

Abstract
Orthopaedic surgeons deployed to Afghanistan are primarily responsible for the provision of care to injured Us and coalition soldiers. A vast and well-coordinated system of echeloned care has evolved to rapidly treat and evacuate injured soldiers. Orthopaedic care of injured Afghan civilians represents a common secondary mission performed by deployed orthopaedic surgeons. In this article, I describe my experiences while deployed to Afghanistan in 2011 as part of the special Operations surgical team.
Care of the Wounded Coalition Soldier in Afghanistan
The evacuation and care of wounded soldiers has evolved throughout the history of warfare. In the recent conflicts in Iraq and Afghanistan, an echeloned approach to trauma care has been instituted.1 There are five levels of care. The principles of damage control surgery are applied at each level, and an efficient system of air evacuation allows for rapid transfer of wounded warriors to US facilities for definitive care.
Level I care begins with immediate care on the battle-field. All soldiers are trained in basic battlefield first aid and carry equipment including tourniquets, angiocaths for needle decompression, and oral airways. In addition, each unit has combat medics who provide first-line medical care. Soldiers are trained to use tourniquets liberally on the battlefield for extremity wounds. Evacuation often proceeds from the battlefield to a battlefield aid station, which is manned by either a physician or a PA. ATLS and resuscitation are performed at this location. However, there is no surgical capability and holding capacity is limited. A wounded soldier who requires surgical treatment may bypass the aid station and be routed directly to a higher level of care.
Surgical capability begins at Level II facilities. Level II facilities are strategically located throughout the theater of operations. All facilities provide basic laboratory and imaging capability and are staffed by orthopaedic surgeons, general surgeons, nurse anesthetists, critical care nursing staff, and other personnel to provide laboratory, radiography, ward, and OR support. Level II resources allow provision of Damage Control Surgery in a timely fashion. With respect to orthopaedic care of extremity injuries, initial debridement and provisional external fixation are typically provided. Fluoroscopic imaging is generally available. Only coalition soldiers with relatively minor injuries are treated definitively at Level II facilities. Soldiers are rapidly transported from the Level II facility to a higher level of care, which typically occurs within a few hours of arrival at the Level II facility.
Level III facilities are larger, fixed facilities which have a capability similar to US civilian trauma centers. There are two Level III facilities in Afghanistan. Specialists assigned to Level III facilities often include vascular surgeons, thoracic surgeons, urologists, obstetrician/ gynecologists, neurosurgeons, otolaryngologists, and ophthalmologists in addition to general and orthopaedic surgeons. Advanced imaging, laboratory, and critical care resources are available. With respect to injured coalition soldiers, Level III facilities allow for additional resuscitation and provisional surgical treatment en route to higher levels of care. Orthopaedic care typically involves repeat debridement, application or adjustment of external fixation, and Wound VAC application. Evacuation to higher levels of care often occurs within 24 hours or less of arrival to a Level III facility.
Level IV represents the first facility in which definitive surgical management can be provided outside the combat zone. With respect to Afghanistan and Iraq, soldiers are evacuated from the Level III facilities to Landstuhl Regional Medical Center in Germany. Injuries are further evaluated, debrided, and provisionally stabilized as needed. Definitive fixation is only performed for simple, closed injuries. Patients are usually held no longer than 72 hours prior to transport back to the United States for definitive care.
Level V care is provided by several military treatment facilities in the United States. Efforts are made to evacuate the patient as close to his home station as possible while still providing the necessary capabilities. Many of these complex extremity wounds require a high level of skill and experience to manage appropriately. Military facilities able to provide the full spectrum of care and rehabilitation for complex injuries are located in Washington D.C., San Antonio, and San Diego.
Care of Local Nationals
While care of coalition soldiers in theater is generally limited to damage control surgery, definitive care is provided to Afghan soldiers, police, and civilians at Level II and Level III facilities throughout Afghanistan. In fact, at many locations the majority of care is provided to Afghans. This involves management of complex extremity injuries that challenge available material resources as well as the individual orthopaedic surgeon’s knowledge and technical skill.
Special Operations Surgical Team
I deployed to Afghanistan as part of the Air Force Special Operations Surgical Team (SOST). Team members included a general surgeon, an orthopaedic surgeon, an emergency physician, a nurse anesthetist and a surgical technician. SOST was developed in 2003 to enhance the speed, flexibility, and reach of surgical care in support of special operations missions.2 SOST provides scaled increments of capability depending on the mission and anticipated time at a given location. For shorter missions, the team travels with only backpacks and can set up resuscitative and surgical capability within 10 minutes of arrival at any location. In the most remote locations, orthopaedic care is limited to debridement, fasciotomies, and provisional stabilization via external fixation, usually without the aid of fluoroscopic guidance.
My Experiences Deployed to Afghanistan
From July to December of 2011 I was in Afghanistan with the Special Operations Surgical Team. Based upon the theater needs at the time, our unique capabilities were only required for a small percent of the time. Therefore, we had the opportunity to visit a number of different locations and augment other coalition facilities while waiting for missions specific to our capabilities. We also spent time mentoring at an Afghan Hospital, a very unique professional and cultural opportunity. (In the remainder of this article, I’ll describe some of my experiences.)
Level III Facility, Bagram Air Field
Bagram Air Field is located north of Kabul in North-east Afghanistan and is one of the largest bases in Afghanistan. The base was actually a primary staging point for Soviet operations in the 80s, and a contentious strategic location in the subsequent Afghan Civil War. During the US’s ten-year involvement, Bagram Air Field has continued to play a central role. Many coalition troops in supporting roles remain in Bagram while deployed, and many others pass through en route to more forward locations. This large facility actually contains coffee shops, fast food and movie theaters.
Craig Joint Theater Hospital, located on Bagram Air Field, is a large Level III facility. As noted above, this type of facility rapidly accepts transfers from lower level facilities, provides additional resuscitation and stabilization, and facilitates transfer back to the United States via Germany. Imaging capability such as CT and angiography, as well as specialized surgical capability including vascular and neurological surgery can also be employed at this location.
Three Air Force orthopaedic surgeons are assigned primarily to Craig joint Theater Hospital. This generally includes a fellowship-trained hand surgeon and orthopaedic traumatologist. A typical deployment here is six months. In addition to the assigned surgeons, many other surgeons will briefly pass through the facility on their way to more forward locations. I spent two weeks at this facility in August of 2011 and had the opportunity to assist with clinical duties. The orthopaedic resources and facilities are very much on par with what one would expect at a Level I facility in the United States. Multiple implants are available, including various nails and pre-contoured plates, as well as surgical microscopes and the full gamut of microvascular surgical equipment.
At Bagram, the orthopaedic surgeon has the opportunity to evaluate the majority of all orthopaedic injuries sustained by US and other coalition soldiers in Afghanistan as they pass through en route to Germany and the United States. Almost all injuries have already been provisionally stabilized and debrided at a Level II facility. Their second debridement is performed at Bagram. While I was at Bahram, I gained an appreciation for the remarkable volume and severity of extremity injuries sustained in this conflict. Many of the injuries are the result of blasts from improvised explosive devices (IEDs). The dismounted (walking) IED blast represents a particularly severe injury often associated with bilateral lower extremity traumatic amputations with associated abdominal, peroneal, and upper extremity injuries. With improved technology such as body armor, many previously fatal injuries are now survivable, making effective treatment and rehabilitation of severe extremity injuries more common.
A second role of the orthopaedic surgeon assigned to Bagram is the definitive care of local Afghan soldiers and civilians. Again, high-energy gunshot wounds and IED blasts are very prevalent. Some of the more difficult local-national cases from around Afghanistan can be referred to Bagram on a space-available basis. General principles of managing war wounds are again employed to include provisional fixation and multiple debridements prior to attempts at definitive treatment. Often, there are questions of limb salvage versus amputation. Although the International Red Cross does provide fairly consistent, if primitive, prosthesis care throughout much of the country, the Afghans were generally very resistant to consent to elective amputation in almost any circumstance. I did participate in multiple procedures designed to preserve limbs, including rotational flaps as well as nerve repairs, tendon transfers, and complex hand re-construction procedures. Unfortunately, postoperative complications such as infection seemed to be relatively common, and follow-up at this large, centralized facility was quite inconsistent, even after complex procedures. Interestingly, many patients with external fixators in place did not return to be seen after their operations.
Level II Facility, Southern Afghanistan
Approximately 10 weeks of my deployment were spent augmenting an existing Forward Surgical Team (FST) in southern Afghanistan, in a region which was a previous Taliban stronghold. During my depoloyment it was an area of contention and frequent violence. Many Afghans affiliate more with their ethnic group and local tribe than with the nation as a whole. These regional variations were obvious during my brief time in Afghanistan. Generally speaking, people in this region practiced more fundamental Islam, were less educated, and were less tolerant of western notions of women’s rights compared to other regions.
The facility included a four-bed trauma bay, a single OR with two tables, as well as plain radiography and fluoroscopic capability (Figure 1). Level II facilities typically are stocked with basic small- and large-fragment plate and screws as well as external fixators. We were also able to arrange for the incorporation of intramedually nails for tibial and retrograde femoral nailings as well as flexible rods for pediatric femur fractures.
Figure 1. Operating room at the Level II Forward Surgical Element in southern Afghanistan. Fluoroscopic capability as well as basic orthopaedic implants including flexible IM rods were available at this facility.

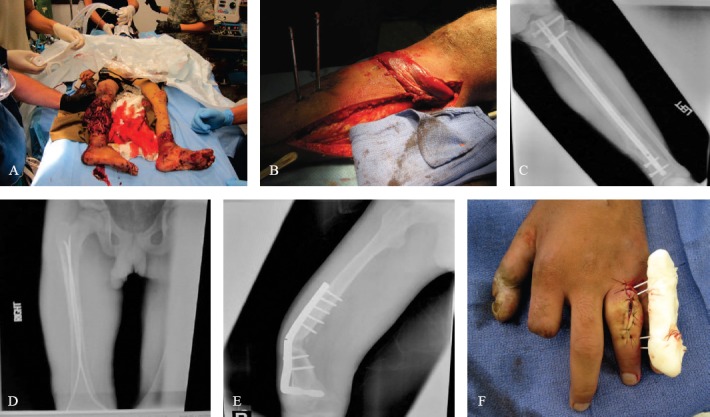
As an orthopaedic surgeon, I stayed busy here, performing over 150 cases over a ten- week period (Figure 2). Over 90% of the surgeries were provided to local Afghan soldiers and civilians, including many children. IED injuries were quite prevalent as were gunshot wounds. In addition, when resources were available, we also provided orthopaedic care for non-war related trauma including traffic accidents and simple falls.
Figure 2. Typical cases performed in Level II facility, southern Afghanistan. A- 6 year old male with IED blast wounds. B-soleus flap for tibia coverage in 30 year old male. C- IM nail for open tibia fracture following GSW. D- flexible rods for closed femur fracture in 8 year old male. E – 12 year old male with TB of bone eventually treated with revision ORIF with ICBG. prior surgery had been performed in pakistan. F – PIP fusion stabilized with improvised external fixator using K-wires and methylmethacralate.
In my first year of surgical practice at Eglin Air Force Base, Florida, I performed primarily arthroscopic procedures and occasional trauma cases – usually limited to simple, closed fractures. This certainly did not prepare me for the complex extremity trauma I saw in Afghanistan. Fortunately, I was very well trained at Iowa and could discuss and work together on difficult cases with Dr. Brannan, another orthopaedic surgeon assigned to the facility. Given our limited resources, we often had to be a bit creative in choosing implants and reconstruction options.
We performed the first tibial and femoral intramedullary nailing procedures in this region. This represented a significant improvement over definitive external fixation, which was the previous preferred treatment. I also performed a number of flexible nail cases for pediatric femur fractures, avoiding definitive external fixation or prolonged traction in children too large for immediate spica casting.
Soft tissue management represented the primary challenge in managing complex war wounds. Skin grafting was employed frequently, as were rotational gastroc and soleus flaps for open tibia wounds. These procedures were often performed in conjunction with illiac crest bone grafting. Free flaps were not attempted due to surgeon and resource limitations. Patients requiring free-flap coverage were often told that amputation was the only option available to them.
The opportunity to provide care to Afghans at this location was a very rewarding and valuable professional experience for me. For much of my time in Afghanistan, I felt much more like a humanitarian worker than a US military soldier. I was able to make decisions, perform surgery to the best of my ability, and document only what was needed to insure appropriate continuity of care. We were truly the only medical option for many people and had the opportunity to significantly improve their lives. It was a refreshing experience and increased my interest in future overseas volunteer activities.
Forward Deployment in Support of Special Operations Teams
Our Special Operations Surgical Team (SOST) spent several days at far forward locations in support of small-unit special operations missions. I cannot discuss specific locations, but we traveled by helicopter with only backpacks and could quickly set up provisional surgical and resuscitative capability in tents or even outdoors, as needed. I carried the “surgical table” in my backpack, which simply consisted of a litter and stanchions. By participating in these missions, I gained even more appreciation for the unique talents, dedication, and bravery of these elite special forces units.
Mentoring at an Afghan National Army Hospital, Western Afghanistan
Our team also spent seven weeks mentoring Afghan surgeons in an Afghan National Army Hospital (ANA) in western Afghanistan. The culture and people of this region sharply contrasted with those from other regions. Even the Dari language was distinct. People tended to be more educated, and women played a more prominent role in society.
By Afghan standards, the ANA hospital was very well equipped. The primary administrator of the hospital was a well-connected Afghan general. The hospital had an ICU with ventilators as well as two modern ORs. Orthopaedic equipment included basic plates and screws, external fixators, and SIGN nails. However, limitations to providing modern care did exist. For example, we could run no laboratory tests due to absent or tainted reagents. The purity and integrity of medications such as IV antibiotics were always in question. The largely well-meaning and dedicated medical staff at the hospital dealt with these challenges daily.
I worked with two Afghan surgeons who performed both general surgery and orthopaedic procedures. Standards for medical and surgical training are much different in Afghanistan compared to western nations. Both surgeons had largely been trained as apprentices. One received most of his training from Soviet surgeons when Afghanistan was under Soviet control. The other trained for a few years in a large hospital in Kabul. Years of constant war and conflict had honed their basic trauma skills. Both could perform amputations with great skill and speed. We performed several interesting surgeries together. Femoral nonunions were relatively common following definitive external fixator treatment, and we plated a number of these with illiac crest autograft.
Surgical mentoring at the Afghan hospital during a time of war certainly presented some unique challenges. Cultural and language differences were profound. I was younger than both of my Afghan colleagues and was a visitor in their hospital. Although there were some frustrating moments initially, I hope that our work ultimately provided benefit to the Afghan surgeons and the facility in general. I sincerely enjoyed having the opportunity to work in an Afghan hospital, learn about their culture, and develop friendships with my ANA colleagues (Figure 3).
Figure 3. Enjoying lunch with members of the SOST team and our Afghan colleagues at the Afghan National Army Hospital in western Afghanistan.

Conclusions
Orthopaedic military surgeons in Afghanistan care for injured US soldiers and provide musculoskeletal care to the local populations. Although it is difficult to be away from family and assume an increased level of personal danger, deploying as an orthopaedic surgeon to Afghanistan clearly represented the most valuable and rewarding experience of my young professional career.
References
- 1.Bagg MR, Covey DC, Powell ET. Levels of medical care in the global war on terrorism. J Am Acad Orthop Surg. 2006;14(10):57–59. doi: 10.5435/00124635-200600001-00003. [DOI] [PubMed] [Google Scholar]
- 2.Ervin M. Air Force Special Operations Command Special Operations Surgical Team (SOST) CONOPS. Journal of Special Operations Medicine. 2008;8(2):68–75. [Google Scholar]