
Fig. 4.
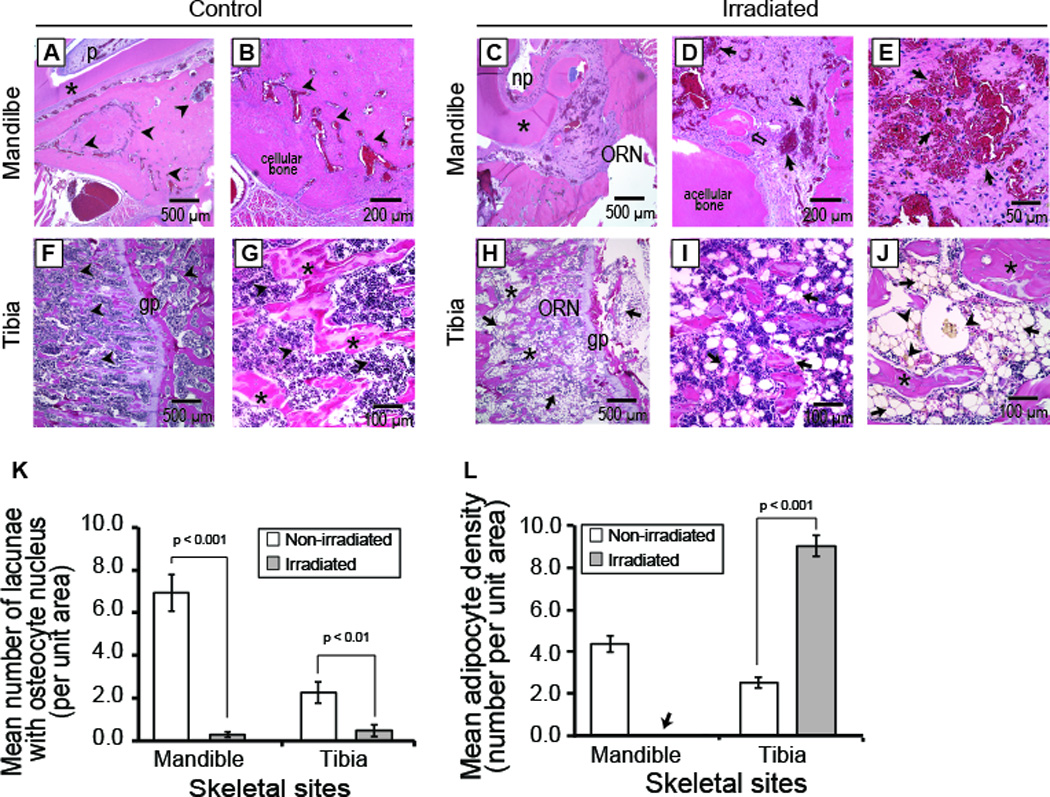
Differential histological presentations of mandible and tibia osteoradionecrosis. Non-irradiated mandibular bone (control) (top panel, A, B) displayed a network of normal blood vessels, abundant osteocytes and marrow elements (black arrow heads) in proximity to the mandibular incisor composed of normal dentin (black star) and pulp tissues (p). Similarly, non-irradiated tibia (bottom panel, F, G) displayed abundant marrow elements (arrow heads) and trabecular bone (black star) plus intact growth plate (gp). Irradiated mandible (top panel, C, D, E) succumbed to ORN with characteristic acellular necrotic bone lacking osteocytes, necrotic pulp (np), sequestrum (clear black arrow), and damaged vasculature with erythrocyte extravasation (solid black arrows). The necrotic regions in the mandible were infiltrated by eosinophilic amorphous ground substance with abundant basophilic cells. Radiation damage in tibia (bottom panel, H, I, J) consisted of trabecular micro-fracture with disjointed and fewer trabecular bone (black star), altered architecture of the growth plate (gp), fatty marrow elements (black arrows), coalesced adipocytes and fatty microvesicles (black arrowheads). ORN was associated with empty osteocyte lacunae in both mandible (p < 0.001) and tibia (p < 0.01) (K); while adipocytes were also suppressed in the mandible (black arrow, L), there was marked adipocytic infiltration in the tibia (p < 0.001)(L). [ORN = osteoradionecrosis].