

Abstract
Rationale
Abuse and neglect are highly prevalent in children and have enduring neurobiological effects. Stressful early life environments perturb the hypothalamic–pituitary–adrenal (HPA) axis, which in turn may predispose to psychiatric disorders in adulthood. However, studies of childhood maltreatment and adult HPA function have not yet rigorously investigated the differential effects of maltreatment subtypes, including physical abuse.
Objective
In this study, we sought to replicate our previous finding that childhood maltreatment was associated with attenuated cortisol responses to stress and determine whether the type of maltreatment was a determinant of the stress response.
Methods
Salivary cortisol response to the Trier Social Stress Test (TSST) was examined in a non-clinical sample of women (n=110). Subjects had no acute medical problems and were not seeking psychiatric treatment. Effects of five maltreatment types, as measured by the Childhood Trauma Questionnaire, on cortisol response to the TSST were investigated. To further examine the significant (p<0.005) effect of one maltreatment type, women with childhood physical abuse (PA) (n=20) were compared to those without past PA (n=90).
Results
Women reporting childhood PA displayed a significantly blunted cortisol response to the TSST compared with subjects without PA, after controlling for estrogen use, age, other forms of maltreatment, and other potential confounds. There were no differences between PA and control groups with regard to physiological arousal during the stress challenge.
Conclusions
In a non-clinical sample of women with minimal or no current psychopathology, physical abuse is associated with a blunted cortisol response to a psychosocial stress task.
Keywords: Childhood, Trauma, Stress, Physical abuse, Cortisol, HPA axis, Saliva
Introduction
Early life trauma is widely prevalent. The developmental stress caused by such abuse has repeatedly been associated with later-life consequences. Various forms of childhood adversity, including a chaotic and neglectful home environment in addition to physical and sexual trauma, have been shown to be additive risk factors for psychopathology, including suicide (Dube et al. 2001) and development of mood disorders (Kessler and Magee 1993; Molnar et al. 2001). The physiologic changes that underpin the psychopathologic sequelae of early life stress are just beginning to be characterized. In addition to neurohormonal dysregulation, early life stress in the form of maltreatment may mediate changes in immune function, as evidenced by elevated levels of inflammatory markers (Danese et al. 2008).
Evidence points to dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis as one underlying source of the adverse health outcomes stemming from early life stress. Both increased and decreased cortisol responsivity have been linked to maltreatment during critical times of brain development in childhood (Heim et al. 2000). Our group reported decreased reactivity of the HPA axis in healthy adults reporting childhood maltreatment compared with non-maltreated controls when subjects were exposed to a standardized psychosocial challenge (Carpenter et al. 2007). Discrepant or seemingly opposite findings regarding the direction of abnormal HPA axis reactivity or basal cortisol indices (Bremmer et al. 2007) likely reflect the numerous factors that may alter HPA axis function in such investigations (Entringer et al. 2009; Fiocco et al. 2007; Kajantie et al. 2007; Kudielka et al. 2009). HPA axis function is thought to change with age (Kudielka et al. 2009) and may vary with sex (Chopra et al. 2009; Kirschbaum et al. 1999), as well as with certain genetic polymorphisms (Derijk and de Kloet 2008; Ising et al. 2008; Kumsta et al. 2007; Wust et al. 2009). Monophasic oral contraceptives may have a blunting effect on free cortisol response to psychological stress in women (Kirschbaum et al. 1999).
Cortisol concentrations may be measured in different biological specimens, including serum, plasma, and saliva. Findings may vary according to the source used for assay in acute stress challenge. Furthermore, researchers in this area have described different subtypes of abuse and neglect that may have different, perhaps even opposite, effects on HPA axis responsivity as assessed in adulthood (Flory et al. 2009; Roy 2002; Schafer et al. 2010). A post hoc analysis of cortisol response to the Trier Social Stress Test (TSST) in a previous study we conducted revealed the direction of cortisol response seen among maltreated subjects differed according to maltreatment subtype; emotional neglect significantly dampened and sexual abuse significantly enhanced cortisol response to acute stress (TSST), while a trend-level dampening effect was seen for physical abuse (Carpenter et al. 2007). Other research groups have also reported abnormal cortisol concentrations unique to one, but not other, subtypes of maltreatment reported by adult subjects (Flory et al. 2009; Weissbecker et al. 2006).
Given these considerations, we sought to replicate and extend our earlier findings by investigating the effect of childhood maltreatment on stress responses in adult women from a community sample. In contrast to our prior study, cortisol concentrations were measured in saliva rather than in plasma. We approached this study by examining the effect of each of five different subtypes of maltreatment independently and hypothesized that exposure to early life adversity would be associated with diminished cortisol response to acute psychosocial stress challenge.
Methods and materials
One hundred and ten women, ages 18 to 61 years, were enrolled and completed all assessments in the study protocol. Subjects were recruited from the community via flyers, as well as through Internet and newspaper advertisements seeking healthy volunteers. Phone screens, diagnostic interviews, and laboratory screening tests were used to exclude participants currently meeting diagnostic criteria for substance use disorders and all disorders characterized by psychosis. Subjects underwent physical and neurological examinations. Electrocardiograms and laboratory studies for complete blood count, serum electrolytes, thyroid-stimulating hormone, urine toxicology, and urinalysis were conducted. Subjects were excluded from the present study if they were pregnant, worked night shifts, or if they had one or more of the following conditions: acute or unstable medical illness, a history of brain injury, seizure disorder, endocrine disease, or recreational use of illicit substances. Also excluded were individuals undergoing treatment with drugs which might influence HPA axis function, including psychotropic medications, beta blockers, angiotensin-converting enzyme inhibitors, ketoconazole, metyrapone, and corticosteroids. Subjects were free of these medications for at least 2 weeks (or five half-lives, if appropriate) prior to participation. Additionally, subjects could not have previously participated in a TSST. Oral contraceptives and estrogen replacement therapies were allowed, but depot formulations of progesterone were excluded due to their poorly characterized effects on the HPA axis. Stage of menstrual cycle was determined by self-report and recorded. All subjects gave voluntary written informed consent to participate in this study, which was approved by the Butler Hospital Institutional Review Board.
Subjects seeking treatment for psychiatric symptoms or disorders were excluded from this study. The presence of current or lifetime history of Axis I psychiatric diagnoses was assessed using the Structured Clinical Interview for DSM-IV (SCID; First et al. 1996). The 28-item version of the Childhood Trauma Questionnaire (CTQ; Bernstein et al. 2003) was used to assess childhood maltreatment. The CTQ (28-item version) is a self-report measure that generates a total score and subscale scores for five types of maltreatment (emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect). CTQ subscale scores reaching the threshold for the “moderate to severe” range were considered positive for maltreatment. Subjects scoring “none or minimal” for each subscale were considered controls with regard to that particular type of maltreatment.
The following additional self-report measures were included to further characterize subjects: (1) Inventory of Depressive Symptomatology—Self-Report Scale (IDS-SR; Rush et al. 1996), (2) State–Trait Anxiety Questionnaire (STAI; Spielberger 1983), and the (3) Perceived Stress Scale (PSS; Cohen et al. 1983).
The TSST is a standardized laboratory stressor that reliably induces psychological and physiological stress, which is reflected in subjects’ cortisol and physiological responses. The TSST protocol involves public speaking, role-playing, and mental arithmetic tasks in front of a panel of confederate judges. The subjects are informed of the protocol and then have an anticipation period followed by a 10-min test period. During the test period, the subject must deliver a monologue speech about his or her qualifications for a chosen vocation and perform mental arithmetic consisting of serial subtraction. Subjects were provided with limited information about the nature of the TSST other than that they would be involved in a “role play” that involved possible transient psychological distress.
To minimize the effects of diurnal variation in cortisol response, the TSST was administered at the same time on each test day. Subjects were instructed not to eat or exercise for 1 h before the test. Saliva samples were collected at time points 0 (1:45P.M.; immediately before meeting the judges and being told about the public speech and arithmetic recitation), 15 min (2:00P.M.; the end of the anticipation period during which the subject prepared his or her speech), 30 min (2:15P.M.; several minutes after completing the speaking/arithmetic test), 45 min, 60 min, 75 min, and 90 min. Heart rate and blood pressure were monitored before, during, and after the role-play/arithmetic stressor. Somatic and mood self-report ratings included a battery of Visual Analog Scales (VAS) (scaled 0 to 100) and the Profile of Mood States (POMS; Norcross et al. 1984), respectively, and were recorded at time points 0, 30, and 75 min.
Salivary cortisol concentrations were determined using competitive immunofluorescent assay kits from Salimetrics (State College, PA, USA). Each saliva sample was assayed in duplicate. Optical density was read on a Tecan plate reader (Mannedorf/Zurich, Switzerland) at 450 nm, using Biosoft’s Assay Zap software (Cambridge, UK). The intra-assay coefficient of variation (cv) was approximately 1.4% while the inter-assay cv was approximately 4.0%.
Statistical analyses were conducted using SPSS 16.0 for Windows (SPSS, Inc., Chicago, IL, USA). All analyses were two-tailed with alpha set to p<0.05. A standard Pearson correlation matrix was used to examine the relationships between five different maltreatment subtype scores. Descriptive statistics were used to characterize the sample (n=110). Cortisol values were positively skewed and therefore log-transformed to meet normal distribution requirements for statistical tests. Repeated measures General Linear Model (GLM) was used to determine the effects of maltreatment on cortisol reactivity to TSST in models that included CTQ data (summarized as total score for 28-item scale, dichotomized scores for each of five subscales, or as the total number of subscales scored positive for maltreatment), estrogen use (dichotomized), and subject age. Huynh–Feldt adjustment was made for violations of sphericity assumptions.
Post hoc analyses were constructed to examine more specifically the significant effect of physical abuse (PA), by comparing features from two groups based on the presence (n=20) or absence (n=90) of PA. Chi-square and t tests were used to test for baseline differences between these groups. Repeated measures GLMs examined significant effects of PA with regard to potential confounds: menstrual cycle phase (estimated by number of days from onset of last menstrual period to TSST), socioeconomic status (education status used as proxy), and recent (within past month) levels of perceived stress, current levels of depressive and anxiety symptoms, current or lifetime Axis I diagnosis, and other types of maltreatment. Post hoc power and effect size determinations were generated by the SPSS GLM repeated measures procedure, by electing the “partial eta squared” and “observed power” options provided in the analysis program by SPSS. The Bonferroni procedure was used to adjust for multiple comparisons by dividing the overall alpha (0.05) by 5 (representing five CTQ subscales), to yield p=0.0167 as the threshold for statistical significance.
Results
Relationship between maltreatment subtypes
Scores on the five CTQ subscales were significantly intercorrelated (all p<0.01), with Pearson correlation coefficients in the matrix ranging from r=0.38 (sexual abuse and emotional neglect) to r =0.80 (emotional abuse and emotional neglect). When threshold (moderate–severe) criteria were applied for dichotomization, all maltreatment subtypes remained significantly correlated with one another at the p<0.05 level except one (sexual abuse and emotional neglect, p=0.06). There were three subjects who reported exclusive emotional abuse, two subjects who reported exclusive PA, six reported exclusive sexual abuse, two reported exclusive emotional neglect, and one reported exclusive physical neglect.
Cortisol response to the TSST
All models revealed significant changes in salivary cortisol concentrations over time during the TSST. Given space limitations, detailed statistical results for significant GLM effects are limited to the group×time and between-groups analyses below.
Childhood maltreatment and cortisol responses
The total CTQ score was not a statistically significant predictor of the cortisol response to the TSST in the repeated measures GLM, but did impact the response curves at a trend level (group×time effect, F=1.2, p= 0.087). Individual models assessing the effects of moderate–severe maltreatment according to maltreatment type revealed that PA was a significant predictor of lower cortisol response to the TSST (effect of PA group—F= 4.95, p<0.005). Childhood PA was associated with lower cortisol responses to the TSST across time, but there was not a significant group×time effect of PA (Fig. 1). The effect of PA remained highly significant, even when scores for all other maltreatment subtypes (dichotomized) were entered into the model as covariates (F=15.83, p<0.001), and also after application of a Bonferroni correction factor. None of the other maltreatment types was significantly related to the salivary cortisol response to this test.
Fig. 1.
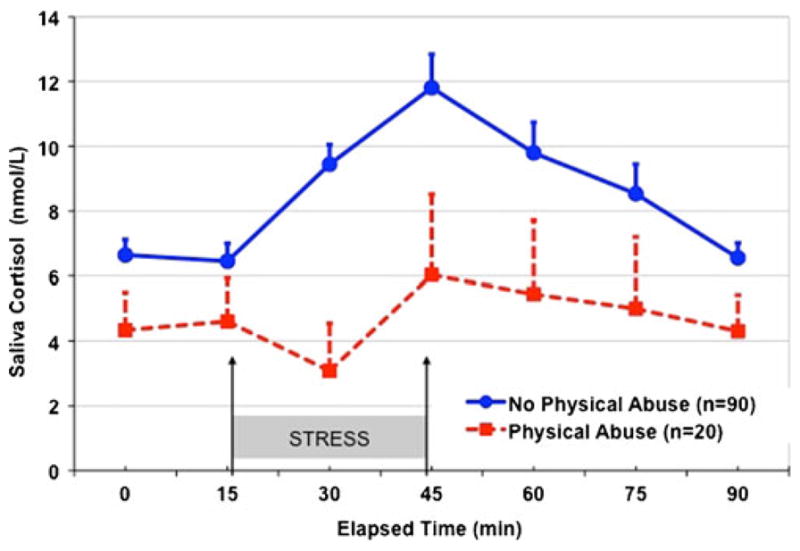
Salivary cortisol response to the TSST in medication-free adult women, grouped according to presence or absence of childhood physical abuse (moderate or severe on CTQ subscale)
Relationship of cortisol response with number of maltreatment subtypes
There were 58 subjects who reported no maltreatment at all, 14 subjects who reported having experienced only one type of maltreatment; 14 subjects reported two types, ten subjects reported three types, eight subjects reported four types, and six subjects reported all five maltreatment subtypes. There was no significant relationship between the number of different abuse/neglect subtypes (ranging from “none” to all five) endorsed by subjects and their cortisol responses to the TSST. The effect of PA remained robust when subjects with PA (n=20) were compared to the group (n=58) reporting no past maltreatment on any of the CTQ subscales (effect of group—F=5.9, p=0.017).
Comparison of subject groups defined by physical abuse
PA items on the CTQ included statements such as the following: “Family hit me so hard that it left me with bruises or marks”; “I was punished with a belt/board/cord/other hard object”; “I believe that I was physically abused”. Table 1 compares the clinical features of subject groups defined by the presence of PA (n=20 with PA, n=90 without PA). Individuals with PA were significantly older and had more current and lifetime Axis I disorders. There was no significant difference in the distribution of educational levels across the two groups. PA subjects were more likely to report all other subtypes of childhood maltreatment on CTQ subscales. Variables showing significant group differences were entered in post hoc GLMs as discussed below.
Table 1.
Characteristics of subjects in groups defined by physical abuse (PA)
| PA (n=20) | No PA (n=90) | p value | |
|---|---|---|---|
| Age (years) (mean±SD) | 36.5±12.5 | 29.1±10.4 | 0.007 |
| Estrogen use, n (%) | 4 (20.0) | 37 (41.1) | 0.077 |
| Years of education, n (%) | |||
| <12 years | 0 (0.0) | 1 (1.1) | |
| ≥12 years | 5 (25.0) | 44 (48.9) | |
| College graduate | 10 (50.0) | 34 (37.8) | |
| Professional degree | 5 (25.0) | 11 (12.2) | |
| Childhood trauma questionnaire—total (mean±SD) | 14.4±3.8 | 7.5±2.5 | 0.001 |
| Childhood trauma questionnaire subscales, n (%) (moderate to severe) | |||
| Emotional abuse | 17 (85.0) | 19 (21.1) | 0.001 |
| Emotional neglect | 14 (70.0) | 19 (21.1) | 0.001 |
| Sexual abuse | 10 (50.0) | 14 (15.6) | 0.001 |
| Physical neglect | 11 (55.0) | 10 (11.1) | 0.001 |
| Physical abuse | 20 (100.0) | 0 (0.0) | N/A |
| DSM axis I disorder, n (%) | |||
| Current | 9 (45.0) | 15 (16.7) | 0.006 |
| Lifetime | 16 (80.0) | 33 (36.7) | 0.001 |
| Inventory for depression symptomatology—self-report (mean±SD) | 23.6±15.3 | 12.8±8.3 | 0.006 |
| State–Trait Anxiety Scale (mean±SD) | |||
| State | 39.7±13.1 | 31.1±9.2 | 0.013 |
| Trait | 44.6±13.9 | 34.1±9.9 | 0.005 |
| Perceived stress scale (mean±SD) | 28.7±11.5 | 18.6±8.4 | 0.001 |
Effects of age and estrogen use
There was no significant effect found for subject age on cortisol response to TSST. A significant effect of estrogen use, as indicated by a significant within-subjects quadratic term contrast (F=9.3, p=0.003), showed that subjects taking estrogen had relatively greater cortisol release during the recovery phase of the response curve (i.e., after time point 30). When subjects not taking estrogen were examined separately (n=69), the above finding for PA group retained the same level of significance (F=16.1, p<0.001).
Post hoc testing for potential confounds
Age and estrogen use were controlled in the primary models described above. Additional post hoc models, controlling for the variables associated with PA, were conducted to ensure that the significant effects of PA were not attributable to these factors. There were no significant effects of education level, recent perceived stress (PSS), subclinical depressive symptomatology (IDS-SR, total score), state anxiety, or trait anxiety (STAI) on cortisol response and these variables did not influence the PA finding. The effect or PA remained significant when controlling for menstrual phase (among the subset of 101 women who were not post-menopausal; F=4.49, p<0.05). Furthermore, the main finding remained unchanged when categories of current diagnoses were examined independently as covariates (i.e., major depressive disorder, any depressive disorder, post-traumatic stress disorder) and when analyses were re-run excluding the subjects who endorsed SCID criteria for current major depressive episode (n=10) or current post-traumatic stress disorder (PTSD; n= 3). There were two subjects with PTSD from the PA group and one PTSD subject without a history of PA. When these three were excluded, the main finding (PA group effect) remained significant (F=8.4, p=0.005). History of a lifetime Axis I diagnosis did not produce any significant effects on cortisol response and did not diminish the significance of PA findings.
Effect of PA on physiological and emotional response to the stress challenge
Repeated measures GLMs using heart rate and blood pressure recordings during the TSST procedures as the repeated dependent variable showed no significant difference between subjects with and without a history of PA. Both groups showed transient increases in vital signs during the TSST as reflected by rise from baseline (time 0) to peak (30 min) and subsequent recovery toward baseline (75 min). Similarly, data from the POMS subscales showed both groups experienced equivalent stress-induced changes in tension/anxiety, elation, fatigue, depression, vigor, arousal, and positive mood. However, PA subjects had significantly greater overall scores for anger/hostility (multivariate F=6.6, p=0.002; between-groups F=6.1, p= 0.015) and confusion (between-groups F=4.3, p=0.04) during the acute stress challenge. Changes in anger and confusion scores during the TSST were not significantly correlated with cortisol response.
Effect size and power considerations
A partial eta-squared statistic generated by the GLM procedure in SPSS can be used to estimate the “proportion of total variation attributable to the factor, partialling out (excluding) other factors from the total nonerror variation” (Pierce et al. 2004). For our main analysis, which included five maltreatment subtypes, age, and estrogen use, the effect of PA group was associated with a partial eta squared of 0.14. This is considered a large effect (Kittler et al. 2007). Power of a statistical test is the probability that it will find a statistically significant difference, in this case between subjects with PA and without PA, as a function of the size of the true difference between those two populations. The observed power level for this PA group effect in our GLM was 0.98. It is thus unlikely that such a large effect would be detected by chance.
Discussion
In the present study involving a sample of 110 women from the community, we found a significantly lowered salivary cortisol response to a psychosocial stress task among subjects who reported a history of childhood physical abuse. This effect remained significant when we statistically controlled for the effect of estrogen use and restricted the sample to subjects not receiving estrogen-containing compounds. The results also remained significant when we compared subjects with physical abuse to a control group without physical abuse or any other type of maltreatment. As our results remained unchanged after exclusion of subjects with current major depressive disorder and post-traumatic stress disorder, we conclude that the difference in cortisol responsivity reflects a persistent alteration in the HPA axis independent of current psychopathology.
These results should be considered in light of earlier work by our group, which described a significant overall effect of early life maltreatment as flattening cortisol response to the TSST (Carpenter et al. 2007). In the regression analysis comparing separate maltreatment subtypes in that sample of 50 healthy adults, only a trend level (negative) effect was seen between PA and cortisol response. Here we report a statistically significant effect of PA, in the same direction. However, in the prior investigation, both emotional neglect and sexual abuse had significant and opposite effects on cortisol response to acute stress (TSST), with emotional neglect dampening cortisol reactivity and sexual abuse increasing it. Independent effects did not emerge for emotional neglect or sexual abuse in this sample, so we did not replicate these same maltreatment subtype findings with this subject cohort. In the prior study, we found a significant effect of maltreatment when all five subtypes were grouped together in one summary variable, but in the present study the same analysis strategy produced only a non-significant trend.
In the present study, we examined maltreatment subtypes separately, and here report statistically significant results specific to PA. There are several possible explanations to account for inconsistency across our two studies measuring cortisol response to TSST. Differences between the two sample populations or types of biological specimens are one consideration. The previous study included both males and females and was done with assessment of hormone response measured in plasma. The current study was conducted only in women and measured cortisol concentrations in saliva. Size of sample and/or the size of the subject subsets reporting different types of childhood maltreatment is another area of divergence. The total number of subjects in the previous study who reported moderate–severe PA was only 9, so those analyses may have been insufficiently powered to detect the PA finding we observed in the present study. Similarly, our failure to detect significant effects of sexual abuse and emotional neglect may also be in part attributable to the composition of the samples, since both maltreatment types were reported by a smaller proportion in this sample than in the previous study sample (sexual abuse, 22% versus 35%; emotional neglect, 30% versus 52%). The simultaneous presence of differential effects (that could cancel each other out when combined) across the five abuse subtypes is also a possibility, i.e., sexual abuse was found to significantly increase cortisol response, whereas emotional neglect was found to decrease it, in the prior study. Small sample sizes, insufficient power, and multiple statistic comparisons can contribute to chance findings and create apparent discrepancies from one study to the next. However, the effect size we found for PA on cortisol response was large, the p value withstood correction with the Bonferroni factor, and the observed power level was very high, so the finding is unlikely spurious.
It is important to note that most of the subjects with PA in the present investigation also reported additional type(s) of childhood maltreatment, so it was not possible for us to determine the effects of PA alone. A community sample of women evaluated with the CTQ found 30% reported at least one subtype of maltreatment, but nearly half of those reported the co-occurrence of two or more maltreatment subtypes (Scher et al. 2004). Recruitment of subjects with exclusive PA for research protocols like this could pose considerable feasibility challenges, but would permit the optimal design for isolating the effects of PA. We found PA remained significant even after statistically controlling for other types of maltreatment. While this study was not specifically designed to investigate the severity of trauma or the cumulative effect of experiencing multiple different forms of abuse or neglect experienced in childhood, the number of maltreatment types was not predictive of the cortisol response to the TSST.
Our results add to the existing literature on differential effects of childhood maltreatment subtypes that suggests PA may somehow act as a unique determinant of adult HPA axis reactivity. Using the CTQ subscales, Weissbecker et al. (2006) reported effects of PA on diurnal HPA function that were distinct from those of sexual abuse in women with fibromyalgia. Specifically, they found PA was associated with flattened diurnal salivary cortisol profiles. Flory et al. (2009) also demonstrated that PA was significantly related to lower plasma cortisol levels by performing linear regression analyses with five CTQ subscales data from a non-clinical sample with personality disorders. In contrast to PA, physical neglect emerged in that study as a significant effect in the opposite direction, i.e., associated with higher cortisol concentrations, after controlling for other forms of maltreatment. Consistent with our results, Flory and colleagues detected substantial overlap for the five maltreatment types in correlational analyses, but no significant relationship between cortisol and total CTQ score. Our findings lend additional support to the notion that the CTQ subscales capture distinct experiences that are not additive, but it remains unclear why physical abuse stands alone as a significant determinant of reduced cortisol concentrations in this collection of studies.
Other researchers have reported associations between adverse early life environment and cortisol hyporeactivity in non-clinical samples (Bellingrath and Kudielka 2008; Elzinga et al. 2008; Kraft and Luecken 2009), but our findings specifically link PA to cortisol hyporeactivity in healthy adults. Our data were not sufficiently detailed to reveal whether PA exposure was intermittent or chronic. Some have speculated that chronic abuse causes a HPA “burn-out” phenomenon in which persistently elevated cortisol levels during early neurodevelopment lead to lasting changes in the HPA axis that manifest as dampened cortisol responses to future stress (De Bellis 2002; Tarullo and Gunnar 2006). Another suggestion of “duration” or “timing” effects of maltreatment emerged from a regression analysis of variables that might predict HPA response to the TSST in a sample of adult women (Heim et al. 2002), some of whom had major depression or PTSD. While a (dichotomized) history of childhood (physical or sexual) abuse predicted higher peak hormone concentrations, that analysis also identified significant predictors of opposite direction effects, i.e., the number of childhood abuse events before puberty had a significant negative effect, while the number of traumatic events during or after puberty had a significant positive effect, on peak adrenocorticotropin (ACTH) concentrations. Corresponding analysis of cortisol data revealed that severity of adult (past month) stress exposure and the number of abuse events before puberty both predicted negative effects on peak responses to the stress test. We did not have data on the timing of stress exposure, relative to puberty, age, or other developmental milestones, and it is possible that our inability to statistically account for such effects in our analyses impacted the extent to which we were able to replicate the findings our past findings with regard to neglect (negative) and sexual abuse (positive) and cortisol stress response. The complexity of these and other findings reported to date suggests future neuroendocrine studies of childhood maltreatment will require large samples sizes to achieve the necessary statistical power for parsing out multiple effects embedded in stressful early environments.
Prior work from our own group examining childhood parental loss and adult HPA function (Tyrka et al. 2008) also highlights how multiple features of an early life stressor might determine whether cortisol reactivity is exaggerated or attenuated. The interaction between loss of a parent during childhood and the quality of care provided by the parents emerged as a complex relationship, such that parental desertion together with very low levels of parental care was associated with dampened cortisol responses to a standard neuroendocrine challenge test. When parental care was not taken into consideration, death or desertion of a parent during childhood was associated with increased cortisol responses, particularly in men. While the quality of parental care was not examined in the current study, one might expect poor quality parenting and low levels of parental care to characterize the early environment of those in our sample who reported childhood PA or other maltreatment types perpetrated by primary caregivers. Additional information from our sample of 110 women, such as the age at first exposure to PA, relationship with the perpetrator, availability of nurturing and supportive caretakers concurrent with PA, and the frequency or duration of the abuse during child and teen years, would also have allowed us to explore the data for these more subtle potential effects.
In addition to timing of stress exposure and contextual factors, gender and genes may account for our significant findings. Gender may mediate how different abuse subtypes shape HPA axis responses to stress (Kudielka and Kirschbaum 2005), or mediate the effect of genetic polymorphisms on stress response (Shalev et al. 2009; Wust et al. 2009). Our research group has recently shown an association between the candidate polymorphisms of the corticotropin-releasing hormone receptor gene (CRHR1) and cortisol response patterns in adults (Tyrka et al. 2010). Among subjects reporting childhood maltreatment, one specific genotype was associated with elevated cortisol responses to a neuroendocrine challenge test. The present study did not include genotyping, but future exploration of gene×environment interactions might profitably focus on self-reported childhood physical abuse and salivary cortisol response to acute stress challenge.
Strengths of our study include a sample population of paid volunteers drawn from the community who were not seeking psychiatric care. Additionally, our sample contained only women, which allowed for the isolation of HPA effects in females. We also controlled for use of estrogen-containing compounds and menstrual cycle phase, which have been shown to affect cortisol levels (Kirschbaum et al. 1999). Limitations of our study include its reliance on subjects’ recall. It is possible that some subjects had distorted memory of early environment (Hardt and Rutter 2004) or chose not to disclose their abuse. A sample even more homogenous than the one we recruited, with regard to age, health history, and estrogen use, would have reduced the potential for introducing confounds and eliminated the need for multiple covariates in our models. The CTQ scale we used does not characterize the specific timing, duration, or severity of the abuse/neglect exposure. As mentioned above, we did not examine contextual factors that may have mitigated the deleterious effects of the adverse early experiences, such as the quality and availability of social supports during or after exposure to childhood stressors. Finally, our subjects were well-educated, young, and generally healthy. As such, our sample may have consisted of subjects with an endophenotype that is adaptive, or otherwise more resilient, to the impact of early life adversity.
While a convergence of results from preclinical and clinical investigations indicates that various forms of chronic stress or deprivation might lead to dampened HPA axis reactivity, the clinical significance of relatively diminished cortisol response to provocative testing is not yet known. Blunted cortisol responses have been associated with chronic inability to withdraw from work obligations (Bellingrath and Kudielka 2008), cocaine relapse (Back et al. 2010), high anxiety sensitivity (Shirotsuki et al. 2009; Sjors et al. 2009), other subclinical mood/somatic symptoms (Brooks and Robles 2009), and with increased activity of the transcription factor nuclear factor-kappaB (NF-kappaB; a major inducer of inflammatory genes) (Wolf et al. 2009). Longitudinal evaluation of healthy individuals with dampened cortisol stress response patterns is needed to elucidate how these findings predict future mental and physical health outcomes.
Acknowledgments
Funding for this study was provided by NIMH Grant R01 MH068767 (LLC) and K23 MH067947 (ART). The authors report no disclosures relevant to this work. No therapeutic pharmaceutical or device products were utilized in this research protocol. The authors disclose the following biomedical financial interests and sources of support over the past 3 years and the foreseeable future. Drs. Tyrka, Price, and Carpenter have received grant/research support from the National Institutes of Health, NARSAD, Department of Defense, Sepracor, Cyberonics, Neuronetics, UCB Pharma, and Medtronic. Dr. Tyrka received honoraria for continuing medical education from Lundbeck and Takeda. Dr. Price has received speakers’ bureau honoraria from Jazz Pharmaceuticals and MD Conferences/Psychiatry Review Course, consultant income from Abbott, Gerson Lehrman, Wiley, Qatar National Research Fund, Alberta Heritage Foundation for Medical Research, Springer, and Lundbeck. Dr. Carpenter has served as a consultant or on an advisory board for Abbott, AstraZeneca, Cyberonics, Novartis, Neuronetics, and Wyeth, and has received honoraria for continuing medical education from AstraZeneca and speakers’ bureau honoraria from Cyberonics and Neuronetics. Dr. Geracioti received grant support from the National Institutes of Health, the Department of Veterans Affairs, and the Department of Defense; he is the principal equity holder of RxDino, LLC, a pharmaceutical company which is developing dual corticosteroids for dermatological indications. Dr. Thaddeus Shattuck discloses no outside support. The authors thank Kelly Colombo, B.A. for her assistance with data management and Nosa N. Ekhator, M.S. for his technical facility with the salivary cortisol assays.
Contributor Information
Linda L. Carpenter, Email: Linda_Carpenter_MD@Brown.edu, Mood Disorders Research Program and Laboratory for Clinical Neuroscience, Brown Department of Psychiatry and Human Behavior, Butler Hospital, 345 Blackstone Blvd, Providence, RI 02906, USA
Thaddeus T. Shattuck, Mood Disorders Research Program and Laboratory for Clinical Neuroscience, Brown Department of Psychiatry and Human Behavior, Butler Hospital, 345 Blackstone Blvd, Providence, RI 02906, USA
Audrey R. Tyrka, Mood Disorders Research Program and Laboratory for Clinical Neuroscience, Brown Department of Psychiatry and Human Behavior, Butler Hospital, 345 Blackstone Blvd, Providence, RI 02906, USA
Thomas D. Geracioti, Department of Psychiatry, University of Cincinnati College of Medicine and Veterans Affairs Medical Center, Cincinnati, OH, USA
Lawrence H. Price, Mood Disorders Research Program and Laboratory for Clinical Neuroscience, Brown Department of Psychiatry and Human Behavior, Butler Hospital, 345 Blackstone Blvd, Providence, RI 02906, USA
References
- Back SE, Hartwell K, DeSantis SM, Saladin M, McRae-Clark AL, Price KL, Moran-Santa Maria MM, Baker NL, Spratt E, Kreek MJ, Brady KT. Reactivity to laboratory stress provocation predicts relapse to cocaine. Drug Alcohol Depend. 2010;106:21–27. doi: 10.1016/j.drugalcdep.2009.07.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bellingrath S, Kudielka BM. Effort–reward-imbalance and overcommitment are associated with hypothalamus–pituitary–adrenal (HPA) axis responses to acute psychosocial stress in healthy working schoolteachers. Psychoneuroendocrinology. 2008;33:1335–1343. doi: 10.1016/j.psyneuen.2008.07.008. [DOI] [PubMed] [Google Scholar]
- Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, Stokes J, Handelsman L, Medrano M, Desmond D, Zule W. Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abuse Negl. 2003;27:169–190. doi: 10.1016/s0145-2134(02)00541-0. [DOI] [PubMed] [Google Scholar]
- Bremmer MA, Deeg DJ, Beekman AT, Penninx BW, Lips P, Hoogendijk WJ. Major depression in late life is associated with both hypo- and hypercortisolemia. Biol Psychiatry. 2007;62:479–486. doi: 10.1016/j.biopsych.2006.11.033. [DOI] [PubMed] [Google Scholar]
- Brooks KP, Robles TF. Recent depressive and anxious symptoms predict cortisol responses to stress in men. Psychoneuroendocrinology. 2009;34:1041–1049. doi: 10.1016/j.psyneuen.2009.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carpenter LL, Carvalho JP, Tyrka AR, Wier LM, Mello AF, Mello MF, Anderson GM, Wilkinson CW, Price LH. Decreased adrenocorticotropic hormone and cortisol responses to stress in healthy adults reporting significant childhood maltreatment. Biol Psychiatry. 2007;62:1080–1087. doi: 10.1016/j.biopsych.2007.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chopra KK, Ravindran A, Kennedy SH, Mackenzie B, Matthews S, Anisman H, Bagby RM, Farvolden P, Levitan RD. Sex differences in hormonal responses to a social stressor in chronic major depression. Psychoneuroendocrinology. 2009;34:1235–1241. doi: 10.1016/j.psyneuen.2009.03.014. [DOI] [PubMed] [Google Scholar]
- Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385–396. [PubMed] [Google Scholar]
- Danese A, Moffitt TE, Pariante CM, Ambler A, Poulton R, Caspi A. Elevated inflammation levels in depressed adults with a history of childhood maltreatment. Arch Gen Psychiatry. 2008;65:409–415. doi: 10.1001/archpsyc.65.4.409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Bellis MD. Developmental traumatology: a contributory mechanism for alcohol and substance use disorders. Psychoneuroendocrinology. 2002;27:155–170. doi: 10.1016/s0306-4530(01)00042-7. [DOI] [PubMed] [Google Scholar]
- Derijk RH, de Kloet ER. Corticosteroid receptor polymorphisms: determinants of vulnerability and resilience. Eur J Pharmacol. 2008;583:303–311. doi: 10.1016/j.ejphar.2007.11.072. [DOI] [PubMed] [Google Scholar]
- Dube SR, Anda RF, Felitti VJ, Chapman DP, Williamson DF, Giles WH. Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: findings from the adverse childhood experiences study. JAMA. 2001;286:3089–3096. doi: 10.1001/jama.286.24.3089. [DOI] [PubMed] [Google Scholar]
- Elzinga BM, Roelofs K, Tollenaar MS, Bakvis P, van Pelt J, Spinhoven P. Diminished cortisol responses to psychosocial stress associated with lifetime adverse events a study among healthy young subjects. Psychoneuroendocrinology. 2008;33:227–237. doi: 10.1016/j.psyneuen.2007.11.004. [DOI] [PubMed] [Google Scholar]
- Entringer S, Kumsta R, Hellhammer DH, Wadhwa PD, Wust S. Prenatal exposure to maternal psychosocial stress and HPA axis regulation in young adults. Horm Behav. 2009;55:292–298. doi: 10.1016/j.yhbeh.2008.11.006. [DOI] [PubMed] [Google Scholar]
- Fiocco AJ, Joober R, Lupien SJ. Education modulates cortisol reactivity to the Trier Social Stress Test in middle-aged adults. Psychoneuroendocrinology. 2007;32:1158–1163. doi: 10.1016/j.psyneuen.2007.08.008. [DOI] [PubMed] [Google Scholar]
- First MB, Spitzer RL, Gibbon M, Williams JB. Structured clinical interview for DSM-IV axis I disorders, patient edition (SCIP-I/P) New York State Psychiatric Institute, Biometrics Research; New York: 1996. [Google Scholar]
- Flory JD, Yehuda R, Grossman R, New AS, Mitropoulou V, Siever LJ. Childhood trauma and basal cortisol in people with personality disorders. Compr Psychiatry. 2009;50:34–37. doi: 10.1016/j.comppsych.2008.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hardt J, Rutter M. Validity of adult retrospective reports of adverse childhood experiences: review of the evidence. J Child Psychol Psychiatry. 2004;45:260–273. doi: 10.1111/j.1469-7610.2004.00218.x. [DOI] [PubMed] [Google Scholar]
- Heim C, Newport DJ, Heit S, Graham YP, Wilcox M, Bonsall R, Miller AH, Nemeroff CB. Pituitary–adrenal and autonomic responses to stress in women after sexual and physical abuse in childhood. JAMA. 2000;284:592–597. doi: 10.1001/jama.284.5.592. [DOI] [PubMed] [Google Scholar]
- Heim C, Newport DJ, Wagner D, Wilcox MM, Miller AH, Nemeroff CB. The role of early adverse experience and adulthood stress in the prediction of neuroendocrine stress reactivity in women: a multiple regression analysis. Depress Anxiety. 2002;15:117–125. doi: 10.1002/da.10015. [DOI] [PubMed] [Google Scholar]
- Ising M, Depping AM, Siebertz A, Lucae S, Unschuld PG, Kloiber S, Horstmann S, Uhr M, Muller-Myhsok B, Holsboer F. Polymorphisms in the FKBP5 gene region modulate recovery from psychosocial stress in healthy controls. Eur J Neurosci. 2008;28:389–398. doi: 10.1111/j.1460-9568.2008.06332.x. [DOI] [PubMed] [Google Scholar]
- Kajantie E, Feldt K, Raikkonen K, Phillips DI, Osmond C, Heinonen K, Pesonen AK, Andersson S, Barker DJ, Eriksson JG. Body size at birth predicts hypothalamic–pituitary–adrenal axis response to psychosocial stress at age 60 to 70 years. J Clin Endocrinol Metab. 2007;92:4094–4100. doi: 10.1210/jc.2007-1539. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Magee WJ. Childhood adversities and adult depression: basic patterns of association in a US national survey. Psychol Med. 1993;23:679–690. doi: 10.1017/s0033291700025460. [DOI] [PubMed] [Google Scholar]
- Kirschbaum C, Kudielka BM, Gaab J, Schommer NC, Hellhammer DH. Impact of gender, menstrual cycle phase, and oral contraceptives on the activity of the hypothalamus–pituitary–adrenal axis. Psychosom Med. 1999;61:154–162. doi: 10.1097/00006842-199903000-00006. [DOI] [PubMed] [Google Scholar]
- Kittler JE, Menard W, Phillips KA. Weight concerns in individuals with body dysmorphic disorder. Eat Behav. 2007;8:115–120. doi: 10.1016/j.eatbeh.2006.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kraft AJ, Luecken LJ. Childhood parental divorce and cortisol in young adulthood: evidence for mediation by family income. Psychoneuroendocrinology. 2009;34:1363–1369. doi: 10.1016/j.psyneuen.2009.04.008. [DOI] [PubMed] [Google Scholar]
- Kudielka BM, Kirschbaum C. Sex differences in HPA axis responses to stress: a review. Biol Psychol. 2005;69:113–132. doi: 10.1016/j.biopsycho.2004.11.009. [DOI] [PubMed] [Google Scholar]
- Kudielka BM, Hellhammer DH, Wüst S. Why do we respond so differently? Reviewing determinants of human salivary cortisol responses to challenge. Psychoneuroendocrinology. 2009;34:2–18. doi: 10.1016/j.psyneuen.2008.10.004. [DOI] [PubMed] [Google Scholar]
- Kumsta R, Entringer S, Koper JW, van Rossum EF, Hellhammer DH, Wust S. Sex specific associations between common glucocorticoid receptor gene variants and hypothalamus–pituitary–adrenal axis responses to psychosocial stress. Biol Psychiatry. 2007;62:863–869. doi: 10.1016/j.biopsych.2007.04.013. [DOI] [PubMed] [Google Scholar]
- Molnar BE, Buka SL, Kessler RC. Child sexual abuse and subsequent psychopathology: results from the National Comorbidity Survey. Am J Public Health. 2001;91:753–760. doi: 10.2105/ajph.91.5.753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Norcross JC, Guadagnoli E, Prochaska JO. Factor structure of the Profile of Mood States (POMS): two partial replications. J Clin Psychol. 1984;40:1270–1277. doi: 10.1002/1097-4679(198409)40:5<1270::aid-jclp2270400526>3.0.co;2-7. [DOI] [PubMed] [Google Scholar]
- Pierce CA, Block RA, Aguinis H. Cautionary note on reporting eta-squared values from multifactor ANOVA designs. Educ Psychol Meas. 2004;64:916–924. [Google Scholar]
- Roy A. Urinary free cortisol and childhood trauma in cocaine dependent adults. J Psychiatr Res. 2002;36:173–177. doi: 10.1016/s0022-3956(02)00002-x. [DOI] [PubMed] [Google Scholar]
- Rush AJ, Gullion CM, Basco MR, Jarrett RB, Trivedi MH. The Inventory of Depressive Symptomatology (IDS): psychometric properties. Psychol Med. 1996;26:477–486. doi: 10.1017/s0033291700035558. [DOI] [PubMed] [Google Scholar]
- Schafer I, Teske L, Schulze-Thusing J, Homann K, Reimer J, Haasen C, Hissbach J, Wiedemann K. Impact of childhood trauma on hypothalamus–pituitary–adrenal axis activity in alcohol-dependent patients. Eur Addict Res. 2010;16:108–114. doi: 10.1159/000294362. [DOI] [PubMed] [Google Scholar]
- Scher CD, Forde DR, McQuaid JR, Stein MB. Prevalence and demographic correlates of childhood maltreatment in an adult community sample. Child Abuse Negl. 2004;28:167–180. doi: 10.1016/j.chiabu.2003.09.012. [DOI] [PubMed] [Google Scholar]
- Shalev I, Lerer E, Israel S, Uzefovsky F, Gritsenko I, Mankuta D, Ebstein RP, Kaitz M. BDNF Val66Met polymorphism is associated with HPA axis reactivity to psychological stress characterized by genotype and gender interactions. Psychoneuroendocrinology. 2009;34:382–388. doi: 10.1016/j.psyneuen.2008.09.017. [DOI] [PubMed] [Google Scholar]
- Shirotsuki K, Izawa S, Sugaya N, Yamada KC, Ogawa N, Ouchi Y, Nagano Y, Nomura S. Salivary cortisol and DHEA reactivity to psychosocial stress in socially anxious males. Int J Psychophysiol. 2009;72:198–203. doi: 10.1016/j.ijpsycho.2008.12.010. [DOI] [PubMed] [Google Scholar]
- Sjors A, Larsson B, Karlson B, Osterberg K, Dahlman J, Gerdle B. Salivary cortisol response to acute stress and its relation to psychological factors in women with chronic trapezius myalgia —a pilot study. Psychoneuroendocrinology. 2009;35:674–685. doi: 10.1016/j.psyneuen.2009.10.007. [DOI] [PubMed] [Google Scholar]
- Spielberger CD. Manual for the state–trait anxiety inventory (form Y) Consulting Psychologists Press; Palo Alto: 1983. [Google Scholar]
- Tarullo AR, Gunnar MR. Child maltreatment and the developing HPA axis. Horm Behav. 2006;50:632–639. doi: 10.1016/j.yhbeh.2006.06.010. [DOI] [PubMed] [Google Scholar]
- Tyrka AR, Wier L, Price LH, Ross N, Anderson GM, Wilkinson CW, Carpenter LL. Childhood parental loss and adult hypothalamic–pituitary–adrenal function. Biol Psychiatry. 2008;63:1147–1154. doi: 10.1016/j.biopsych.2008.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tyrka AR, Price LH, Kao HT, Porton B, Marsella SA, Carpenter LL. Childhood maltreatment and telomere shortening: preliminary support for an effect of early stress on cellular aging. Biol Psychiatry. 2010;67:531–534. doi: 10.1016/j.biopsych.2009.08.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weissbecker I, Floyd A, Dedert E, Salmon P, Sephton S. Childhood trauma and diurnal cortisol disruption in fibromyalgia syndrome. Psychoneuroendocrinology. 2006;31:312–324. doi: 10.1016/j.psyneuen.2005.08.009. [DOI] [PubMed] [Google Scholar]
- Wolf JM, Rohleder N, Bierhaus A, Nawroth PP, Kirschbaum C. Determinants of the NF-kappaB response to acute psychosocial stress in humans. Brain Behav Immun. 2009;23:742–749. doi: 10.1016/j.bbi.2008.09.009. [DOI] [PubMed] [Google Scholar]
- Wust S, Kumsta R, Treutlein J, Frank J, Entringer S, Schulze TG, Rietschel M. Sex-specific association between the 5-HTT gene-linked polymorphic region and basal cortisol secretion. Psychoneuroendocrinology. 2009;34:972–982. doi: 10.1016/j.psyneuen.2009.01.011. [DOI] [PubMed] [Google Scholar]