
Figure 1.
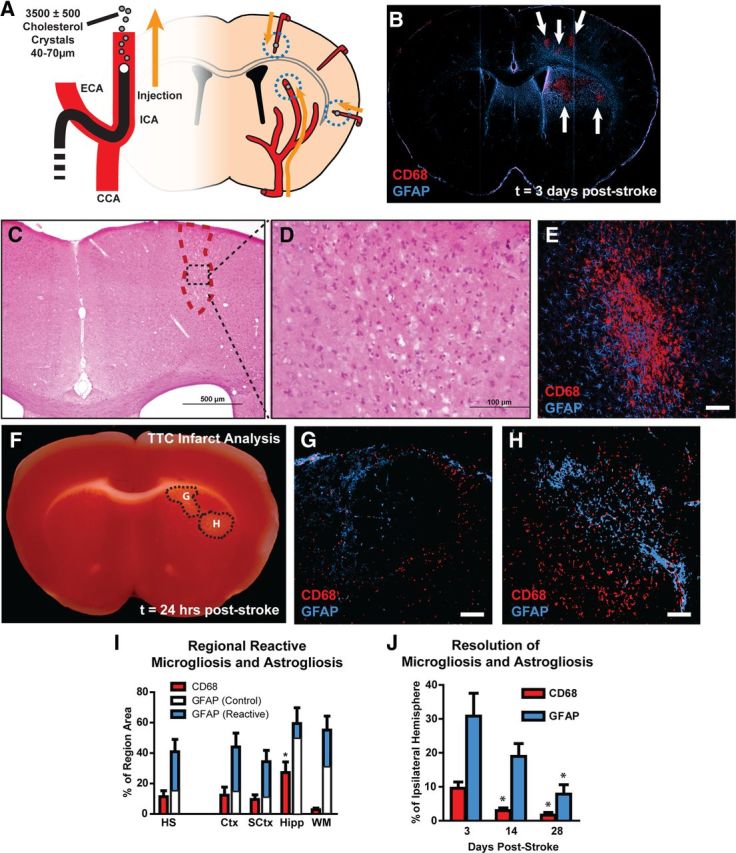
Widespread reactive gliosis surrounding diffuse ischemic lesions. A, Schematic of diffuse stroke model. A total of 3500 ± 500 cholesterol crystals (40–70 μm) were injected unilaterally via the ICA. Ischemic lesions formed along the deep segments of penetrating cerebral arteries. B, Ischemic lesions (arrows) are defined by immunolabeling against CD68 and GFAP. Lesions consist of CD68-poisitive cores surrounded by large areas of reactive astrogliosis. C, D, H&E staining 3 d after injury indicates a small columnar cortical lesion that with marked macrophage infiltration. E, CD68/GFAP immunolabeling of a consecutive slice demonstrates that microinfarcts apparent by H&E labeling are characterized by a CD68-positive core surrounded by a wide field of reactive astrogliosis. F–H, TTC staining and immunolabeling against CD68 and GFAP 24 h after stroke shows that lesions are detectible by TTC, and at this time point are surrounded by a rim of reactive microglia and astrocytes. I, Three days after stroke, CD68-immunolabeling (red bars) occupied a larger proportion of the hippocampus than other brain regions (*p < 0.05, ANOVA). GFAP immunoreactivity (blue bars) occupied large areas surrounding CD68-positive cores. White bars reflect control GFAP immunoreactivity in contralateral hemisphere. J, Fourteen days after ischemic injury, CD68-positive lesions occupied a smaller proportion of the ipsilateral hemisphere compared to 3 d (*p < 0.05, ANOVA). GFAP immunoreactivity was not significantly reduced from levels at 3 d until 28 d after stroke (*p < 0.05, ANOVA). HS, Hemisphere. Scale bars: 50 μm.