

Abstract
Periodontitis is the most common localized dental inflammatory disease related with several pathological conditions like inflammation of gums (gingivitis), degeneration of periodontal ligament, dental cementum and alveolar bone loss. In this perspective, the various preventive and treatment modalities, including oral hygiene, gingival irrigations, mechanical instrumentation, full mouth disinfection, host modulation and antimicrobial therapy, which are used either as adjunctive treatments or as stand-alone therapies in the non-surgical management of periodontal infections, have been discussed. Intra-pocket, sustained release systems have emerged as a novel paradigm for the future research. In this article, special consideration is given to different locally delivered anti-microbial and anti inflammatory medications which are either commercially available or are currently under consideration for Food and Drug Administration (FDA) approval. The various in vitro dissolution models and microbiological strain investigated to impersonate the infected and inflamed periodontal cavity and to predict the in vivo performance of treatment modalities have also been thrashed out. Animal models that have been employed to explore the pathology at the different stages of periodontitis and to evaluate its treatment modalities are enlightened in this proposed review.
Keywords: Chemotherapeutic agents, intra-pocket devices, mechanical therapies, oral hygiene
INTRODUCTION
Periodontal disease is the most common localized dental inflammatory disease caused by bacterial infection of the periodontal cavity associated with subgingival plaque.[1] This is often associated with diverse pathological conditions like inflammation of gums (gingivitis), degeneration of periodontal ligament and dental cementum and alveolar bone loss.[2] Gingivitis is the initial stage of disease which may or may not progress into severe condition like periodontitis which shows evidences of cavity formation, loss of clinical attachment level and degeneration of alveolar bone.[3]
There is an abundance of literature reports of bacteria being the only microbes responsible for the occurrence of periodontal disease. They are believed to release enzymes and toxins that destroy the periodontium.[4] However, some of the recent studies have offered evidences suggesting that the host's immune inflammatory responses also play an important role in the destruction of periodontal attachment structures.[5] The host responses results in a cascade of events leading to connective tissue and alveolar bone loss.[6] The series of events are often initiated from the lipo-polysaccharides present in bacteria that stimulate the release of cytokines.[7] Cytokines are inflammatory mediators that stimulate fibroblasts and epithelial cells. These cells consequently release the prostaglandins (PGE2) and matrix metalloproteinase. Prostaglandins induce the alveolar bone resorption while matrix metalloproteinase (collagenase) damages or destroys the connective tissue. In addition, interleukin-1β and tumor necrosis factor-α are other pro-inflammatory mediators which are also involved in the damage of the periodontium.[1,7–9] Despite the fact that the presence of bacteria and their products are important factors to stimulate the disease, the sensitivity of the disease and its progression rate are also governed by the susceptibility of the host.[3]
Host response and increased patient's susceptibility to periodontitis can be affected by a number of environmental and acquired risk factors like heredity, smoking, hormonal variation (during pregnancy, menopause), systemic diseases (Marfan's and Ehlers-Danlos syndromes, diabetes, osteoporosis, HIV, neutropenias), stress, nutritional deficiencies, medications [calcium channel blockers, immunomodulatory agents, anticonvulsants] and poor oral hygiene.[10–12]
These risk factors can also affect the onset, rate of progression, severity of periodontal disease and response to therapy and therefore should be evaluated so as to design treatment plan and maintenance therapy.[3] The susceptibility of patients to periodontitis can be reduced by modifying the risk factors by frequent dental visits, smoking cessation, intake of hormonal, calcium, biphosphonate and nutritional supplements and improved oral hygiene.[3]
The present review highlights the importance of oral hygiene besides providing an insight into the various conventional approaches used for the effective prevention and treatment of periodontal diseases. Over the fast few years, researchers have focused on strategies for optimizing the delivery of the drugs to the periodontal pocket for the treatment of periodontal diseases. The various intrapocket drug delivery systems developed for the localized delivery of therapeutic agents, thereby obviating the shortcomings associated with the systemic delivery of antimicrobial agents used in the treatment of periodontal diseases, have also been discussed. A thorough knowledge of the various evaluation techniques used for the testing of developed periodontal drug delivery systems is a very important aspect for confirming the usefulness and commercial viability of the developed dosage form. Almost all the reviews published so far only concentrate on the various delivery systems used for the treatment of periodontal diseases, with no mention of their evaluation strategies used. The present review, besides giving information on the various conventional approaches used for the effective prevention and treatment of periodontal diseases, describes the various in vitro models, in vivo models and anti microbial studies which have been carried out by various researchers for evaluating the efficacy of the developed periodontal dosage form.
APPROACHES FOR THE TREATMENT OF PERIODONTAL DISEASES
Periodontal disease is usually initiated by opportunistic infections. Treatment of the periodontal disease is a great challenge because the infection occurs due to bacterial biofilm which is highly resistant to the antimicrobials and host response.[3] Removal of the bacteria from the periodontal cavity is a tedious task and the bacteria continue to remain in the oral cavity. The severity of disease mainly depends on the bacterial components present as well as on the host response.[3,8]
In the initial stage of the disease, inflammation is limited to the gingiva (gingivitis) but later extends to the deeper tissues in turn leading to gingival swelling, bleeding of gums and halitosis. In the late phase of disease, the supporting collagen of periodontium begins to degenerate, resorption of alveolar bone takes place and epithelial tissue of gingiva migrates which leads to formation of pockets.[1,13] The choice of the treatment strategy therefore depends upon the stage of disease.
Various approaches applied for the treatment of disease include surgical intervention, mechanical therapy and use of pharmacological agents.[3,14,15] Medications are specifically used for better management of periodontitis and include antimicrobials that change microbial flora in periodontal milieu and host response modulating agents which modify host response like reduction of excessive enzymes level, cytokines, prostaglandins and osteoclast activity.[16] The anatomy of healthy, infected and diseased tooth is represented in Figure 1 and the pathogenesis of periodontal disease and possible treatments is represented in Figure 2.
Figure 1.
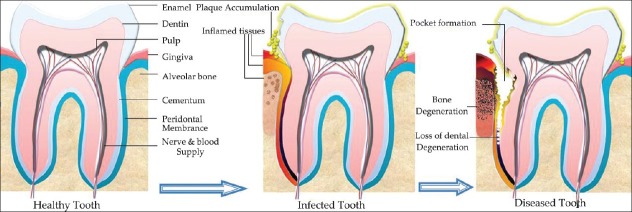
Anatomy of healthy, infected and diseased tooth
Figure 2.
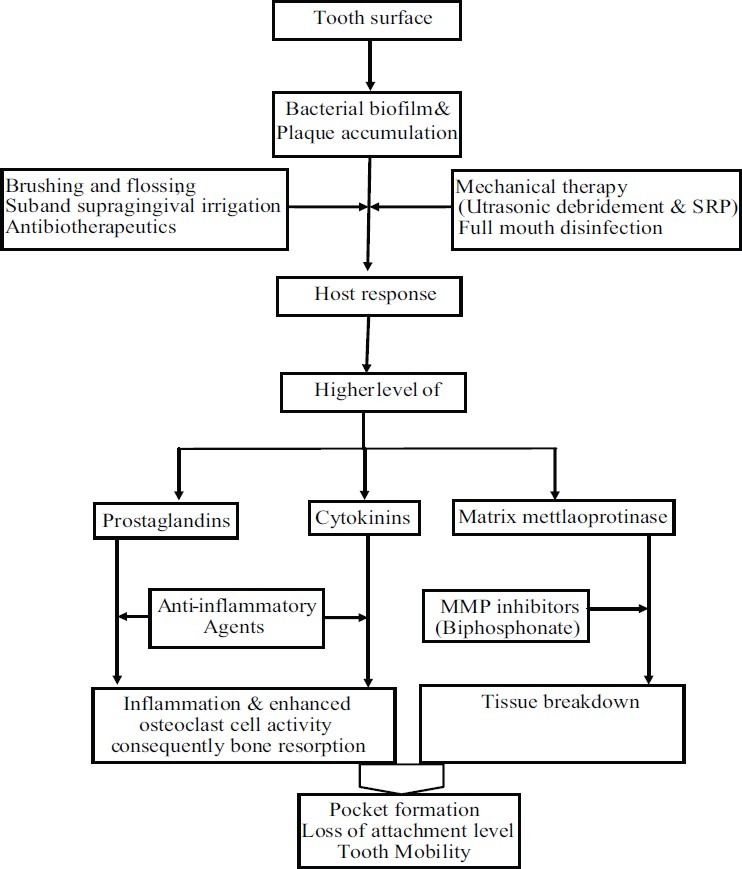
Progression of disease and intervention therapies
The incidence of initiation and progression of periodontal diseases can be reduced by maintenance of good oral hygiene.
STRATEGIES FOR MAINTENANCE OF GOOD ORAL HYGIENE
The initial events of the disease could be often countered by following practices which assures oral hygiene.
Brushing and flossing
The first-line approach is brushing and flossing which appreciably reduces microbes in oral cavity.[3] The American Dental Association (ADA) recommends brushing for 2 min twice a day and flossing once a day.[3] It aids effectively in the reduction of gingivitis and in the treatment of periodontitis. However, a large part of the population does not follow the above mentioned protocol. Therefore, a large population, approximately more than 50% of adults suffer from gingivitis.[17,18]
Supragingival irrigation
Supragingival irrigation potentiates the effectiveness of tooth-brushing and aids in the reduction of gingival inflammation in those patients who do not follow good oral hygiene.[19] A positive correlation was found between supragingival irrigation, which could be either by acetyl salicylic acid (ASA) or water and the reduction in disease severity. Thus, regular supragingival irrigation with either 0.3% ASA or water besides usual oral hygiene seems to be a valuable extra periodontal supportive remedy in patients showing the signs of moderate to severe periodontitis.[20] Antiseptic irrigations have been employed for managing plaque buildup.[21] Peridex, Perioguard and Listrine are the antiseptic irrigations clinically approved by American Dental Association. Clinical studies have revealed other benefits of these antiseptic irrigations, such as control of halitosis,[22,23] improvement in gingival health around dental implants,[24] reduction in plaque and gingivitis in orthodontic patients.[21]
Subgingival irrigation
The status of subgingival irrigation in the management of periodontitis remains a topic of debate. Several studies indicated the impact of subgingival irrigation as a monotherapy and in combination with root planning and revealed that subgingival irrigation with a variety of agents reduced the amount of gingival microbial load.[25,26] Subgingival irrigation helps to diminish gingival inflammation despite unchanged plaque levels[27–29] by diluting plaque toxicity, interference with subgingival plaque maturation, or possibly by washing away unattached plaque.[29,30] Pocket irrigation is able to reduce microbial load in the pocket and offers some better clinical parameters like pocket depth, bleeding of gum etc, but is associated with a major drawback of showing erratic results which is probably attributed to short residence time of the drug in the periodontal pocket.[31] The biologic rationale for performing subgingival irrigation is to nonspecifically reduce microbial deposits that may induce periodontal diseases. Therefore, it is an attempt to directly reduce the pocket microflora to block the initiation of periodontitis or its smooth progress.[32]
However, the effects which can be achieved with scaling and root planning are not possible with single episodes of subgingival irrigation.[33,34] Various studies have revealed that subgingival irrigation is able to decrease mean probing depths by not more than 1 mm.[35,36] If root planning preceded irrigation therapy, probing depths were decreased to 2 to 3 mm. Therefore, if probing depth reduction is desired, root planning is indicated.[37]
Mechanical therapies for the treatment of periodontal diseases
Plaque is a mixture of bacteria, minerals and some food residue. Some plaque hardens into calculus. Often, plaque and calculus do not come off with the brush and floss and cause inflammation, an ongoing state of gingivitis.[38]
Tooth scaling is an effective method for inhibition and cure of gingivitis. Periodontal scaling procedures include the removal of plaque, calculus and stain from the crown and root surfaces of teeth.[39] Scaling and root planning has become the “gold standard” nonsurgical treatment of periodontitis.[40] Several clinical investigations have indicated that it effectively reduces the microbial level in periodontal pocket and improves the clinical parameters like bleeding on probing and probing depths and clinical attachment level.[40] Scaling and root planning may be performed using a number of dental tools, including sonic or ultrasonic instruments and hand instruments, such as periodontal scalers and curettes.[3]
Manual scaling and root planning can often be difficult and time consuming due to the complex and unfavorable root morphology when working blindly at deep pocket sites.[41,42] Several investigations have supported the controversy that root planning can reduce probing depths, gain clinical attachment and inhibit disease progression.[43] Scaling and root planning is a localized treatment but is not able to get rid of the pathogenic bacteria at all times due to their presence within periodontal tissues, or in the case of deeper pockets, where the instruments are difficult to reach. As probing depth increases, manual instruments become less efficient to confiscate the root of the problem.[43,44]
This led to the development of power-driven ultrasonic mechanical instruments that have enhanced the capability of the operator to reach into furcations more efficiently and to go through the depth of the pocket more conveniently.[45] These instruments cause the elimination of root surface accretions with a vibrating mechanical device.[46] Many ultrasonic scalars also include a liquid output or lavage, which aids in cooling the tool during use, as well as rinses all the unwanted materials from the teeth and gum line. The lavage can also be used to deliver antimicrobial agents.[46]
Ultrasonic scalars have been extensively used in recent years due to their ease to use, the time advantage, a reduction in effort and stress of the operator.[41,47] However, several studies have also reported that the microbiological and clinical effects achieved by ultrasonic debridement are similar to those achieved by manual scaling and root planning.[46,48,49]
After mechanical debridement, the microbial load drops to 0.1%.[50] However, it recolonizes within a week this time with less pathogenic composition.[51] In this perspective, the concept of one stage, full-mouth disinfection was introduced in 1995 for the avoidance of re-infection from microbial reservoirs and showed potential results.[52] Objective of this concept was to eliminate or at least suppress all periodontopathogens in a very short time period not only from the periodontal pockets but also from all intraoral niches such as tongue, tonsils and mucus membrane.[53] One stage, full mouth disinfection comprises of combination of therapeutic efforts i.e. mechanical therapy and antimicrobial therapy.[53] Swierkot and coworkers performed a comparative study between one-stage full-mouth disinfection (FMD), full-mouth scaling and root planning (FM-SRP) and quadrant scaling and root planning (Q-SRP) in patients with generalized chronic periodontitis. FMD group was treated as per the following design: scaling and root planning in two sessions within 24 h, one subgingival application of 1% chlorhexidine gel, brushing of dorsum of the tongue with 1% chlorhexidine gel for 1 min, spraying of each tonsil four times with 0.2% chlorhexidine spray and rinsing twice for 1 min with 0.2% chlorhexidine solution. Patients were instructed to rinse the oral cavity once daily for 30 s with 0.2% chlorhexidine solution and also spray the tonsils once daily with 0.2% spray for 14 days after the treatment. In the FM-SRP-group, scaling and root planning was performed in two sessions within 24 h without antiseptics and in the Q-SRP group scaling and root planning was performed quadrant-wise in weekly intervals and no additional antiseptics were used. In this study, all three treatment modalities showed significant clinical improvement at any time. In the FM-SRP group, reduction of probing depth and bleeding on probing were significantly higher as compared to other two groups. The bacteria could be reduced in each group even though this reduction was only significant for Prevotella intermedia in the FMD group after 8 months of the treatment. All the treatment modalities (FMD, FM-SRP and Q-SRP) showed an improved clinical and microbiological profile upto 8 months, after which no significant differences were observed in any group.[54]
The use of lasers is also being investigated as a new technique for the treatment for periodontal disease.[55] Several features, such as ablation or vaporization, hemostasis, and sterilization effects, make this laser treatment technique as an adjunct or alternatives to conventional mechanical periodontal therapy.[56] The CO2 and Neodymium-doped: Yttrium-Aluminum-Garnet (Nd:YAG) lasers have been approved for soft tissue treatment and Erbium–doped: Yttrium–Aluminum-Garnet (Er:YAG) laser has been introduced which can be used for periodontal hard tissues treatment such as root surface debridement, as well as soft tissue management.[55,56] The authors feel that more extensive research has to be carried out to confirm the usefulness of laser as a technique for treatment of periodontal diseases, especially in terms of chances of recolonization of microorganisms after laser treatment as compared to other techniques used.
Chemotherapeutic agents used for the treatment of periodontal diseases
Chemotherapeutics agents used for the treatment of periodontal diseases are discussed below.
Host modulation therapy (HMT)
Clinical data obtained from the recent research has shown that the periodontal tissue degeneration is brought about by the bacterial plaque, their toxins, and the host's inflammation-immunity response to them.[8] The objective of host modulatory therapy (HMT) is to alter the host response to bring down the destruction levels.[8] Various host modulatory agents are available, namely, doxycycline at sub-antimicrobial dose, bisphosphonates, anti-inflammatory drugs, enamel matrix derivatives and growth factors. All these agents are able to modify host-response and block the destructive aspects of the immune response.[57] Anti-inflammatory drugs are able to inhibit the prostaglandins and cytokinins; tetracyclines are the collagenase inhibitors and biphosphonates reduce the osteoclast cell activity.[8] Recently, FDA approved a new therapy which involves systemic administration of drug that is to be used adjunct to scaling and root planning.[8] It involves the systemic sub antimicrobial dose of tetracycline. Periostat, 20 mg capsule of doxycycline hyclate, is the FDA approved product which is a collagenase inhibitor and marketed for oral administration.[3,8] Doxycycline hyclate is an antimicrobial agent which does not show the antibacterial activity in this dose level, but it effectively reduces the collagenase activity in patients suffering from periodontitis.[58]
Antimicrobial therapy
The most widely used methods of controlling disease progression are the mechanical methods and surgical debridement. However, they are not efficient to remove all the microbes present in the periodontal pocket and tissues. Thus, residual microbes in the periodontal milieu re-colonize after 8 weeks of treatment.[3] Therefore, adjunct use of chemotherapeutic agents along with mechanical and surgical debridement could be more effective.[3]
The bacteria are the foremost etiological factor responsible for periodontal disease, and therefore the use of antimicrobial therapy along with the mechanical therapy is a good biological rationale for the treatment of the periodontal disease. Undoubtedly, a lot of valuable effects can be achieved by the systemic antimicrobial treatment.[59]
However, currently systemic antibiotics are prescribed only for the treatment of rapidly progressing or refractory periodontitis.[44,60] Multiple dosing of systemic antibiotics involves several drawbacks, which include erratic antibiotic concentration at the targeted site,[61] a quick fall in the plasma drug concentration below the therapeutic index,[62] and development of resistance to antibiotics. Besides this, a high antibiotic dose is required which in turn causes several side effects in patients.[44] The above-mentioned apparent shortcomings of systemic antimicrobial treatment led to the development of interest in localized intra-pocket drug delivery systems for the treatment of periodontal diseases.[63–65]
LOCALIZED INTRA-POCKET DRUG DELIVERY SYSTEMS
Intra-pocket drug delivery systems are highly attractive systems due to the following advantages: less unwanted side effects, superior worth and improved patient compliance.[2] The charm of treating periodontal diseases by the localized drug delivery systems is based on the fact that they provide higher accessibility to the periodontal cavity and deliver drugs at bacteriostatic or bactericidal concentration at the targeted site for extended periods of time to generate the wanted clinical benefits.[2] The local drug delivery devices, which have been approved for the treatment of periodontal diseases, are Perio chip®, Jerusalem, Israel (2.5 mg chlorhexidine gluconate, thin solid chip system), Atridox®, Fort Collins, Colo, USA (10% doxycycline hyclate, flowable polymer syringe), Actisite®, Palo Alto CA, USA (25% tetracycline fibers) and Arestin®, Warminster, Pennsylvania (1 mg minocycline hydrochloride, microspheres syringe).
The periodontal pocket provides a natural reservoir, which is easily accessible for the insertion of a delivery device. At the site of the periodontal disease, the flow rate of gingival cravicular fluid (GCF) becomes 40 times higher than in the normal condition.[66] The GCF provides a leaching medium for the release of a drug from the dosage form and for its distribution throughout the pocket.[2] These features, together with the fact that the periodontal diseases are localized to the immediate environment of the pocket, make the periodontal pocket a natural site for treatment with local delivery systems.[2]
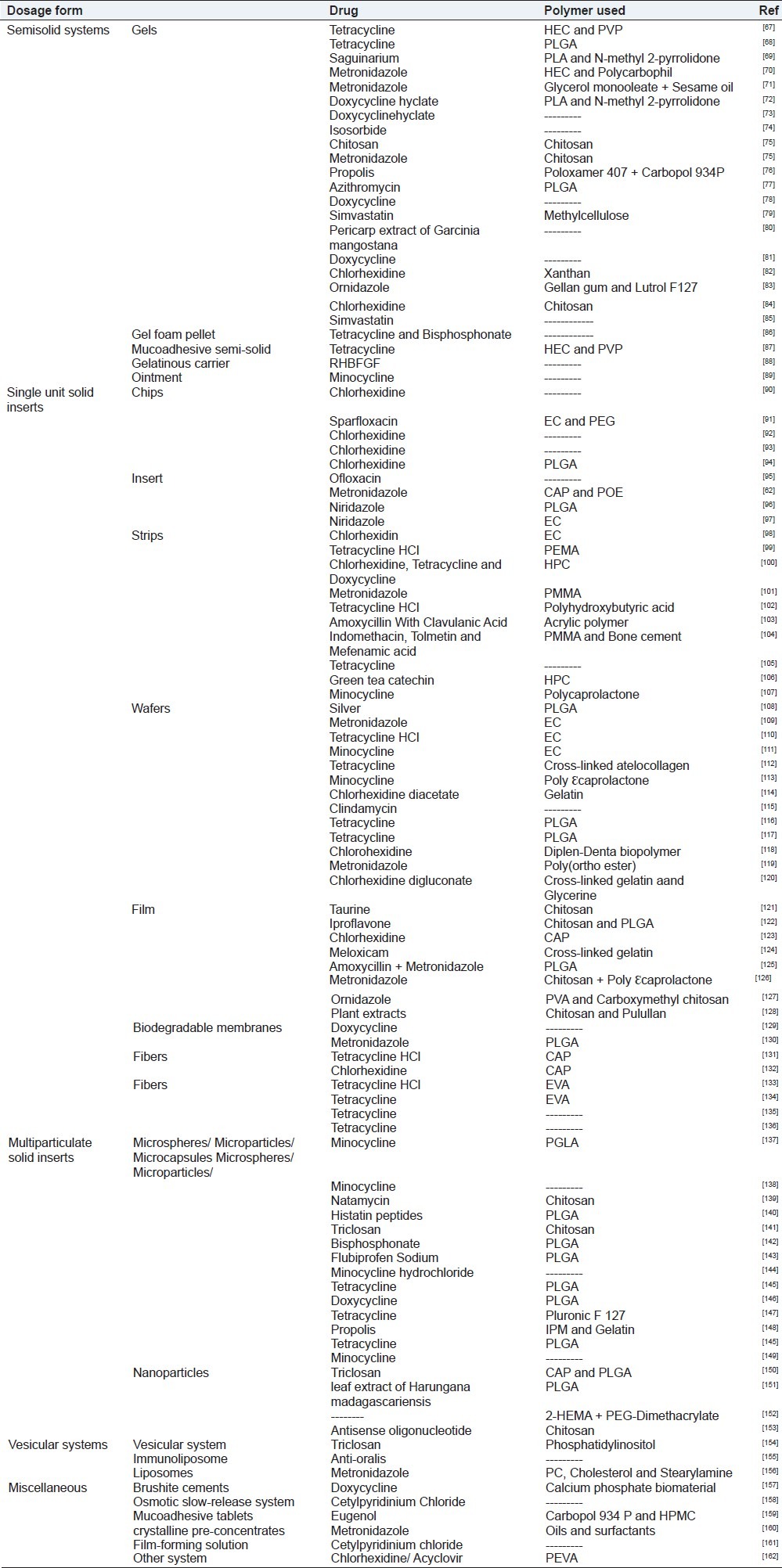
Biodegradable and biocompatible polymers of natural, synthetic or semi-synthetic origin are used for development of intrapocket drug delivery devices to meet the pharmacological and biological obligations.[2] There are various chemotherapeutic agents, studied for localized intra pocket drug delivery systems for the treatment of periodontal diseases. The chemotherapeutic agents used include antiseptics, antimicrobials, host response modulating agents such as anti-inflammatory agents, growth factors and enamel derivative matrices. Localized intra-pocket drug delivery systems along with their structural material and chemotherapeutic agent investigated for the treatment of periodontal disease are listed in Table 1.
Table 1.
Localized intra-pocket drug delivery systems investigated for the treatment of periodontal diseases
Despite the fact that localized intrapocket delivery systems are better than the conventional treatment options with regards to targeted delivery of the drug at the site of action, reduced dose, sustained drug action and patient compliance resulting from reduction in frequency of dosing, extensive clinical trials need to be carried out on the prepared dosage forms before any substantial conclusion can be drawn regarding the improved efficacy of these dosage form in long-term management of periodontitis as compared to the conventional therapies already available.
The success of a developed periodontal dosage form also depends on the choice of appropriate evaluation parameters and use of relevant techniques, which has been discussed below.
EVALUATION MODELS FOR PERIODONTAL DOSAGE FORMS
There are various methods which have been used for the evaluation of efficacy of periodontal dosage forms. These models can broadly be divided into in vitro and in vivo and microbiological models.
IN VITRO MODELS USED FOR EVALUATION OF PERIODONTAL DOSAGE FORMS
The efficacy of the delivery system depends on the release profile of drug from the formulation. In vitro release profile gives important information on the in vivo performance of the delivery system proposed for controlled release of the drugs.[163] The most excellent dissolution method for in vivo-in vitro correlation is, apparently, the method that illustrates what happens in vivo. The in vitro dissolution depends on type of formulation, manufacturing process, the characteristics of the active pharmaceutical ingredients such as the solubility and dissolution rate, apparatus, dissolution parameters and dissolution medium (volume of dissolution media, pH of media).[164] The selection of a suitable in vitro model must be done carefully so as to mimic as stringently as possible the in vivo behavior. The data obtained from the in vitro release for different parameters may be reliable and predestined.[164]
The periodontal pockets provide the reservoir for intra-pocket while gingival cravicular fluid act as a leaching medium for the release of a drug from the dosage form and its distribution throughout the pocket.[2] The characteristics of the gingival cravicular fluid, like pH, volume, flow rate and composition can influence the dissolution profile of the drug delivery systems. Small volumes of GCF (0.04 μL) and flow rate (0.03 μL/min) were observed in healthy pockets. With respect to protein concentrations, it shows the similarity with extracellular fluid and it is thought to represent a normal extracellular transudate.[165] In contrast to healthy site, the fluid production and flow rate become higher at inflamed site. However, the volume and fluid flow rate depends on the degree of inflammation at individual sites. Volumes of about 0.5 μL and flow rates of 0.5 μL/min and 0.33 μL/min have been reported by Hattingh and Ho and Goodson, respectively,[66,165] while Cimasoni reported the flow rate at an individual site to be 150-200 μL/hr (2.5-3.33 μL/min), i.e., near about 5 mL/day.[166] The pH of the gingival cravicular fluid also varies from 6.0 to 8.0 according to the extent of inflammation or severity of periodontal disease.[166,167]
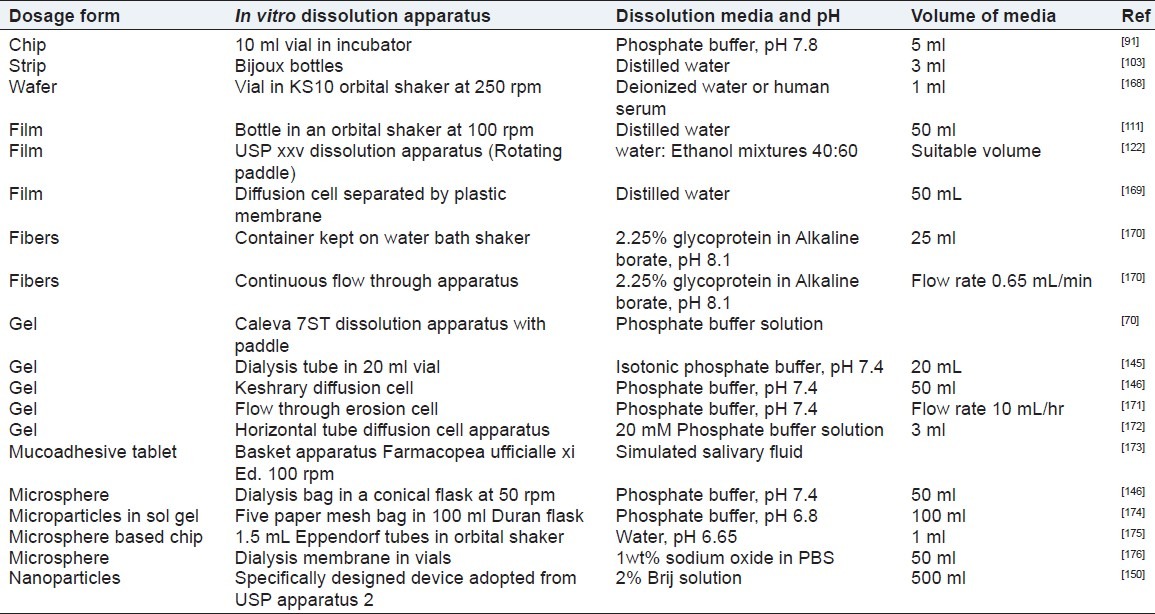
In order to mimic the inflamed periodontal cavity, selection of in vitro model, pH and composition of dissolution media are critical parameters required to achieve a good in vitro-in vivo correlation. With respect to the composition, serum rich media would mimic GCF, although, distilled water can also be a good alternative media as it has pH of 6.0-6.5 which is similar to the pH observed in the periodontal pocket at earlier stage of the periodontal disease (pH 6-7).[167] Distilled water was also chosen as an in vitro dissolution media in earlier studies with periochip.[114] Parthasarathy et al. used 10 ml vial as in vitro model and phosphate buffer pH 7.4 as the dissolution media to mimic the in vivo condition.[91] Esposito pointed out that dialysis bag could reproduce condition of a formulation applied to the periodontal cavity.[163] The various intra pocket devices employed along with their in vitro dissolution apparatus and dissolution media used to mimic the periodontal cavity are reported in Table 2.
Table 2.
In vitro models used for the evaluation of intra-pocket drug delivery systems developed for periodontal diseases
The in vitro methods used for evaluation of periodontal formulation provide a good idea of the release of the drug from the dosage form and its performance in vitro under the conditions of test. However, the exact efficacy of the dosage form cannot be interpreted correctly without performing in vivo studies in appropriate animal models. The various in vivo models used by various researchers for evaluating the efficacy of the periodontal dosage forms are discussed below.
IN VIVO MODELS USED FOR EVALUATION OF PERIODONTAL DOSAGE FORMS
There are many animals which can be and have been used to investigate the pathology of the periodontal diseases and to evaluate its treatment.[177] However, the data obtained from animal study may be valuable or controversial to humans because different species do not respond identically or even similarly to humans.[177] But the data obtained from animal studies provides a guide to go ahead for human application. Human studies have many limitations: to evaluate the pathogenesis and its treatment modalities in human studies such as finding out level of the disease, risk factors of individual and susceptibility of disease progression have to be critically studied. Therefore, animal models are required. Before selecting the animal models, consideration should be given to the human anatomy as well as at the stage of the periodontal disease. Non human primates, rats, dogs, ferrets hamsters can be used to study the different aspects of periodontal disease and treatment with some benefits and limitations.[177]
Non human primates
Considering dental formula and dental anatomy, nonhuman primates are almost similar to humans. There is no difference in histology of healthy monkey gingiva and human gingival.[177] In all the stages of gingivitis, the composition of plaque flora is also comparable to humans.[178,179] Cynomolgus monkey (Mecca fescicularis) shows similarity with inflammatory infiltrate in periodontal disease to humans which makes them an appropriate model to find out the pathogenesis of periodontitis, while Squirrel monkey (Saimiri sciureus) and marmosets show the variation in inflammatory infiltrate and these differences make them inappropriate model for the same.[179,180] Squirrel monkey is an appropriate model for the study of progressive marginal periodontitis associated with traumatic injury.[181] Marmosets are small non human primates with small cavity for periodontal procedure while the Cynomolgus and rhesus monkey (Mecca mulata) are large human primates suitable for experimentally induced periodontitis.[182,183] Periodontal regenerative procedure and histometric analysis can be done only in monkey and dog models as they require quantifying new cementum periodontal ligament and alveolar bone formation after regenerative periodontal surgery.
Caton et al. described three types of experimentally induced periodontal lesions in non-human primates.[184] In acute defect model, periodontal lesions are induced by surgical removal of bone, cementum and periodontal ligament where spontaneous regeneration of the defects occurs. The chronic defects are induced by placement of orthodontic elastics around the circumference of teeth which may take up to 6 months.[184] Deep defects are found more likely in proximal sites rather than on the facial and lingual surfaces. This model has several advantages, including rapidly-produced defects which do not heal with notable amounts of spontaneous regeneration.[184] Due to the possibility of obtaining block biopsies, the rhesus monkey, cynomolgus monkey, and baboons have been used to study osseointegrated oral implants. Ligature-induced periodontitis around teeth and ligature induced peri-implantitis follow similar destructive patterns.[185]
Although various species of non-human primates are adequate for studying different aspects of periodontal diseases, monkeys are expensive to purchase and maintain and are ferocious.[179] Wild captured monkeys can also be carriers of Mycobacterium tuberculosis, Herpes Simplex Type B, Shigella species and Simian B.[76] Monkeys are also susceptible to systemic infections and diseases, and create difficulties in controlling post-surgical infections and trauma.[177]
Rats
Rodents show the physiological change in dentination throughout the life period which leads to change in the position of teeth especially in molar teeth.[186] Epithelium and connective tissue of rats are similar to humans in regard of histology, the only difference being in sulcular epithelia which is keratinized in rat.[187] The inflammatory process in the rats is also different from humans.[188] Gnotobiotic or germfree rats are used to study oral diseases.[189] Rats showed periodontal destruction within 84 days after contamination with the Gram positive bacteria (Actinomycosus viscosus, A. israelli, streptococcus mutant) isolated from human oral cavity.[190,191] Periodontal disease in rats is different from that of humans and rats are relatively resistant to periodontal disease.[192] Rats fed a sucrose-rich diet show rapid bacterial plaque formation on molar fissure and inter dental space.[193] In the light of the above facts, it can be concluded that rat is a suitable model for calculus and carries but not for periodontal disease. It is mainly used for oral micro flora research.[192]
Hamsters
Hamsters have been used to evaluate the transmissibility of periodontal disease with plaque bacteria.[194] The disease can be induced by introducing isolates from infected hamsters into noninfectious hamsters and can be transmitted from generation to generation.[195] Hamsters infected with cariogenic Streptococci strain develop caries and extensive periodontal disease and both the conditions can be evaluated at the same time.[194] Hamsters have been used mostly for exploration of caries due to the potential of the cariogenic micro-organisms to form profuse amount of plaque and quickly develop carious lesions.[186]
Dogs
Beagle dogs are good candidates for studying periodontal disease progression, tissue regeneration, tissue wound recoveries and dental implants. Because of its humble nature, susceptibility to disease and identical pathogenesis to human,[196–198] it may also be a valuable model for experimental periodontitis. Gingival recession is a unique character in dogs with periodontitis.[197] Gingivitis in young dogs may not essentially progress into periodontitis.[199] Different age groups of dogs show the variable severity and range in gingivitis and periodontitis.[197] There are many features which govern conversion of gingivitis in to periodontitis.[200] The induced gingivitis turns into periodontitis in young dogs by allowing the plaque accumulation.[201] Ligature placement may induce the advance lesion and major tissue destruction within first 4 weeks.[202] Despite close resemblance in the character of gingivitis in dogs and humans, some difference still exists in inflammatory lesions which occur mainly in the coronal portion of connective tissue at gingival margin in dogs in contrast to humans where they occur in sulcus.[203] Much faster bone turnover rate and different architecture and thickness of bone limits the suitability of dogs for regression study.[183]
Ferrets
Ferrets have been used as a dental model and medical model.[204] King et al. 1940 pointed out the similarity in periodontal disease in humans and ferrets and reported the ferrets as an animal model.[205] The course of the periodontal lesion in them follows a similar path as in humans and tissue response characteristics in them are also identical in all respects to those found in human gingivitis.[205] Ligature-induced periodontitis can be developed in ferrets within 28 days.[206] The ferrets are a suitable model for the study of sulcus because sulcus formation is diet independent and shows resemblance with human sulcus and can be screened in living animal which is not possible in rats.[204]
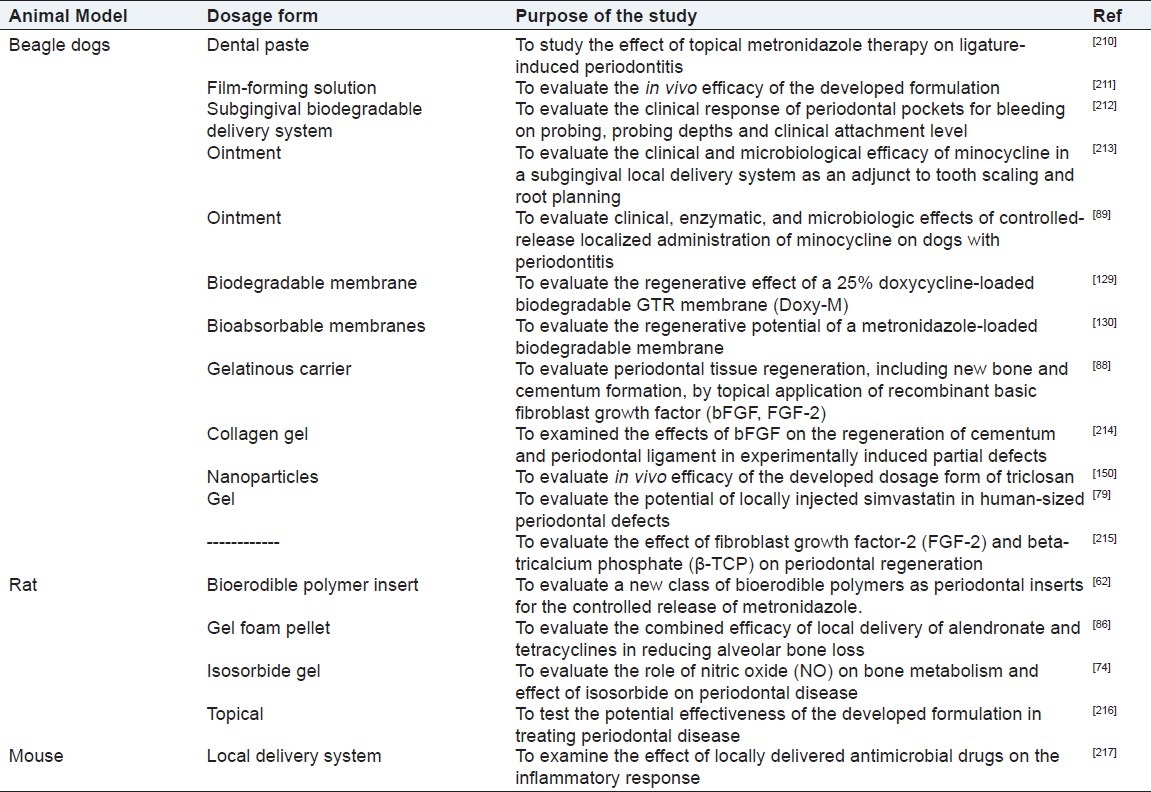
For the evaluation of the efficacy of treatment modalities of periodontal disease, various practices have been employed. Generally, the effects of treatments are evaluated by enumerating clinical improvements and changes in the subgingival microflora.[207] Clinical improvement is assessed by various indices which include, gingival and plaque index, gingival crevicular flow rate, degree of bleeding on probing, pocket depth, and attachment level.[65,208,209] The various animal models to evaluate the effectiveness of the developed dosage form for the treatment of periodontal diseases are given in Table 3.
Table 3.
Animal models used to evaluate the effectiveness of the intra-pocket delivery systems developed for the treatment of periodontal diseases
Besides the in vitro studies and in vivo studies conducted, a very important study for the evaluation of periodontal dosage form relates to the evaluation of antimicrobial activity of the prepared dosage form.
ANTIMICROBIAL MODELS USED FOR EVALUATION OF PERIODONTAL DOSAGE FORMS
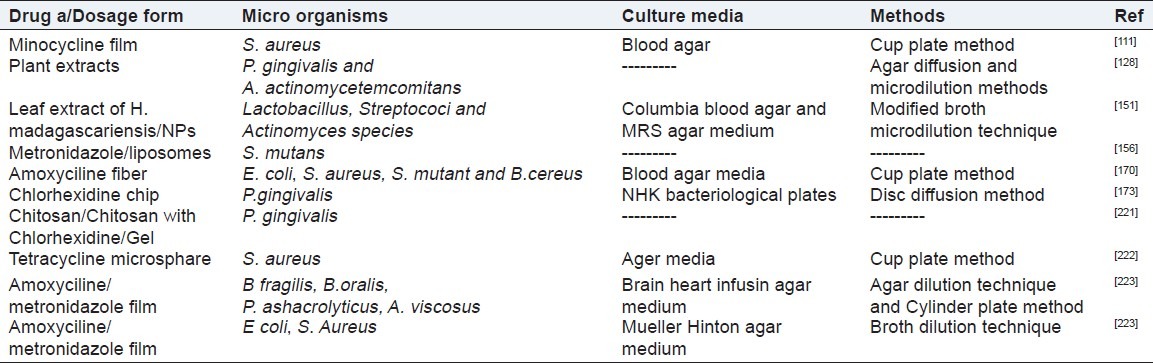
The teeth in the oral cavity are supported by four distinct structures namely gingiva, alveolar bone, cementum and periodontal ligament.[207] A shallow gingival sulcus, less than 3 mm, exists between the gingiva and tooth at healthy sites, the size of which deepens on the disease progression.[207] The healthy gingival sulcus is not free from bacteria. Gram positive bacteria can be found within the cavity. Such bacteria are compatible with the tissue and do not cause any damage.[207] The pocket deeper than 4 mm provides the anerobic environment which is an ideal condition for the development of the pathogenic bacteria[218] primarily Gram negative, facultative or obligate anerobic species, major amongst which are Bacteroides spp. Fusobacterium, Actinobacillus, and Eikenella sp.[1] A few microorganisms associated with endodontal and periodontal infections are listed in Table 4.[219,220]
Table 4.
Microbiological strain, culture media and methods employed to assess antimicrobial activity developed dosage form for periodontal disease
Evaluation from the microbiological point of view involves assessing, changes in the subgingival microflora. There are various in vitro, in vivo and microbiological models which have been studied to evaluate the efficacy of drug delivery systems.
In vitro antimicrobial study is performed to check the efficacy of the formulation against the microorganisms. Selection of the microorganisms for the study depends on the disease. The most common micro organisms, used to check the antmicrobial efficacy of the developed formulation against periododontal diseases, are Prevotella, Fusobacterium, Actinobacillus, and Eikenella spp, S. aureus, E coli and many other enlisted in Table 4. The method of microbiological study (Agar dilution technique, Broth dilution technique, Cup plate method, Turbidimetric method) depends upon the type of micro organism (aerobic or anerobic). The media chosen for the study includes that media in which the micro organism shows maximum growth. Different investigators have used different methods to check the effectiveness of the formulation by using the aliquots of the in vitro release sample collected at different time intervals[222] or by putting the dosage form directly on the media.[173] Ahuja and coworkers performed the microbiological study to see the effectiveness of dental films containing metronidazole and amoxyciline.[223] The efficacy of dental film was evaluated both by using in vitro release study samples collected at different time intervals and by directly putting dental film on periodontal pathogens. The study was carried out in anerobic condition consisting of nitrogen (80%), hydrogen (10%) and carbon dioxide (10%). The microorganisms used for the study were B. fragilis, B.oralis, P. sachrolyticus, A. viscosus and P. acne. The agar dilution technique and broth dilution technique were employed. Brain heart infusion agar media was used as the growth media for microorganisms. Similar study was also carried out in S. aureus and E. coli in aerobic condition using Mueller Hinton agar as growth media. In both studies, it was found that the in vitro released samples and dental films were able to inhibit the growth of micro organisms.[223]
The antimicrobial efficacies of tetracycline loaded microspheres and drug free microspheres were evaluated by Govender and coworkers. For the study, cup plate method was adopted and Staphylococcus aureus ATCC 29213 was chosen as the test micro-organism. The study was carried out in aerobic condition in agar media. For the evaluation purpose aliquots collected from in vitro release study of drug loaded and drug free microspheres at different time intervals were filled into the wells made into the solidified ager media plate inoculated with S. Aureus. Results indicated that drug release at different time intervals was found to be above the MIC (1 μg/ml) and effective to inhibit the growth of S. aureus.[222]
Harungana madagascariensis has been identified to have antibacterial, antifungal, and antiviral activity.[151] In vitro bactericidal activity of the H. madagascariensis leaf extract (HLE) on the oral bacterial strains is mainly implicated in dental caries and gingivitis infections.[223] The potential of HLE antibacterial effects using the poly (D, L-lactide-co-glycolide) nanoparticles [PLG-NP] was investigated.[151] Antimicrobial efficacies of Harungana leaf extract (HLE) and HLE loaded NPs were evaluated on different microorganisms using different growth media for individual microorganisms, namely Columbia blood agar for Streptococcus and Actinomyces species; MRS agar medium for Lactobacillus species; Triptych Soy agar for Fusobacterium, Prevotella and Propionibacterium species. For the purpose of this study, serial dilutions in the concentration range 5-500 μg/ml of HLE and HLE PLGA NPs were prepared in nutrient broth. 100 μl of bacterial suspension was put in the wells of microtiter plate along with 100 μl of each serial dilution of HLE or HLE PLGA NPS or HLE free PLGA NPs. Every track of the microtiter plate enclosed 100 μl bacterial suspension and 100 ml plant extract dilution, or 100 μl HLE loaded PLG-NP dilution, or HLE unloaded PLG-NP (control). Plates were incubated for 24 h at 38°C in the environment of carbon dioxide. Each track of microtiter plate was inoculated on the plates of respective media and the plates were incubated for 48 h in incubator. The antimicrobial results obtained from the study showed that HLE-PLG-NPs have a superior bactericidal activity as compared to the HLE solution against different species except the S. mutant.[151]
CONCLUSION
Periodontitis is an inflammatory disease caused primarily by the periodontal plaque bacteria, although the host immune responses also play an important role. With the advent of concept of delivery of systemic antibiotics as intrapocket devices for the treatment of periodontitis, research has been directed to develop and patent more physiologically acceptable and commercially feasible drug delivery systems as an adjunct to the conventional surgical and nonsurgical treatments for periodontal infections.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Haffajee AD, Socransky SS. Attachment level changes in destructive periodontal diseases. J Clin Periodontol. 1986;13:461–75. doi: 10.1111/j.1600-051x.1986.tb01491.x. [DOI] [PubMed] [Google Scholar]
- 2.Jain N, Jain GK, Javed S, Iqbal Z, Talegaonkar S, Ahmad FJ, et al. Recent approaches for the treatment of periodontitis. Drug Dis Today. 2008;13:932–43. doi: 10.1016/j.drudis.2008.07.010. [DOI] [PubMed] [Google Scholar]
- 3.Ryan ME. Nonsurgical approaches for the treatment of periodontal diseases. Dent Clinics North Am. 2005;49:611–36. doi: 10.1016/j.cden.2005.03.010. [DOI] [PubMed] [Google Scholar]
- 4.Socransky SS. The relationship of bacteria to the etiology of periodontal disease. J Dent Res. 1970;49:203–22. doi: 10.1177/00220345700490020401. [DOI] [PubMed] [Google Scholar]
- 5.Howell TH, Williams RC. Nonsteroidal anti-inflammatory drugs as inhibitors of periodontal disease progression. Crit Rev Oral Biol Med. 1993;4:177–96. doi: 10.1177/10454411930040020301. [DOI] [PubMed] [Google Scholar]
- 6.Loe H, Theilande E, Jensen SB. Experimental gingivitis in man. J Periodontol. 1965;36:177–87. doi: 10.1902/jop.1965.36.3.177. [DOI] [PubMed] [Google Scholar]
- 7.Heasman PA. The role of nonsteroidal anti-inflammatory drugs in the management of periodontal disease. J Dent. 1988;16:247–57. doi: 10.1016/0300-5712(88)90117-0. [DOI] [PubMed] [Google Scholar]
- 8.Oringer RJ. Research, Science, Therapy Committee of the American Academy of Periodontology. Modulation of the host response in periodontal therapy. J Periodontol. 2002;3:460–70. doi: 10.1902/jop.2002.73.4.460. [DOI] [PubMed] [Google Scholar]
- 9.Kirkwood KL, Cirelli JA, Rogers JE, Giannobill WV. Novel host response therapeutic approach to treat periodontal disease. Periodontol 2000. 2007;43:294–315. doi: 10.1111/j.1600-0757.2006.00166.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Genco RJ. Host responses in periodontal diseases: Current concepts. J Periodontol. 1992;63(Suppl. 4):338–55. doi: 10.1902/jop.1992.63.4s.338. [DOI] [PubMed] [Google Scholar]
- 11.Grossi SG, Zambon JJ, Ho AW, Ho AW, Koch G, Dunford RG, et al. Assessment of risk for periodontal disease. I. Risk indicators for attachment loss. J Periodontol. 1994;65:260–7. doi: 10.1902/jop.1994.65.3.260. [DOI] [PubMed] [Google Scholar]
- 12.Salvi GE, Lawrence HP, Offenbacher S, Beck JD. Influence of risk factors on the pathogenesis of periodontitis. Periodontol 2000. 1997;14:173–201. doi: 10.1111/j.1600-0757.1997.tb00197.x. [DOI] [PubMed] [Google Scholar]
- 13.Iqbal Z, Jain N, Jain GK, Talegaonkar S, Ahuja A, Khar RK, et al. Dental therapeutic systems. Recent Pat Drug Deliv Formulation. 2008;2:58–67. doi: 10.2174/187221108783331366. [DOI] [PubMed] [Google Scholar]
- 14.Deporter DA. Periodontal disease part II: Overview of treatment modalities. Can Fam Physician. 1988;34:1391–2. [PMC free article] [PubMed] [Google Scholar]
- 15.Freeman E. Periodontal disease part III: Chemotherapeutics. Can Fam Physician. 1988;34:1395–7. [PMC free article] [PubMed] [Google Scholar]
- 16.Krayer JW, Leite RS, Kirkwood KL. Non-surgical chemotherapeutic treatment strategies for the management of periodontal diseases. Dent Clin North Am. 2010;54:13–33. doi: 10.1016/j.cden.2009.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bader HI. Floss or die: Implications for dental professionals. Den Today. 1998;17:76–82. [PubMed] [Google Scholar]
- 18.Oliver RC, Brown LJ, Loe H. Periodontal diseases in the United States population. J Periodontol. 1998;69:269–78. doi: 10.1902/jop.1998.69.2.269. [DOI] [PubMed] [Google Scholar]
- 19.Newman MG, Cattabriga M, Etienne D, Flemmig T, Sanz M, Kornman KS, et al. Effectiveness of adjunctive irrigation in early periodontitis. Multi-center evaluation. J Periodontol. 1994;65:224–9. doi: 10.1902/jop.1994.65.3.224. [DOI] [PubMed] [Google Scholar]
- 20.Fleming TF, Epp B, Funkenhauser Z, Newman MG, Korman KS, Haubitz I, et al. Adjunctive supragingival irrigation with acetylsalicylic acid in periodontal supportive therapy. J Clin Periodontol. 1995;22:427–33. doi: 10.1111/j.1600-051x.1995.tb00173.x. [DOI] [PubMed] [Google Scholar]
- 21.Brightman LJ, Terezhalmy GT, Greenwell H, Jacobs M, Enlow DH. The effects of a 0.12% chlorhexidine gluconate mouthrinse on orthodontic patients aged 11 through 17 with established gingivitis. Am J Orthod Dentofacial Orthop. 1991;100:324–9. doi: 10.1016/0889-5406(91)70069-9. [DOI] [PubMed] [Google Scholar]
- 22.Pitts G, Brogdon C, Hu L, Masurat T, Pianotti R, Schumann P. Mechanism of action of an antiseptic, anti-order mouthwash. J Dent Res. 1983;62:738–42. doi: 10.1177/00220345830620061001. [DOI] [PubMed] [Google Scholar]
- 23.De Boever EH, Loesche WJ. Assessing the contribution of anaerobic microflora of the tongue to oral malador. J Am Dent Assoc. 1995;126:1384–93. doi: 10.14219/jada.archive.1995.0049. [DOI] [PubMed] [Google Scholar]
- 24.Ciancio SG, Lauciello F, Shibly O, Vitello M, Mather M. The effect of an antiseptic mouthrinse on implant maintenance: Plaque and peri-implant gingival tissues. J Periodontol. 1995;66:962–5. doi: 10.1902/jop.1995.66.11.962. [DOI] [PubMed] [Google Scholar]
- 25.Greenstein G. Effects of subgingival irrigation on periodontal status. J Periodontol. 1987;58:827–36. doi: 10.1902/jop.1987.58.12.827. [DOI] [PubMed] [Google Scholar]
- 26.Shiloah J, Hovious LA. The role of subgingival irrigations in the treatment of periodontitis. J Periodontol. 1993;64:835–43. doi: 10.1902/jop.1993.64.9.835. [DOI] [PubMed] [Google Scholar]
- 27.Lang NP, Raber K. Use of oral irrigators as vehicles for the application of antimicrobial agents in chemical plaque control. J Clin Periodontol. 1981;8:177–88. doi: 10.1111/j.1600-051x.1981.tb02029.x. [DOI] [PubMed] [Google Scholar]
- 28.Lang NP, Ramseir-Grossman K. Optimal dosage of chlorhexidine digluconate in chemical plaque control when applied by an oral irrigator. J Clin Periodontol. 1981;8:189–202. doi: 10.1111/j.1600-051x.1981.tb02030.x. [DOI] [PubMed] [Google Scholar]
- 29.Flemmig TG, Newman MG, Doherty FM, Grossman E, Meckel AH, Bakdash MB. Supragingival irrigation with 0.06% chlorhexidine in naturally occuring gingivitis. I. 6 month clinical observations. J Periodontol. 1990;61:112–7. doi: 10.1902/jop.1990.61.2.112. [DOI] [PubMed] [Google Scholar]
- 30.Boyd RL, Hollander BN, Eakle WS. Comparison of subgingivally placed cannula oral irrigator tip with a supragingivally placed standard irrigator tip. J Clin Periodontol. 1992;19:340–4. doi: 10.1111/j.1600-051x.1992.tb00656.x. [DOI] [PubMed] [Google Scholar]
- 31.Greenstein G. Effects of subgingival irrigation on periodontal status. J Periodontol. 1987;58:827–36. doi: 10.1902/jop.1987.58.12.827. [DOI] [PubMed] [Google Scholar]
- 32.Greenstein G. Research, Science and Therapy Committee of the American Academy of Periodontology. The Role of supra- and subgingival irrigation in the treatment of periodontal diseases. J Periodontol. 2005;76:2015–27. doi: 10.1902/jop.2005.76.11.2015. [DOI] [PubMed] [Google Scholar]
- 33.Listgarten MA, Grossberg D, Schwimer C, Vito A, Gaffar A. Effect of subgingival irrigation with tetrapotassium peroxydiphosphate on scaled and untreated periodontal pockets. J Periodontol. 1989;60:4–11. doi: 10.1902/jop.1989.60.1.4. [DOI] [PubMed] [Google Scholar]
- 34.Southard SR, Drisko CL, Killoy WJ, Cobb CM, Tira DE. The effects of 2% chlorhexidine digluconate irrigation on the levels of Bacteroides gingivalis in periodontal pockets. J Periodontol. 1989;60:302–9. doi: 10.1902/jop.1989.60.6.302. [DOI] [PubMed] [Google Scholar]
- 35.Lander PE, Newcomb GM, Seymour GJ, Powell RN. The antimicrobial and clinical effects of a single subgingival irrigation of chlorhexidine in advanced periodontal lesions. J Clin Periodontol. 1986;13:74–80. doi: 10.1111/j.1600-051x.1986.tb01417.x. [DOI] [PubMed] [Google Scholar]
- 36.Watts EA, Newman HN. Clinical effects on chronic periodontis of a simplified system of oral hygiene including subgingival pulsated jet irrigation with chlorhexidine. J Clin Periodontol. 1986;13:666–70. doi: 10.1111/j.1600-051x.1986.tb00863.x. [DOI] [PubMed] [Google Scholar]
- 37.MacAlpine R, Magnusson I, Kiger R, Crigger M, Garrett S, Egelberg J. Antimicrobial irrigation of deep pockets to supplement oral hygiene instruction and root debridement. I. Biweekly irrigation. J Clin Periodontol. 1985;12:568–77. doi: 10.1111/j.1600-051x.1985.tb01390.x. [DOI] [PubMed] [Google Scholar]
- 38.Marsh PD. Dental plaque as a biofilm and a microbial community-implications for health and disease. BMC Oral Health. 2006;6(Suppl. 1):S14. doi: 10.1186/1472-6831-6-S1-S14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Giusto T. Non-surgical vs. surgical periodontal therapy. New York, USA: SUNY Stonybrook; 1997. p. 1. [Google Scholar]
- 40.Cobb CM. Non-surgical pocket therapy: Mechanical. Ann Periodontol. 1996;1:443–90. doi: 10.1902/annals.1996.1.1.443. [DOI] [PubMed] [Google Scholar]
- 41.Obeid PR, D’Hoore W, Bercy P. Comparative clinical responses related to the use of various periodontal instrumentation. J Clin Periodontol. 2004;31:193–9. doi: 10.1111/j.0303-6979.2004.00467.x. [DOI] [PubMed] [Google Scholar]
- 42.Serino G, Rosling B, Ramberg P, Socransky SS, Lindhe J. Initial outcome and longterm effect of surgical and nonsurgical treatment of advanced periodontal disease. J Clin Periodontol. 2001;28:910–6. doi: 10.1034/j.1600-051x.2001.028010910.x. [DOI] [PubMed] [Google Scholar]
- 43.Cugini MA, Haffajee AD, Smith C, Kent RL, Jr, Socransky SS. The effect of scaling and root planing on the clinical and microbiological parameters of periodontal diseases: 12-month results. J Clin Periodontol. 2000;27:30–6. doi: 10.1034/j.1600-051x.2000.027001030.x. [DOI] [PubMed] [Google Scholar]
- 44.Slots J, Rams TE. Antibiotics in periodontal therapy: Advantages and disadvantages. J Clin Periodontol. 1990;17:479–93. doi: 10.1111/j.1365-2710.1992.tb01220.x. [DOI] [PubMed] [Google Scholar]
- 45.Clifford LR, Needleman IG, Chan YK. Comparison of periodontal pocket penetration by conventional and microultrasonic insets. J Clin Periodontol. 1999;26:124–30. doi: 10.1034/j.1600-051x.1999.260210.x. [DOI] [PubMed] [Google Scholar]
- 46.D’Ercole S, Piccolomini R, Capaldo G, Catamo G, Perinetti G, Guida L. Effectiveness of ultrasonic instruments in the therapy of severe periodontitis: A comparative clinical-microbiological assessment with curettes. New Microbiol. 2006;29:101–10. [PubMed] [Google Scholar]
- 47.Kishida M, Sato S, Ito K. Effects of a new ultra-sonicscaler on fibroblast attachment to root surfaces: A scanning electron microscopy analysis. J Periodontal Res. 2004;39:111–9. doi: 10.1111/j.1600-0765.2004.00715.x. [DOI] [PubMed] [Google Scholar]
- 48.Cobb CM. Clinical significance of non-surgical periodontal therapy: An evidence-based perspective of scaling and root planing. J Clin Periodontol. 2002;29(Suppl. 2):6–16. [PubMed] [Google Scholar]
- 49.Sculean A, Schwarz F, Berakdar M, Romanos GE, Brecx M, Willershausen B. Non-surgical periodontal treatment with a new ultrasonic device (Vector-ultrasonic system) or hand instruments. J Clin Periodontol. 2004;31:428–33. doi: 10.1111/j.1600-051X.2004.00496.x. [DOI] [PubMed] [Google Scholar]
- 50.Goodson JM, Tanner A, McArdle S, Dix K, Watanabe SM. Multicentre evaluation of tetracycline fibre therapy. III. Microbiological response. J Periodontal Res. 1991;26:440–51. doi: 10.1111/j.1600-0765.1991.tb01734.x. [DOI] [PubMed] [Google Scholar]
- 51.Harper DS, Robinson PJ. Correlation of histometric, microbial and clinical indicators of periodontal disease indicators status before and after root planning. J Clin Periodontal. 1987;14:190–6. doi: 10.1111/j.1600-051x.1987.tb00966.x. [DOI] [PubMed] [Google Scholar]
- 52.Koshy G, Corbet EF, Ishikawa I. A full-mouth disinfection approach to nonsurgical periodontal therapy and prevention of reinfection from bacterial reservoirs. Periodontol 2000. 2004;36:166–78. doi: 10.1111/j.1600-0757.2004.03678.x. [DOI] [PubMed] [Google Scholar]
- 53.Teughels W, Dekeyser C, Van Essche M, Quirynen M. One-stage, full-mouth disinfection: Fiction or reality? Periodontol 2000. 2009;50:39–51. doi: 10.1111/j.1600-0757.2008.00292.x. [DOI] [PubMed] [Google Scholar]
- 54.Swierkot K, Nonnenmacher CI, Mutters R, Flores-de-Jacoby L, Mengel R. One-stage full-mouth disinfection versus quadrant and full-mouth root planning. J Clin Periodontol. 2009;36:240–9. doi: 10.1111/j.1600-051X.2008.01368.x. [DOI] [PubMed] [Google Scholar]
- 55.Aoki A, Sasaki KM, Watanabe H, Ishikawa I. Lasers in nonsurgical periodontal therapy. Periodontol 2000. 2004;36:59–97. doi: 10.1111/j.1600-0757.2004.03679.x. [DOI] [PubMed] [Google Scholar]
- 56.Matthews DC. Seeing the light-the truth about soft tissue lasers and nonsurgical periodontal therapy. J Can Dent Assoc. 2010;76:a30. [PubMed] [Google Scholar]
- 57.Rajababu P, Reddy Harinath S, Satyanarayana D, Kumar Sunil P. Non surgical periodontal therapy. Ind J Dent Adv. 2009;1:16–9. [Google Scholar]
- 58.Preshaw PM, Hefti AF, Jepsen S, Etienne D, Walker C, Bradshaw MH. Subantimicrobial dose doxycycline as adjunctive treatment for periodontitis. A review. J Clin Periodontol. 2004;31:697–707. doi: 10.1111/j.1600-051X.2004.00558.x. [DOI] [PubMed] [Google Scholar]
- 59.Slots J, Pallasch TJ. Dentist's role in halting antimicrobial resistance. J Dent Res. 1996;75:1338–41. doi: 10.1177/00220345960750060201. [DOI] [PubMed] [Google Scholar]
- 60.Vandekerckhove BN, Quirynen M, van Steenberghe D. The use of tetracycline-containing controlled release fibres in the treatment of refractory periodontitis. J Periodontol. 1997;68:353–61. doi: 10.1902/jop.1997.68.4.353. [DOI] [PubMed] [Google Scholar]
- 61.Pitcher GR, Newman HN, Strahan JD. Access to subgingival plaque by disclosing agents using mouthrinsing and direct irrigation. J Clin Periodontol. 1980;7:300–8. doi: 10.1111/j.1600-051x.1980.tb01972.x. [DOI] [PubMed] [Google Scholar]
- 62.Gates KA, Grad H, Birek P, Lee PI. A new bioerodible polymer insert for a controlled release of metronidazole. Pharm Res. 1994;11:1605–9. doi: 10.1023/a:1018913921956. [DOI] [PubMed] [Google Scholar]
- 63.Greenstein G. Local drug delivery in the treatment of periodontal diseases: Assessing the clinical significance of the results. J Periodontol. 2006;77:565–78. doi: 10.1902/jop.2006.050140. [DOI] [PubMed] [Google Scholar]
- 64.Listgarten MA, Lindhe J, Hellden L. Effect of tetracycline and or scaling on human periodontal disease, Clinical, microbiological and histological observations. J Clin Periodontol. 1978;5:246–71. doi: 10.1111/j.1600-051x.1978.tb01918.x. [DOI] [PubMed] [Google Scholar]
- 65.Lindhe J, Liljenberg B, Adielsson B. Effect of long-term tetracycline therapy on human periodontal disease. J Clin Periodontol. 1983;10:590–601. doi: 10.1111/j.1600-051x.1983.tb01297.x. [DOI] [PubMed] [Google Scholar]
- 66.Goodson JM. Pharmacokinetic principles controlling efficacy of oral therapy. J Dent Res. 1989;68:1625–32. [Google Scholar]
- 67.Jones DS, Woolfson AD, Djokic J, Coulter WA. Development and mechanical characterization of bioadhesive semi-solid, polymeric systems containing tetracycline for the treatment of periodontal diseases. Pharm Res. 1996;13:1734–8. doi: 10.1023/a:1016413428473. [DOI] [PubMed] [Google Scholar]
- 68.Maze GI, Reinhardt RA, Payne JB, Maze C, Baker RA, Bouwsma OJ, et al. Gingival fluid tetracycline release from bioerodible gels. J Clin Periodontol. 1996;23:133–6. doi: 10.1111/j.1600-051x.1996.tb01815.x. [DOI] [PubMed] [Google Scholar]
- 69.Polson AM, Stoller NH, Hanes PJ, Bandt CL, Garrett S, Southard GL. Two multi-center trials assessing the clinical efficacy of 5% sanguinarine in a biodegradable drug delivery system. J Clin Periodotol. 1996;23:782–8. doi: 10.1111/j.1600-051x.1996.tb00610.x. [DOI] [PubMed] [Google Scholar]
- 70.Jones DS, Woolfson AD, Brown AF, O’neill MJ. Mucoadhesive, syringeable drug delivery systems for controlled application of metronidazole to the periodontal pocket: In vitro release kinetics, syringeability, mechanical and mucoadhesive properity. J Control Rel. 1997;49:71–9. [Google Scholar]
- 71.Noyan U, Yilmaz S, Kuru B, Kadir T, Acar O, Büget E. A clinical and microbiological evaluation of systemic and local metronidazole delivery in adult periodontitis patients. J Clin Periodontol. 1997;24:158–65. doi: 10.1111/j.1600-051x.1997.tb00485.x. [DOI] [PubMed] [Google Scholar]
- 72.Polson AM, Garrett S, Stoller NH, Bandt CL, Hanes PJ, Killoy WJ, et al. Multi-center comparative evaluation of subgingivally delivered sanguinarine and doxycycline in the treatment of periodontitis. II. Clinical results. J Periodontol. 1997;68:119–26. doi: 10.1902/jop.1997.68.2.119. [DOI] [PubMed] [Google Scholar]
- 73.Wolinsky LE, Camargo PM, Polson A, Ryder M, Garrett S. The significance of prior mechanical therapy for changes of periodontal status achieved by local delivery of a doxycyclinehyclate containing gel. J Clin Periodotol. 2001;28:1115–20. doi: 10.1034/j.1600-051x.2001.281205.x. [DOI] [PubMed] [Google Scholar]
- 74.Leitão RF, Rocha FA, Chaves HV, Lima V, Cunha FQ, Ribeiro RA, et al. Locally applied isosorbide decreases bone resorption in experimental periodontitis in rats. J Periodontol. 2004;75:1227–32. doi: 10.1902/jop.2004.75.9.1227. [DOI] [PubMed] [Google Scholar]
- 75.Akncbay H, Senel S, Ay ZY. Application of chitosan gel in the treatment of chronic periodontitis. J Biomed Mat Res Part B. J Biomed Mater Res B Appl Biomater. 2007;80:290–6. doi: 10.1002/jbm.b.30596. [DOI] [PubMed] [Google Scholar]
- 76.Bruschi ML, Jones DS, Panzeri H, Gremião MP, de Freitas O, Lara EH. Semisolid systems containing propolis for the treatment of periodontal disease: In vitro release kinetics, syringeability, rheological, textural, and mucoadhesive properties. J Pharm Sci. 2007;96:2074–89. doi: 10.1002/jps.20843. [DOI] [PubMed] [Google Scholar]
- 77.Pradeep AR, Sagar SV, Daisy H. Clinical and microbiologic effects of subgingivally delivered 0.5% azithromycin in the treatment of chronic periodontitis. J Periodontol. 2008;79:2125–35. doi: 10.1902/jop.2008.070589. [DOI] [PubMed] [Google Scholar]
- 78.Bogren A, Teles RP, Torresyap G, Haffajee AD, Socransky SS, Wennström JL. Locally delivered doxycycline during supportive periodontal therapy: A 3-year study. J Periodontol. 2008;79:827–35. doi: 10.1902/jop.2008.070515. [DOI] [PubMed] [Google Scholar]
- 79.Morris MS, Lee Y, Lavin MT, Giannini PJ, Schmid MJ, Marx DB, et al. Injectable simvastatin in periodontal defects and alveolar ridges: Pilot studies. J Periodontol. 2008;79:1465–73. doi: 10.1902/jop.2008.070659. [DOI] [PubMed] [Google Scholar]
- 80.Rassameemasmaung S, Sirikulsathean A, Amornchat C, Maungmingsook P, Rojanapanthu P, Gritsanaphan W. Topical application of Garcinia mangostana L. pericarp gel as an adjunct to periodontal treatment. Complement Ther Med. 2008;16:262–7. doi: 10.1016/j.ctim.2007.12.004. [DOI] [PubMed] [Google Scholar]
- 81.Tomasi C, Koutouzis T, Wennström JL. Locally delivered doxycycline as an adjunct to mechanical debridement at retreatment of periodontal pockets. J Periodontol. 2008;79:431–9. doi: 10.1902/jop.2008.070383. [DOI] [PubMed] [Google Scholar]
- 82.Paolantonio M, D’Ercole S, Pilloni A, D’Archivio D, Lisanti L, Graziani F, et al. Clinical, microbiologic, and biochemical effects of subgingival administration of a Xanthan-based chlorhexidine gel in the treatment of periodontitis: A randomized multicenter trial. J Periodontol. 2009;80:1479–92. doi: 10.1902/jop.2009.090050. [DOI] [PubMed] [Google Scholar]
- 83.Dabhi MR, Nagori SA, Gohel MC, Parikh RK, Sheth NR. Formulation development of smart gel periodontal drug delivery system for local delivery of chemotherapeutic agents with application of experimental design. Drug Deliv. 2010;17:520–31. doi: 10.3109/10717544.2010.490247. [DOI] [PubMed] [Google Scholar]
- 84.Ji QX, Zhao QS, Deng J, Lü R. A novel injectable chlorhexidine thermosensitive hydrogel for periodontal application: Preparation, antibacterial activity and toxicity evaluation. J Mater Sci Mater Med. 2010;21:2435–42. doi: 10.1007/s10856-010-4098-1. [DOI] [PubMed] [Google Scholar]
- 85.Pradeep AR, Thorat MS. Clinical effect of subgingivally delivered simvastatin in the treatment of patients with chronic periodontitis: A randomized clinical trial. J Periodontol. 2010;81:214–22. doi: 10.1902/jop.2009.090429. [DOI] [PubMed] [Google Scholar]
- 86.Yaffe A, Herman A, Bahar H, Binderman I. Combined local application of tetracycline and bisphosphonate reduces alveolar bone resorption in rats. J Periodontol. 2003;74:1038–42. doi: 10.1902/jop.2003.74.7.1038. [DOI] [PubMed] [Google Scholar]
- 87.Jones DS, Woolfson AD, Brown AF, Coulter WA, McClelland C, Irwin CR. Design, characterisation and preliminary clinical evaluation of a novel mucoadhesive topical formulation containing tetracycline for the treatment of periodontal disease. J Control Release. 2000;67:357–68. doi: 10.1016/s0168-3659(00)00231-5. [DOI] [PubMed] [Google Scholar]
- 88.Murakami S, Takayama S, Kitamura M, Shimabukuro Y, Yanagi K, Ikezawa K, et al. Recombinant human basic fibroblast growth factor (bFGF) stimulates periodontal regeneration in class II furcation defects created in beagle dogs. J Periodontal Res. 2003;38:97–103. doi: 10.1034/j.1600-0765.2003.00640.x. [DOI] [PubMed] [Google Scholar]
- 89.Hirasawa M, Hayashi K, Takada K. Measurement of peptidase activity and evaluation of effectiveness of administration of minocycline for treatment of dogs with periodontitis. Am J Vet Res. 2000;11:1349–52. doi: 10.2460/ajvr.2000.61.1349. [DOI] [PubMed] [Google Scholar]
- 90.Azmak N, Atilla G, Luoto H, Sorsa T. The effect of subgingival controlled-release delivery of chlorhexidine chip on clinical parameters and matrix metalloproteinase-8 levels in gingival crevicular fluid. J Periodontol. 2002;73:608–15. doi: 10.1902/jop.2002.73.6.608. [DOI] [PubMed] [Google Scholar]
- 91.Parthasarathy V, Manavalan R, Mythili R, Siby CT, Jeya M. Ethyl cellulose and polyethylene glycol-based sustained-release sparfloxacin chip: An alternative therapy for advanced periodontitis. Drug Dev Ind Pharm. 2002;28:849–62. doi: 10.1081/ddc-120005631. [DOI] [PubMed] [Google Scholar]
- 92.Kasaj A, Chiriachide A, Willershausen B. The adjunctive use of a controlled-release hlorhexidine chip following treatment with a new ultrasonic device in supportive periodontal therapy: A prospective, controlled clinical study. Int J Dent Hyg. 2007;5:225–31. doi: 10.1111/j.1601-5037.2007.00255.x. [DOI] [PubMed] [Google Scholar]
- 93.Duarte Fde F, Lotufo RF, Pannuti CM. Local delivery of chlorhexidine gluconate in patients with aggressive periodontitis. J Int Acad Periodontol. 2008;10:31–5. [PubMed] [Google Scholar]
- 94.Paolantonio M, D’Angelo M, Grassi RF, Perinetti G, Piccolomini R, Pizzo G, et al. Clinical and microbiologic effects of subgingival controlled-release delivery of chlorhexidine chip in the treatment of periodontitis: A multicenter study. J Periodontol. 2008;79:271–82. doi: 10.1902/jop.2008.070308. [DOI] [PubMed] [Google Scholar]
- 95.Yamagami H, Takamori A, Sakamoto T, Okada H. Intrapocket chemotherapy in adult periodontitis using a new controlled-release insert containing ofloxacin (PT-01) J Periodontol. 1992;63:2–6. doi: 10.1902/jop.1992.63.1.2. [DOI] [PubMed] [Google Scholar]
- 96.Barat R, Srinatha A, Pandit JK, Ridhurkar D, Balasubramaniam J, Mittal N, et al. Niridazole biodegradable inserts for local long-term treatment of periodontitis: Possible new life for an orphan drug. Drug Deliv. 2006;13:365–73. doi: 10.1080/10717540500398126. [DOI] [PubMed] [Google Scholar]
- 97.Barat R, Srinatha A, Pandit JK, Mittal N, Anupurba S. Ethylcellulose inserts of an orphan drug for periodontitis: Preparation, in vitro, and clinical studies. Drug Deliv. 2007;14:531–8. doi: 10.1080/10717540701606517. [DOI] [PubMed] [Google Scholar]
- 98.Friedman M, Golomb G. New sustained release dosage form of chlorhexidine for dental use. J Periodontal Res. 1982;17:323–8. doi: 10.1111/j.1600-0765.1982.tb01160.x. [DOI] [PubMed] [Google Scholar]
- 99.Addy M, Langeroudi M. Comparison of the immediate effects on the sub-gingival microflora of acrylic strips containing 40% chlorhexidine, metronidazole or tetracycline. J Clin Periodontol. 1984;11:379–86. doi: 10.1111/j.1600-051x.1984.tb01336.x. [DOI] [PubMed] [Google Scholar]
- 100.Noguchi T, Izumizawa K, Fukuda M, Kitamura S, Suzuki Y, Ikura H. New method for local drug delivery using resorbable base material in periodontal therapy. Bull Tokyo Med Dent Univ. 1984;31:145–53. [PubMed] [Google Scholar]
- 101.Addy M, Hassan H, Moran J, Wade W, Newcombe R. Use of antimicrobial containing acrylic strips in the treatment of chronic periodontal disease. A three month follow-up study. J Periodontol. 1988;59:557–64. doi: 10.1902/jop.1988.59.9.557. [DOI] [PubMed] [Google Scholar]
- 102.Deasy PB, Collins AE, MacCarthy DJ, Russell RJ. Use of strips containing tetracycline hydrochloride or metronidazole for the treatment of advanced periodontal disease. J Pharm Pharmacol. 1989;41:694–9. doi: 10.1111/j.2042-7158.1989.tb06343.x. [DOI] [PubMed] [Google Scholar]
- 103.Fanas Abu SH, Drucker DB, Hull PS. Evaluation of acrylic strips containing amoxycillin with clavulanic acid for local drug delivery. J Dent. 1991;19:92–6. doi: 10.1016/0300-5712(91)90096-h. [DOI] [PubMed] [Google Scholar]
- 104.Corry D, Moran J. Assessment of acrylic bone cement as a local delivery vehicle for the application of non-steroidal anti-inflammatory drugs. Biomaterials. 1998;19:1295–301. doi: 10.1016/s0142-9612(98)00012-x. [DOI] [PubMed] [Google Scholar]
- 105.Friesen LR, Williams KB, Krause LS, Killoy WJ. Controlled local delivery of tetracycline with polymer strips in the treatment of periodontitis. J Periodontol. 2002;73:13–9. doi: 10.1902/jop.2002.73.1.13. [DOI] [PubMed] [Google Scholar]
- 106.Hirasawa M, Takada K, Makimura M, Otake S. Improvement of periodontal status by green tea catechin using a local delivery system: A clinical pilot study. J Periodontal Res. 2002;37:433–8. doi: 10.1034/j.1600-0765.2002.01640.x. [DOI] [PubMed] [Google Scholar]
- 107.Leung WK, Jin L, Yau JY, Sun Q, Corbet EF. Microflora cultivable from minocycline strips placed in persisting periodontal pockets. Arch Oral Biol. 2005;50:39–48. doi: 10.1016/j.archoralbio.2004.08.002. [DOI] [PubMed] [Google Scholar]
- 108.Bromberg LE, Braman VM, Rothstein DM, Spacciapoli P, O’Connor SM, Nelson EJ, et al. Sustained release of silver from periodontal wafers for treatment of periodontitis. J Control Release. 2000;31:63–72. doi: 10.1016/s0168-3659(00)00233-9. [DOI] [PubMed] [Google Scholar]
- 109.Golomb G, Friedman M, Soskolne A, Stabholz A, Sela MN. Sustained release device containing metronidazole for periodontal use. J Dent Res. 1984;63:1149–53. doi: 10.1177/00220345840630091101. [DOI] [PubMed] [Google Scholar]
- 110.Azoury R, Elkayam R, Friedman M. Nuclear magnetic resonance study of an ethyl cellulose sustained-release delivery system. II. Release rate behavior of tetracycline. J Pharm Sci. 1988;77:428–31. doi: 10.1002/jps.2600770515. [DOI] [PubMed] [Google Scholar]
- 111.Elkayam R, Friedman M, Stabholz A, Soskolne AW, Sela MN, Golub L. Sustained release device containing minocycline for local treatment of periodontal disease. J Control Release. 1988;7:231–6. [Google Scholar]
- 112.Minabe M, Uematsu A, Nishijima K, Tomomatsu E, Tamura T, Hori T, et al. Application of a local drug delivery system to periodontal therapy. I. Development of collagen preparations with immobilized tetracycline. J Periodontol. 1989;60:113–7. doi: 10.1902/jop.1989.60.2.113. [DOI] [PubMed] [Google Scholar]
- 113.Kyun KD, Yun KS, Young JS, Pyoung CC, Heui SS. Development of minocycline containing polycaprolactone film as a local drug delivery. Taehan Chikkwa Uisa Hyophoe Chi. 1990;28:279–90. [PubMed] [Google Scholar]
- 114.Steinberg D, Friedman M, Soskolne A, Sela MN. A new degradable controlled release device for treatment of periodontal disease: In vitro release study. J Periodontol. 1990;61:393–8. doi: 10.1902/jop.1990.61.7.393. [DOI] [PubMed] [Google Scholar]
- 115.Higashi K, Matsushita M, Morisaki K, Hayashi S, Mayumi T. Local drug delivery systems for the treatment of periodontal disease. J Pharmacobiodyn. 1991;14:72–81. doi: 10.1248/bpb1978.14.72. [DOI] [PubMed] [Google Scholar]
- 116.Agarwal RK, Robinson DH, Maze GI, Reinhardt RA. Development and characterization of tetracycline–poly (lactide/glycolide) films for treatment of periodontitis. J Control Release. 1993;23:137–46. [Google Scholar]
- 117.Maze GI, Reinhardt RA, Agarwal RK, Dyer JK, Robinson DH, DuBoism LM, et al. Response to intracrevicular controlled delivery of 25% tetracycline from poly(lactide/glycolide) film strips in SPT patients. J Clin Periodontol. 1995;22:860–7. doi: 10.1111/j.1600-051x.1995.tb01785.x. [DOI] [PubMed] [Google Scholar]
- 118.Dedeian VR, Solov’eva NI, Ezikian TI, Medvedeva IA. The treatment of periodontal diseases using Diplen-Denta films with chlorhexidine (a clinico-laboratory study) Stomatologiia (Mosk) 1997;76:18–22. [PubMed] [Google Scholar]
- 119.Vasavada RC, Junnarkar GH. Release of metronidazole from poly (ortho ester) matrices. Proc. Int Symp Controlled Release Bioact Mater. 1997;24:499–500. [Google Scholar]
- 120.Goffin G. Efficacy of sustained local delivery of chlorhexidine Periochip as an adjuvant to scaling and root planning in the treatment of chronic periodontal disease. Int Dent Rev. 1998;18:1–18. [Google Scholar]
- 121.Ozmeriç N, Ozcan G, Haytaç CM, Alaaddinoğlu EE, Sargon MF, Senel S. Chitosan film enriched with an antioxidant agent, taurine, in fenestration defects. J Biomed Mater Res. 2000;51:500–3. doi: 10.1002/1097-4636(20000905)51:3<500::aid-jbm26>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 122.Perugini P, Genta I, Conti B, Modena T, Pavanetto F. Periodontal delivery of ipriflavone: New chitosan/PLGA film delivery system for a lipopholc drug. Int J Pharm. 2003;252:1–9. doi: 10.1016/s0378-5173(02)00602-6. [DOI] [PubMed] [Google Scholar]
- 123.Cetin EO, Buduneli N, Atlihan E, Kirilmaz L. In vitro studies on controlled-release cellulose acetate films for local delivery of chlorhexidine, indomethacin, and meloxicam. J Clin Periodontol. 2004;31:1117–21. doi: 10.1111/j.1600-051X.2004.00620.x. [DOI] [PubMed] [Google Scholar]
- 124.Cetin EO, Buduneli N, Atlihan E, Kirilmaz L. In vitro studies of a degradable device for controlled-release of meloxicam. J Clin Periodontol. 2005;32:773–7. doi: 10.1111/j.1600-051X.2005.00755.x. [DOI] [PubMed] [Google Scholar]
- 125.Ahuja A, Ali J, Rahman S. Biodegradable periodontal intrapocket device containing metronidazole and amoxycillin: Formulation and characterization. Pharmazie. 2006;61:25–9. [PubMed] [Google Scholar]
- 126.El-Kamel AH, Ashri LY, Alsarra IA. Micromatricial metronidazole benzoate film as a local mucoadhesive delivery system for treatment of periodontal diseases. AAPS PharmSciTech. 2007;8:E75. doi: 10.1208/pt0803075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Wang LC, Chen XG, Zhong DY, Xu QC. Study on poly(vinyl alcohol)/carboxymethyl-chitosan blend film as local drug delivery system. J Mater Sci Mater Med. 2007;18:1125–33. doi: 10.1007/s10856-007-0159-5. [DOI] [PubMed] [Google Scholar]
- 128.Rodriguez-Garcia A, Galan-Wong LJ, Arevalo-Niño K. Development and in vitro evaluation of biopolymers as a delivery system against periodontopathogen microorganisms. Acta Odontol Latinoam. 2010;23:158–63. [PubMed] [Google Scholar]
- 129.Chang CY, Yamada S. Evaluation of the regenerative effect of a 25% doxycycline-loaded biodegradable membrane for guided tissue regeneration. J Periodontol. 2000;71:1086–93. doi: 10.1902/jop.2000.71.7.1086. [DOI] [PubMed] [Google Scholar]
- 130.Kurtiş B, Unsal B, Cetiner D, Gültekin E, Ozcan G, Celebi N, et al. Effect of Polylactide/Glycolide (PLGA) Membranes Loaded With Metronidazole on Periodontal Regeneration Following Guided Tissue Regeneration in Dogs. J Periodontol. 2002;73:694–700. doi: 10.1902/jop.2002.73.7.694. [DOI] [PubMed] [Google Scholar]
- 131.Goodson JM, Haffajee A, Socransky SS. Periodontal therapy by local delivery of tetracycline. J Clin Periodontol. 1979;6:83–92. doi: 10.1111/j.1600-051x.1979.tb02186.x. [DOI] [PubMed] [Google Scholar]
- 132.Coventry J, Newman HN. Experimental use of a slow release device employing chlorhexidine gluconate in areas of acute periodontal inflammation. J Clin Periodontol. 1982;9:129–33. doi: 10.1111/j.1600-051x.1982.tb01228.x. [DOI] [PubMed] [Google Scholar]
- 133.Tonetti M, Cugini MA, Goodson JM. Zero-order delivery with periodontal placement of tetracycline-loaded ethylene vinyl acetate fibres. J Periodontal Res. 1990;25:243–9. doi: 10.1111/j.1600-0765.1990.tb00911.x. [DOI] [PubMed] [Google Scholar]
- 134.Demirel K, Yalçin F, Polat E, Onan U, Meriç H, Altas K. Release kinetics of 25% tetracycline hydrochloride-loaded ethylene vinyl acetate fibers. Periodontal Clin Invest. 1999;21:6–9. [PubMed] [Google Scholar]
- 135.Sakellari D, Vouros I, Konstantinidis A. The use of tetracycline fibres in the treatment of generalised aggressive periodontitis: Clinical and microbiological findings. J Int Acad Periodontol. 2003;5:52–60. [PubMed] [Google Scholar]
- 136.Aimetti M, Romano F, Torta I, Cirillo D, Caposio P, Romagnoli R. Debridement and local application of tetracycline-loaded fibres in the management of persistent periodontitis: Results after 12 months. J Clin Periodontol. 2004;31:166–72. doi: 10.1111/j.0303-6979.2004.00457.x. [DOI] [PubMed] [Google Scholar]
- 137.Paquette DW. Minocycline microspheres: A complementary medical-mechanical model for the treatment of chronic periodontitis. Compend Contin Educ Dent. 2002;23:15–21. [PubMed] [Google Scholar]
- 138.Williams RC, Paquette DW, Offenbacher S, Adams DF, Armitage GC, Bray K, et al. Treatment of periodontitis by local administration of minocycline microspheres: A controlled trial. J Periodontol. 2001;72:1535–44. doi: 10.1902/jop.2001.72.11.1535. [DOI] [PubMed] [Google Scholar]
- 139.Arica B, Aksungur P, Fienel S, Kas SH, Sargon MF, Hincal Atilla AA. Natamycin loaded chitosan microspheres for periodontal therapy. J Fac Pharm. 2003;23:77–84. [Google Scholar]
- 140.Jeyanthi R, Akiyama A, Roberts FD, VanHamont J, Friden P. One-month controlled release of an antimicrobial peptide from biodegradable poly(lactide/glycolide) microspheres for the treatment of periodontitis. Proc. Int Symp Controlled Release Bioact mater. 1997;24:883–4. [Google Scholar]
- 141.Kockisch S, Rees GD, Tsibouklis J, Smart JD. Mucoadhesive, triclosan loaded polymer microspheres for application to the oral cavity: Preparation and the controlled release characteristics. Eur J Pharm Biopharm. 2005;59:207–16. doi: 10.1016/j.ejpb.2004.07.007. [DOI] [PubMed] [Google Scholar]
- 142.Samdancioglu S, Calis S, Sumnu M, Hincal Atilla A. Formulation and in vitro evaluation of bisphosphonate loaded microspheres for implantation in osteolysis. Drug Dev Ind Pharm. 2006;32:473–81. doi: 10.1080/03639040500528871. [DOI] [PubMed] [Google Scholar]
- 143.Samati Y, Yüksel N, Tarimci N. Preparation and characterization of poly (D,L-Lactic-Co-Glycolic Acid) microspheres containing flurbiprofen sodium. Drug Deliv. 2006;13:105–11. doi: 10.1080/10717540500313331. [DOI] [PubMed] [Google Scholar]
- 144.Bland PS, Goodson JM, Gunsolley JC, Grossi SG, Otomo-Corgel J, Doherty F, et al. Association of antimicrobial and clinical efficacy: Periodontitis therapy with minocycline microspheres. J Int Acad Periodontol. 2010;12:11–9. [PubMed] [Google Scholar]
- 145.Esposito E, Cortesi R, Cervellati F, Menegatti E, Nastruzzi C. Biodegradable microparticles for sustained delivery of tetracycline to the periodontal pocket: Formulatory and drug release studies. J Microencapsul. 1997;14:175–87. doi: 10.3109/02652049709015331. [DOI] [PubMed] [Google Scholar]
- 146.Mundargi RC, Srirangrajan S, Agnihotri SA, Sangamesh A, Patil SA, Ravindra S, et al. Development and evaluation of novel biodegradable microsphere based on Poly (D,L-lactide-co-glycolide)and poly(€ -caprolactone) for contolled delivery of doxycycline in the treatment of periodontal pocket: In vitro and in vivo studies. J Control Release. 2007;119:59–68. doi: 10.1016/j.jconrel.2007.01.008. [DOI] [PubMed] [Google Scholar]
- 147.Baker RW, Krisko EA, Kochinke F. A controlled release drug delivery system for periodontal pocket. International symposium on controlled release Bioactive Materials USA. Controlled Release Soc. 1988;140:238a–b. [Google Scholar]
- 148.Bruschi ML, De Freitas O, Lara EH, Panzeri H, Gremião MP, Jones DS. Precursor system of liquid crystalline phase containing propolis microparticles for the treatment of periodontal disease: Development and characterization. Drug Dev Ind Pharm. 2008;34:267–78. doi: 10.1080/03639040701655911. [DOI] [PubMed] [Google Scholar]
- 149.Yeom HR, Park YJ, Lee SJ, Rhyu IC, Chung CP, Nisengard RJ. Clinical and microbiological effects of minocycline-loaded microcapsules in adult periodontitis. J Periodontol. 1997;68:1102–9. doi: 10.1902/jop.1997.68.11.1102. [DOI] [PubMed] [Google Scholar]
- 150.Pinon-Segundo E, Ganem-Quintanar A, Alonso-Perez V, Quintanar-Guerrero D. Preparation and characterization of triclosan nanoparticles for periodontal treatment. Int J Pharm. 2005;294:217–32. doi: 10.1016/j.ijpharm.2004.11.010. [DOI] [PubMed] [Google Scholar]
- 151.Moulari B, Lboutounne H, Chaumont JP, Guillaume Y, Millet J, Pellequer Y. Potentiation of the bactericidal activity of harungana madagascariensis lam. Ex poir. (Hypericaceae) leaf extract against oral bacteria using poly (d, l-lactide-co-glycolide) nanoparticles: In vitro study. Acta Odontol Scand. 2006;64:153–8. doi: 10.1080/00016350500483152. [DOI] [PubMed] [Google Scholar]
- 152.Bakó J, Szepesi M, Márton I, Borbély J, Hegedûs C. Synthesis of nanoparticles for dental drug delivery systems. Fogorv Sz. 2007;100:109–13. [PubMed] [Google Scholar]
- 153.Dung TH, Lee SR, Han SD, Kim SJ, Ju YM, Kim MS, et al. Chitosan-TPP nanoparticle as a release system of antisense oligonucleotide in the oral environment. J Nanosci Nanotechnol. 2007;7:3695–9. doi: 10.1166/jnn.2007.041. [DOI] [PubMed] [Google Scholar]
- 154.Jones MN, Kaszuba M. Polyhydroxy-mediated interactions between liposomes and bacterial biofilms. Biochim Biophys Acta. 1994;1193:48–54. doi: 10.1016/0005-2736(94)90331-x. [DOI] [PubMed] [Google Scholar]
- 155.Jones MN, Song YH, Kaszuba M, Reboiras MD. The interaction of phospholipid liposomes with bacteria and their use in the delivery of bactericides. J Drug Target. 1997;5:25–34. doi: 10.3109/10611869708995855. [DOI] [PubMed] [Google Scholar]
- 156.Vyas SP, Sihorkar V, Dubey PK. Preparation, characterization and in vitro antimicrobial activity of metronidazole bearing lectinized liposomes for intra-periodontal pocket delivery. Pharmazie. 2001;56:554–60. [PubMed] [Google Scholar]
- 157.Tamimi F, Torres J, Bettini R, Ruggera F, Rueda C, López-Ponce M, et al. Doxycycline sustained release from brushite cements for the treatment of periodontal diseases. J Biomed Mater Res A. 2008;85:707–14. doi: 10.1002/jbm.a.31610. [DOI] [PubMed] [Google Scholar]
- 158.Vandekerckhove BN, Van Steenberghe D, Tricio J, Rosenberg D, Encarnacion M. Efficacy on supragingival plaque control of cetylpyridinium chloride in a slow-release dosage form. J Clin Periodotol. 1995;22:824–9. doi: 10.1111/j.1600-051x.1995.tb01779.x. [DOI] [PubMed] [Google Scholar]
- 159.Jadhav BK, Khandelwal KR, Ketkar AR, Pisal SS. Formulation and evaluation of mucoadhesive tablets containing eugenol for the treatment of periodontal diseases. Drug Dev Ind Pharm. 2004;30:195–203. doi: 10.1081/ddc-120028715. [DOI] [PubMed] [Google Scholar]
- 160.Fehér A, Urbán E, Eros I, Szabó-Révész P, Csányi E. Lyotropic liquid crystal preconcentrates for the reatment of periodontal disease. Int J Pharm. 2008;358:23–6. doi: 10.1016/j.ijpharm.2008.02.025. [DOI] [PubMed] [Google Scholar]
- 161.Kozlovsky A, Sintov A, Moldovan M, Tal H. Inhibition of plaque formation by local application of a degradable controlled release system containing cetylpyridinium chloride. J Clin Periodontol. 1994;21:32–7. doi: 10.1111/j.1600-051x.1994.tb00273.x. [DOI] [PubMed] [Google Scholar]
- 162.Tallury P, Alimohammadi N, Kalachandra S. Poly(ethylene-co-vinyl acetate) copolymer matrix for delivery of chlorhexidine and acyclovir drugs for use in the oral environment: Effect of drug combination, copolymer composition and coating on the drug release rate. Dental Mater. 2007;23:404–9. doi: 10.1016/j.dental.2006.02.011. [DOI] [PubMed] [Google Scholar]
- 163.Esposito E, Carotta V, Scabbia A, Trombelli A, Antona PD, Menegatti E, et al. Comparative analysis of tetracycline- containing dental gels: Poloxamer- and monoglyceride- based formulation. Int J Pharm. 1996;142:9–23. [Google Scholar]
- 164.Emami J. In vitro - In vivo Correlation: From Theory to Applications. J Pharm Pharm Sci. 2006;9:169–89. [PubMed] [Google Scholar]
- 165.Hattingh J, Ho E. The concentration of proteins in human gingival crevicular fluid. J Periodontal Res. 1980;15:90–5. doi: 10.1111/j.1600-0765.1980.tb00262.x. [DOI] [PubMed] [Google Scholar]
- 166.Cimasoni G. Crevicular fluid update. Vol. 12. Swizerland: Karger Publishing Co; 1983. p. 71. [Google Scholar]
- 167.Kobayashi K, Kobayashi K, Soeda W, Watanabe T. Gingival cervical pH in experimental gingivitis and occlusal trauma in man. J Periodontol. 1998;69:1036–43. doi: 10.1902/jop.1998.69.9.1036. [DOI] [PubMed] [Google Scholar]
- 168.Bromberg LE, Buxton DK, Friden PM. Novel periodontal drug delivery system for treatment of periodontitis. J Control Release. 2001;71:251–9. doi: 10.1016/s0168-3659(01)00226-7. [DOI] [PubMed] [Google Scholar]
- 169.Shani S, Friedman M, Steinberg D. In vitro assessment of the antimicrobial activity of a local sustained release device containing Amine fluorides forvthe treatment of oral infectious diseases. Diagn Microbiol Infect Dis. 1998;30:93–7. doi: 10.1016/s0732-8893(97)00208-3. [DOI] [PubMed] [Google Scholar]
- 170.Ahuja A, Ali J, Rahman S, Shareef A, Khar RK. Targeted retentive device for oro-dental infections: Formulation and development. Int J Pharm. 2003;259:47–55. doi: 10.1016/s0378-5173(03)00204-7. [DOI] [PubMed] [Google Scholar]
- 171.Roskos KV, Fritzinger BK, Rao SS, Armitage GC, Heller J. Development of a drug delivery system for the treatment of periodontal disease based on bioerodible poly (ortho easters) Biomater. 1995;16:313–7. doi: 10.1016/0142-9612(95)93259-g. [DOI] [PubMed] [Google Scholar]
- 172.Okonogi S, Khongkhunthain S, Bunyaratavej P, Thusaphorn T, Umpriwan R. Development of local injectable dental gel: The influence of certain additives on physicochemical properties of glycerylmonooleate-based formulations. Drug Dev Ind Pharm. 2004;30:347–57. doi: 10.1081/ddc-120030929. [DOI] [PubMed] [Google Scholar]
- 173.Periole L, Amborgi V, Rubini D, Giovagnoli S, Ricci M, Balsi P, Rossi C. Novel mucoiadhesive buccal formulation containing metronidazole for the treatment of periodontal disease. J Control Release. 2004;95:521–33. doi: 10.1016/j.jconrel.2003.12.018. [DOI] [PubMed] [Google Scholar]
- 174.Kelly HM, Deasy PB, Ziaka E, Claffey N. Formulation and preliminary in vivo dog studies of a novel drug delivery system for the treatment of periodontitis. Int J Pharm. 2004;274:167–83. doi: 10.1016/j.ijpharm.2004.01.019. [DOI] [PubMed] [Google Scholar]
- 175.Yue IC, Poff J, Cortés ME, Sinisterra RD, Faris CB, Hildgen P, et al. A novel polymeric chlorhexidine delivery device for the treatment of periodontal disease. Biomaterials. 2004;25:3743–50. doi: 10.1016/j.biomaterials.2003.09.113. [DOI] [PubMed] [Google Scholar]
- 176.Liuy DZ, Chenz WZ, Lee CP, Wuz SL, Wangz YC, Chung TW. Effects of alginate coated on PLGA microspheres for delivery tetracycline hydrochloride to periodontal pockets. J Microencapsul. 2004;21:643–52. doi: 10.1080/02652040400000512. [DOI] [PubMed] [Google Scholar]
- 177.Weinberg MA, Bral M. Laboratory animal models in periodontology. J Clin Periodontol. 1999;26:335–40. doi: 10.1034/j.1600-051x.1999.260601.x. [DOI] [PubMed] [Google Scholar]
- 178.Krygier G, Genco R, Mashimo P, Hausman E. Experimental gingivitis in Macaca Speciosa monkeys: Clinical, bacteriologic and histologic similarities to human gingivitis. J Periodontol. 1973;44:454–463. doi: 10.1902/jop.1973.44.8.454. [DOI] [PubMed] [Google Scholar]
- 179.Schou S, Holmstrup P, Kornman KS. Non-Human primates used in studies of periodontal disease pathogenesis: A review of the literature. J Periodontol. 1993;64:497–508. doi: 10.1902/jop.1993.64.6.497. [DOI] [PubMed] [Google Scholar]
- 180.Brecx M, Nalbandiam J, Ooya K, Kornman K, Robertson R. Morphological studies on periodontal disease in the Cynomolgus monkey (II). Light microscopic observations on ligature induced Periodontitis. J Periodontal Res. 1985;20:165–75. doi: 10.1111/j.1600-0765.1985.tb00423.x. [DOI] [PubMed] [Google Scholar]
- 181.Polson AM. Trauma and progression of marginal periodontitis in squirrel monkeys (II). Co-destructive factors or periodontitis and mechanicallyproduced injury. J Periodontal Res. 1974;9:108–13. doi: 10.1111/j.1600-0765.1974.tb00661.x. [DOI] [PubMed] [Google Scholar]
- 182.Caton JG, Kowalski CJ. Primate model for testing periodontal treatment procedures (II). Production of contralaterally similar lesions. J Periodontol. 1976;46:506–10. doi: 10.1902/jop.1976.47.9.506. [DOI] [PubMed] [Google Scholar]
- 183.Giannobile WV, Finkelman RD, Lynch SE. Comparison of canine and non-human primate animal models for periodontal regenerative therapy. Result following a single administration of PDGF/IGF-I. J Periodontol. 1994;65:1158–68. doi: 10.1902/jop.1994.65.12.1158. [DOI] [PubMed] [Google Scholar]
- 184.Caton J, Mota L, Gandini L, Laskaris B. Non-human primate models for testing the efficacy and safety of periodontal regenerative procedures. J Periodontol. 1994;65:1143–50. doi: 10.1902/jop.1994.65.12.1143. [DOI] [PubMed] [Google Scholar]
- 185.Fritz EF, Braswell LD, Koth D, Jeff coat M, Reddy M, Cotsonis G. Experimental peri-implantitis in consecutively placed, loaded root-form and plateform implants in adult Macaca mulatta monkeys. J Periodontol. 1997;68:1131–5. doi: 10.1902/jop.1997.68.11.1131. [DOI] [PubMed] [Google Scholar]
- 186.Navia JM. Animal models in dental research. Vol. 169. Alabama: University of Alabama Press; 1977. pp. 170–8. [Google Scholar]
- 187.Listgarten MA. Similarity of epithelial relationships in the gingiva of rat and man. J Periodontol. 1975;46:677–80. doi: 10.1902/jop.1975.46.11.677. [DOI] [PubMed] [Google Scholar]
- 188.Irving J, Socransky S. Histological changes in experimental periodontal disease in gnotobiotic rats and conventional hamsters. J Periodontal Res. 1974;9:73–80. doi: 10.1111/j.1600-0765.1974.tb00656.x. [DOI] [PubMed] [Google Scholar]
- 189.Socransky S, Hubersak C, Propas D. Induction of periodontal destruction in gnotobiotic rats by a human oral strain of Actinomyces Naeslundii. Arch Oral Biol. 1970;15:993–5. doi: 10.1016/0003-9969(70)90095-6. [DOI] [PubMed] [Google Scholar]
- 190.Klausen B, Hougen H, Eriksen W, Fiehn N. Induction of periodontal bone loss in athymic (nude) rats monoinfected with streptococcus mutans. J Periodontal Res. 1986;21:5–12. doi: 10.1111/j.1600-0765.1986.tb01431.x. [DOI] [PubMed] [Google Scholar]
- 191.Crawford J, Taubman M, Smith D. The natural history of periodontal bone loss in germfree and gnotobiotic rats infected with periodontophathic microorganisms. J Periodontal Res. 1978;8:57–62. doi: 10.1111/j.1600-0765.1978.tb00186.x. [DOI] [PubMed] [Google Scholar]
- 192.Heijl L, Wennstrom J, Lindhe J, Socransky SS. Periodontal disease in gnotobiotic rats. J Periodontal Res. 1980;15:405–19. doi: 10.1111/j.1600-0765.1980.tb00298.x. [DOI] [PubMed] [Google Scholar]
- 193.Baer PM, Stephan R, White C. Studies on experimental calculus formation in the rat. J Periodontol. 1961;32:190–6. [Google Scholar]
- 194.Jordan H, Keyes P. Aerobic, grampositive, filamentous bacteria as etiologic agents of experimental periodontal disease in Hamster. Arch Oral Bio. 1964;9:401–14. doi: 10.1016/0003-9969(64)90025-1. [DOI] [PubMed] [Google Scholar]
- 195.Keyes P, Jordan H. Periodontal lesions in Syrian hamster (III) findings related to an infectious and transmissible component. Arch Oral Biol. 1964;9:377–400. doi: 10.1016/0003-9969(64)90024-x. [DOI] [PubMed] [Google Scholar]
- 196.Attstrom R, Graf-De Beer M, Schroeder H. Clinical and histologic characteristics of normal gingival in dogs. J Periodontal Res. 1975;10:115–27. doi: 10.1111/j.1600-0765.1975.tb00016.x. [DOI] [PubMed] [Google Scholar]
- 197.Ericsson I, Lindhe J, Rylander H, Okamoto H. Experimental periodontal breakdown in the dog. Scandinavia J Res. 1975;83:189–92. doi: 10.1111/j.1600-0722.1975.tb01198.x. [DOI] [PubMed] [Google Scholar]
- 198.Gad T. Periodontal disease in dogs (I). Clinical investigation. J Periodontal Res. 1968;3:268–72. doi: 10.1111/j.1600-0765.1968.tb01929.x. [DOI] [PubMed] [Google Scholar]
- 199.Hull PS, Soames JV, Davies RM. Periodontal disease in a Beagle dog colony. J Comp Path. 1974;84:143–51. doi: 10.1016/0021-9975(74)90055-3. [DOI] [PubMed] [Google Scholar]
- 200.Lindhe J, Hamp S, Löe H. Plaque induced periodontal disease in Beagle Dogs, A 4-year clinical roentgenographical and histometrical study. J Periodontal Res. 1975;10:243–55. doi: 10.1111/j.1600-0765.1975.tb00031.x. [DOI] [PubMed] [Google Scholar]
- 201.Soames J, Davies R. Lymphocytemacrophage and lymphocyte-lymphocytem associations in early gingivitis in Beagle dogs. J Periodontal Res. 1980;15:341–4. doi: 10.1111/j.1600-0765.1980.tb00290.x. [DOI] [PubMed] [Google Scholar]
- 202.Schroeder H, Lindhe J. Conversion of established gingivitis in the dog into destructive periodontitis. Arch Oral Biol. 1975;20:775–82. doi: 10.1016/0003-9969(75)90052-7. [DOI] [PubMed] [Google Scholar]
- 203.Lindhe J, Rylander H. Experimental gingivitis in young dogs. Scandinavia J Dent Res. 1975;83:314–26. doi: 10.1111/j.1600-0722.1975.tb00444.x. [DOI] [PubMed] [Google Scholar]
- 204.Harper DS, Mann PH, Regnier S. Measurement of dietary effects upon calculus accumulation rates in the domestic ferret. J Dent Res. 1990;69:447–50. doi: 10.1177/00220345900690020501. [DOI] [PubMed] [Google Scholar]
- 205.King JD, Gimson AP. Experimental investigations of periodontal disease in the ferret and related lesions in man. Br Dent J. 1947;83:126–7. [PubMed] [Google Scholar]
- 206.Fischer RG, Klinge B. Clinical and histological evaluation of ligature-induced periodontitis in the domestic ferret. J Clin Periodontol. 1994;21:230–9. doi: 10.1111/j.1600-051x.1994.tb00311.x. [DOI] [PubMed] [Google Scholar]
- 207.Medlicott NJ, Rathbone MJ, Tucker IG, Holborow HW. Delivery systems for the administration of drugs to the periodontal pocket. Adv Drug Del Rev. 1994;13:181–203. [Google Scholar]
- 208.Ainamo J. Epidemiology of periodontal disease. In: Lindhe J, editor. Textbook of clinical periodontology. Munksgaard: Copenhagen; 1989. pp. 70–91. [Google Scholar]
- 209.Nyman S, Lindhe J. Examination of patients with periodontal disease. In: Lindhe J, editor. Textbook of clinical periodontology. Munksgaard: Copenhagen; 1989. pp. 310–22. [Google Scholar]
- 210.Klinge B, Kuvatanasuhati J, Attström R, Kalfas S, Edwardsson S. The effect of topical metronidazole therapy on experimentally-induced periodontitis in the beagle dog. J Clin Periodontol. 1992;19:702–7. doi: 10.1111/j.1600-051x.1992.tb02532.x. [DOI] [PubMed] [Google Scholar]
- 211.Kozlovsky A, Sintov A, Zubery Y, Tal H. Inhibition of plaque formation and gingivitis in beagle dogs by topical use of a degradable controlled-release system containing chlorhexidine. J Dent Res. 1992;71:1577–81. doi: 10.1177/00220345920710090601. [DOI] [PubMed] [Google Scholar]
- 212.Polson AM, Southard GL, Dunn RL, Yewey GL, Godowski KC, Polson AP, et al. Periodontal pocket treatment in beagle dogs using subgingival doxycycline from a biodegradable system. I. Initial clinical responses. J Periodontol. 1996;67:1176–84. doi: 10.1902/jop.1996.67.11.1176. [DOI] [PubMed] [Google Scholar]
- 213.Hayashi K, Takada K, Hirasawa M. Clinical and microbiological effects of controlled-release local delivery of minocycline on periodontitis in dogs. Am J Veterinary. 1998;59:464–7. [PubMed] [Google Scholar]
- 214.Sato Y, Kikuchi M, Ohata N, Tamura M, Kuboki Y. Enhanced cementum formation in experimentally induced cementum defects of the root surface with the application of recombinant basic fibroblast growth factor in collagen gel in vivo. J Periodontol. 2004;75:243–8. doi: 10.1902/jop.2004.75.2.243. [DOI] [PubMed] [Google Scholar]
- 215.Anzai J, Kitamura M, Nozaki T, Nagayasu T, Terashima A, Asano T, Murakami S. Effects of concomitant use of fibroblast growth factor (FGF)-2 with beta-tricalcium phosphate (β-TCP) on the beagle dog 1-wall periodontal defect model. Biochem Biophys Res Commun. 2010;403:345–50. doi: 10.1016/j.bbrc.2010.11.032. [DOI] [PubMed] [Google Scholar]
- 216.Luan Q, Desta T, Chehab L, Sanders VJ, Plattner J, Graves DT. Inhibition of experimental periodontitis by a topical boron-based antimicrobial. J Dent Res. 2008;87:148–52. doi: 10.1177/154405910808700208. [DOI] [PubMed] [Google Scholar]
- 217.Houri-Haddad Y, Halabi A, Soskolne WA. Inflammatory response to chlorhexidine, minocycline HCl and doxycycline HCl in an in vivo mouse model. J Clin Periodontol. 2008;35:783–8. doi: 10.1111/j.1600-051X.2008.01290.x. [DOI] [PubMed] [Google Scholar]
- 218.Vandekerckhove BN, Quirynen M, Van Steeberghe D. The use of localy delivered minocycline in the treatment of chronic periodontitis. A review of literature. J Clin Periodontol. 1998;25:964–8. doi: 10.1111/j.1600-051x.1998.tb02399.x. [DOI] [PubMed] [Google Scholar]
- 219.Newman HN. Plaque and chronin inflammatory disease. A question of ecology. J Clin Periodontol. 1990;17:533–44. [PubMed] [Google Scholar]
- 220.Cheristersson LA, Zambon JJ, Genco RJ. Dental bacterial plaques. Nature and role in periodontal disease. J Clin Periodontol. 1991;11:21–32. doi: 10.1111/j.1600-051x.1991.tb02314.x. [DOI] [PubMed] [Google Scholar]
- 221.Ikinci G, Senel S, Akincibay H, Kaş S, Erciş S, Wilson CG, Hincal AA. Effect of chitosan on a periodontal pathogen Porphyromonas gingivalis. Int J Pharm. 2002;235:121–7. doi: 10.1016/s0378-5173(01)00974-7. [DOI] [PubMed] [Google Scholar]
- 222.Govender S, Pillay V, Chetty DJ, Essack SY, Dangor CM, Govender T. Optimisation and characterisation of bioadhesive controlled release tetracycline microspheres. Int J Pharm. 2005;306:24–40. doi: 10.1016/j.ijpharm.2005.07.026. [DOI] [PubMed] [Google Scholar]
- 223.Ahuja A, Rahman S, Ali A, Chaudhry R. Effect of Dental Films containing amoxyciline and metronidazole on periodontal pathogens: Microbiological response. Pharmazie. 2003;58:716–20. [PubMed] [Google Scholar]