
Figure 2.
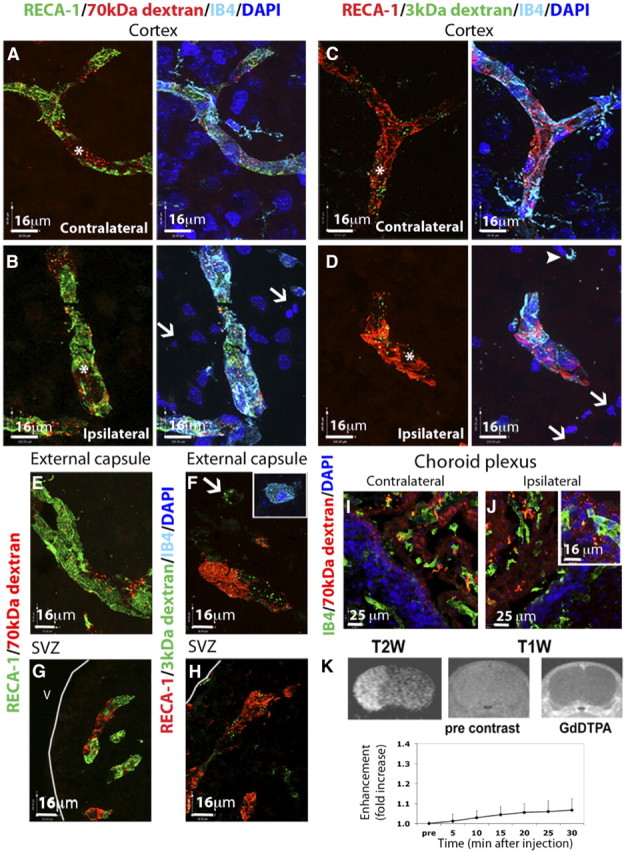
Extravasation of intravascular tracers of different size is low in the injured regions of the neonate after acute MCAO. A–D, The distribution of TRITC-conjugated 70 kDa dextran (A, B) and fluorescein-conjugated 3 kDa dextran (C, D) was restricted to the vasculature (RECA-1+/IB4+ vessels, asterisks) in the contralateral (A, C) brain hemisphere. In the injured areas (B, D), intravenous tracers colocalized with brain vessels (RECA1+/IB4+, asterisks) and were not observed in the extravascular spaces. E, F, The distribution of 3 and 70 kDa dextran was restricted to the brain vasculature in the ipsilateral external capsule 24 h after reperfusion (E, F), although occasional 3 kDa signal was detected in microglia/macrophages located in this brain region (F, arrow and inset). G, H, No leakage of 70 kDa dextran (G) or 3 kDa dextran (H) was observed in the ipsilateral SVZ 24 h after reperfusion. I, J, Leakage of 70 kDa dextran was detected in the choroid plexus in both contralateral (I) and ipsilateral (J) ventricles. K, Coronal T1-weighted images showing contrast imaging of Gd-DTPA 24 h after neonatal MCAO. Contrast was increased in areas outside the brain (right) but was minimal in the brain up to 30 min after injection of Gd-DTPA (right vs middle, bottom graph). Injured areas were identified in the same animals by T2-weighted imaging (left). V, ventricle.