by the next morning. Six of these 12 interns also reported protocol failures with events during Phase I. Table 3 summarizes communication failures with events for each study phase.
Table 3.
Protocol Deviation Events per Study Phase
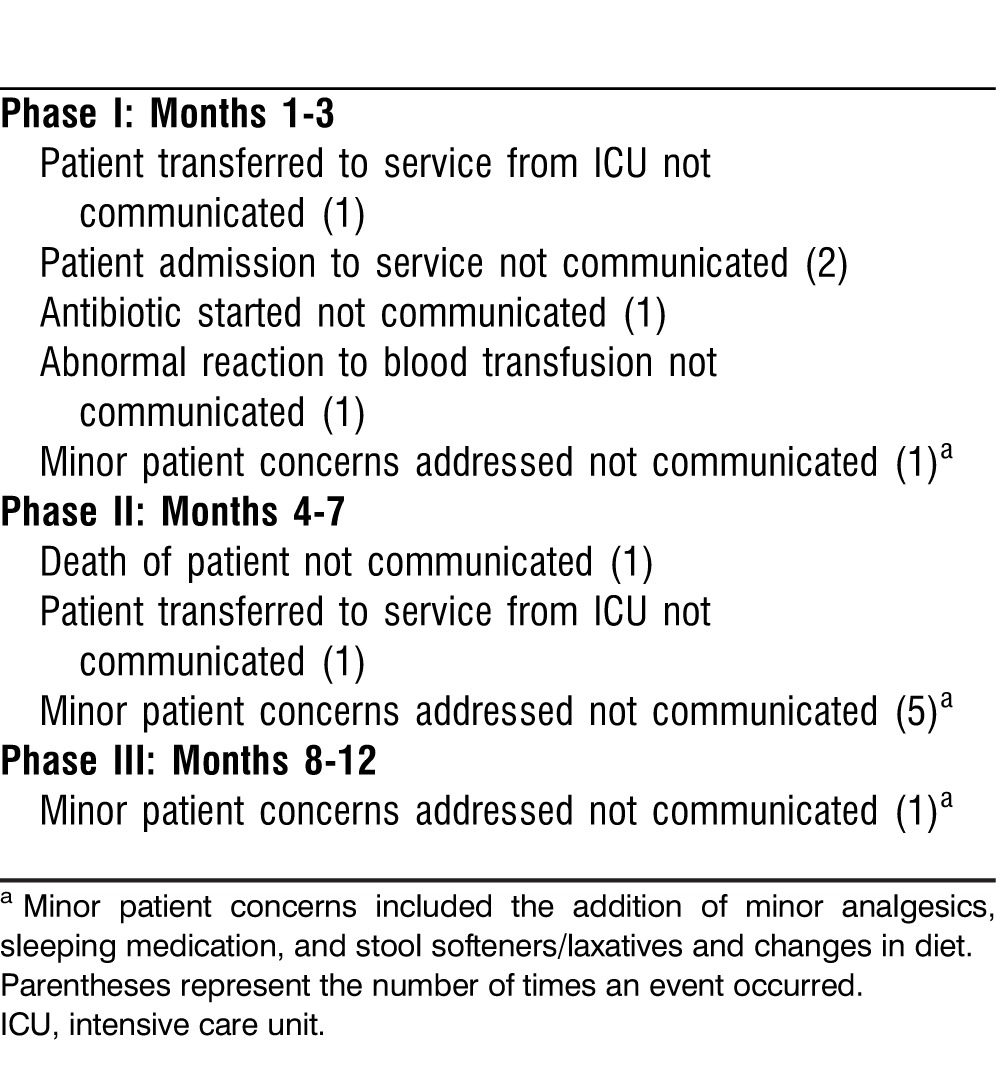
In Phase II, 10 of the 17 interns reported protocol failures without events, in which the on-call intern did not complete the electronic patient handoff form for the primary interns to access the next morning. Seven of these 17 interns also reported protocol failures with events during Phase II.
In Phase III, 9 of the 18 interns reported protocol failures without events, in which the on-call intern did not share patient handoff information during the formal face-to-face meeting in the morning. One of these 18 interns also reported a protocol failure with an event.
Over the study phases, the proportion of interns who reported protocol failures without an event had a significant negative trend of −0.2562 (95% CI: −0.519, 0.007; P=0.037, based on a 1-sided test). No significant risks of protocol failure without an event between phases were revealed. Meanwhile, the proportion of interns who reported protocol failures with an event over the study year had a significant negative trend of −0.4076 (95% CI: −0.639, −0.177; P=0.003, based on a 1-sided test). Interns in Phase I had a 9 (95% CI: 1.2, 65.6; P=0.009) times greater risk of reporting protocol failure with an event compared to interns in Phase III. Interns in Phase II had a 7.4 (95% CI: 1.1-54.1; P=0.016) times greater risk of reporting protocol failure with an event compared to Phase III. No significant risk of protocol failures without events was revealed between Phases I and II.
DISCUSSION
Patient handoffs should entail clear and concise exchanges of pertinent medical information between team members, but problems can be encountered as one team member assumes responsibility for the care of a patient from another team member. This study is one of the first published to focus on the morning sign-in process that occurs daily in teaching hospitals across the country. Multiple prior studies have evaluated the evening sign-out process.4,13-21 These prior studies confirmed the importance of using a standardized handoff instrument and the need to include face-to-face communication as a part of the sign-out process.4,13,16-18,20-22 The present study examined 3 patient handoff methods for the morning sign-in process to identify the most effective method interns used. No known prior studies on resident sign-outs or sign-ins compared the effectiveness of paper, electronic, and scheduled face-to-face patient handoff methods.
During Phase I, on-call interns recorded handwritten notes on a printed patient handoff form summarizing any overnight patient concerns or changes. Results demonstrated that on-call interns did not consistently complete the sign-in sheets or return them to the designated area prior to the arrival of the primary interns. This phase held the greatest risk for a protocol failure with an event.
During Phase II, the on-call intern typed notes about overnight patient concerns or changes into an electronic handoff form located on a secure intranet site. Intern interviews demonstrated that the overnight notes were sometimes absent or missing important information. In Phase II, a lower percentage of failures in the handoff process occurred than in Phase I, with reported events resulting from missing information. This method appeared more efficient, but still presented a level of risk to patient care.
In Phase III, the primary team interns met face-to-face with the on-call intern for rounds each morning. Results from this phase demonstrated imperfect intern attendance at morning sign-in rounds. However, when data from this phase were compared to the other 2 phases, Phase III had the fewest events from unreported patient information. Improvements in the sign-in process were significant when reviewing the number of interns reporting events during face-to-face sign-ins compared to the other phases.
Of the few published studies that have addressed the morning sign-in process, data have shown sign-ins to be less organized than sign-outs. Sign-in often involves only exchanges of handoff forms or haphazard verbal exchanges of information.11,12,22 This study demonstrated that the best method for ensuring that the on-call intern adequately transfers patient information to primary interns returning to the hospital in the morning is a formal face-to-face meeting.
Medical errors are frequently caused by poor communication between healthcare professionals.3,23 Content omissions in communicating information can potentially impact patient care.7 Scheduled face-to-face sign-ins can add an extra layer of security for preventing poor exchanges of information that occur during the handoff process. These face-to-face meetings also allow residents to ask questions of the on-call intern to clarify any events that may have occurred overnight. Emphasis must be placed on 100% intern attendance at face-to-face sign-in meetings to ensure that no communication failures occur.
Most published literature on patient handoffs at teaching institutions confirms that the methods for conducting face-to-face sign-in and sign-out rounds require examination. Studies have shown the benefits from active participation by senior residents13,14 and supervising faculty.17,22 However, a survey of internal medicine residency programs confirmed that attending physician involvement in the patient handoff process may be minimal at best.24 Current ACGME Common Program Requirements specify “(s)ponsoring institutions and programs must ensure and monitor effective, structured hand-over processes to facilitate both continuity of care and patient safety. Programs must ensure that residents are competent in communicating with team members in the hand-over process.”2 Studies such as ours provide additional support for institutions to develop formal sign-out and sign-in processes for residents. These processes should include active participation of supervising faculty who can help residents develop competence in the patient handoff process. With changes in resident duty-hour limits, the examination of patient handoffs remains a fertile ground for educational research.
Limitations
The present study was conducted in an internal medicine residency program at a single teaching hospital. All interns on the internal medicine teaching service participated in the study, providing a representative sample. Data were taken from structured interviews conducted at the end of each month. The validity of intern-reported protocol failures and events depended on the accuracy of recalled information. The use of identical data collection methods throughout the 3 study phases minimized the risk of differentially missing information between phases. No changes at the institution during the study period that would have altered the patient handoff process were known, but intern progression through training may have affected the quality of handoffs. However, during the study period, residency program leadership stressed to interns at orientation and at the beginning of each rotation block the importance of thorough exchanges of patient information during evening sign-out and morning sign-in processes. These actions provided consistent and continual reinforcements to the interns. Lastly, the present study solely focused on the patient handoff process and did not evaluate subsequent patient outcomes.
CONCLUSION
This study demonstrated that a scheduled face-to-face handoff process improved the communication of essential patient care information between cross-covering teams of interns. This process is a low-cost method that residency programs can easily use to promote effective patient handoffs. Other teaching hospitals and different types of inpatient teaching services should replicate and test the implementation of this handoff method to examine its overall utility. Future research may also examine the generalizability of these results to the resident sign-out process. This study is important because teaching hospitals must ensure the best exchange of patient information while adhering to work-hour restrictions and an increased number of patient handoffs.
Footnotes
Components of this study were presented in poster format at the Association for Hospital Medical Education (AHME) Meeting, Ft. Lauderdale, FL, May 16-19, 2012.
The authors have no financial or proprietary interest in the subject matter of this article.
Epitoma
With the advent of resident duty hours, transitions of care between physicians have become more frequent and present potential risk for patient safety. The Accreditation Council for Graduate Medical Education has recognized this risk and mandated that programs ensure and monitor effective structured hand-over processes. This study from the University of Iowa–Des Moines is one of the first to demonstrate that face-to-face transfer of care was more likely to ensure a consistent structured transfer of care compared to a paper or electronic handoff in the morning. More of these types of studies are needed to ensure that we are using and teaching the best practices for patient safety.
—Guest Editor Leonardo Seoane, MD
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties competencies for Patient Care, Medical Knowledge, Interpersonal and Communication Skills, and Systems-Based Practice.
REFERENCES
- 1.American Medical Association, Accreditation Council for Graduate Medical Education. Directory of Graduate Medical Education Programs, 2003-2004. Chicago, IL: American Medical Association Press;; 2003. [Google Scholar]
- 2.American Medical Association, Accreditation Council for Graduate Medical Education. Graduate Medical Education Directory, 2011-2012. Chicago, IL: American Medical Association Press;; 2011. [Google Scholar]
- 3.Petersen LA, Brennan TA, O'Neil AC, Cook EF, Lee TH. Does housestaff discontinuity of care increase the risk for preventable adverse events? Ann Intern Med. 1994 Dec 1;121(11):866–872. doi: 10.7326/0003-4819-121-11-199412010-00008. [DOI] [PubMed] [Google Scholar]
- 4.Vidyarthi AR, Arora V, Schnipper JL, Wall SD, Wachter RM. Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign-out. J Hosp Med. 2006 Jul;1(4):257–266. doi: 10.1002/jhm.103. [DOI] [PubMed] [Google Scholar]
- 5.Agency for Healthcare Research and Quality. National and regional estimates on hospital use for all patients from the HCUP Nationwide: 2009 national statistics. http://hcupnet.ahrq.gov/HCUPnet.jsp?Id=F7F06B722D37FDEF&Form=DispTab&JS=Y&Action=%3E%3ENext%3E%3E&_InDispTab=Yes&_Results=Print&SortOpt. Accessed August 23, 2012.
- 6.White AA, Pichert JW, Bledsoe SH, Irwin C, Entman SS. Cause and effect analysis of closed claims in obstetrics and gynecology. Obstet Gynecol. 2005 May;105(5 Pt 1):1031–1038. doi: 10.1097/01.AOG.0000158864.09443.77. [DOI] [PubMed] [Google Scholar]
- 7.White AA, Wright SW, Blanco R, et al. Cause-and-effect analysis of risk management files to assess patient care in the emergency department. Acad Emerg Med. 2004 Oct;11(10):1035–1041. doi: 10.1197/j.aem.2004.04.012. [DOI] [PubMed] [Google Scholar]
- 8.Laine C, Goldman L, Soukup JR, Hayes JG. The impact of a regulation restricting medical house staff working hours on the quality of patient care. JAMA. 1993 Jan 20;269(3):374–378. [PubMed] [Google Scholar]
- 9.Beach C, Croskerry P, Shapiro M. Center for Safety in Emergency Care. Profiles in patient safety: emergency care transitions. Acad Emerg Med. 2003 Apr;10(4):364–367. doi: 10.1111/j.1553-2712.2003.tb01350.x. [DOI] [PubMed] [Google Scholar]
- 10.Gandhi TK. Fumbled handoffs: one dropped ball after another. Ann Intern Med. 2005 Mar 1;142(5):352–358. doi: 10.7326/0003-4819-142-5-200503010-00010. [DOI] [PubMed] [Google Scholar]
- 11.Arora V, Johnson J, Lovinger D, Humphrey HJ, Meltzer DO. Communication failures in patient sign-out and suggestions for improvement: a critical incident analysis. Qual Saf Health Care. 2005 Dec;14(6):401–407. doi: 10.1136/qshc.2005.015107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Helms AS, Perez TE, Baltz J, et al. Use of an appreciative inquiry approach to improve resident sign-out in an era of multiple shift changes. J Gen Intern Med. 2012 Mar;27(3):287–291. doi: 10.1007/s11606-011-1885-4. Epub 2011 Oct 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Horwitz LI, Moin T, Krumholz HM, Wang L, Bradley EH. What are covering doctors told about their patients? Analysis of sign-out among internal medicine house staff. Qual Saf Health Care. 2009 Aug;18(4):248–255. doi: 10.1136/qshc.2008.028654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chang VY, Arora VM, Lev-Ari S, D'Arcy M, Keysar B. Interns overestimate the effectiveness of their hand-off communication. Pediatrics. 2010 Mar;125(3):491–496. doi: 10.1542/peds.2009-0351. Epub 2010 Feb 8. [DOI] [PubMed] [Google Scholar]
- 15.Arora V, Kao J, Lovinger D, Seiden SC, Meltzer D. Medication discrepancies in resident sign-outs and their potential to harm. J Gen Intern Med. 2007 Dec;22(12):1751–1755. doi: 10.1007/s11606-007-0415-x. Epub 2007 Oct 26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bernstein J, MacCourt DC, Jacob DM, Mehta S. Utilizing information technology to mitigate the handoff risks caused by resident work hour restrictions. Clin Orthop Relat Res. 2010 Oct;468(10):2627–2632. doi: 10.1007/s11999-010-1376-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Borowitz SM, Waggoner-Fountain LA, Bass EJ, Sledd RM. Adequacy of information transferred at resident sign-out (in-hospital handover of care): a prospective survey. Qual Saf Health Care. 2008 Feb;17(1):6–10. doi: 10.1136/qshc.2006.019273. [DOI] [PubMed] [Google Scholar]
- 18.Flanagan ME, Patterson ES, Frankel RM, Doebbeling BN. Evaluation of a physician informatics tool to improve patient handoffs. J Am Med Inform Assoc. 2009 Jul-Aug;16(4):509–515. doi: 10.1197/jamia.M2892. Epub 2009 Apr 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gakhar B, Spencer AL. Using direct observation, formal evaluation, and an interactive curriculum to improve the sign-out practices of internal medicine interns. Acad Med. 2010 Jul;85(7):1182–1188. doi: 10.1097/ACM.0b013e3181da8370. [DOI] [PubMed] [Google Scholar]
- 20.Van Eaton EG, Horvath KD, Lober WB, Rossini AJ, Pellegrini CA. A randomized, controlled trial evaluating the impact of a computerized rounding and sign-out system on continuity of care and resident work hours. J Am Coll Surg. 2005 Apr;200(4):538–545. doi: 10.1016/j.jamcollsurg.2004.11.009. [DOI] [PubMed] [Google Scholar]
- 21.Wohlauer MV, Rove KO, Pshak TJ, et al. The computerized rounding report: implementation of a model system to support transitions of care. J Surg Res. 2012 Jan;172(1):11–17. doi: 10.1016/j.jss.2011.04.015. Epub 2011 May 5. [DOI] [PubMed] [Google Scholar]
- 22.Salerno SM, Arnett MV, Domanski JP. Standardized sign-out reduces intern perception of medical errors on the general internal medicine ward. Teach Learn Med. 2009 Apr-Jun;21(2):121–126. doi: 10.1080/10401330902791354. [DOI] [PubMed] [Google Scholar]
- 23.Sutcliffe KM, Lewton E, Rosenthal MM. Communication failures: an insidious contributor to medical mishaps. Acad Med. 2004 Feb;79(2):186–194. doi: 10.1097/00001888-200402000-00019. [DOI] [PubMed] [Google Scholar]
- 24.Horwitz LI, Krumholz HM, Green ML, Huot SJ. Transfers of patient care between house staff on internal medicine wards: a national survey. Arch Intern Med. 2006 Jun 12;166(11):1173–1177. doi: 10.1001/archinte.166.11.1173. [DOI] [PubMed] [Google Scholar]