

This article discusses new and future treatments for senior men with advanced prostate cancer that progresses during or after docetaxel therapy.
Keywords: Advanced, Senior adults, Treatment, Metastatic, Prostate
Abstract
The landscape of treatment for advanced prostate cancer is continually evolving as new therapies are developed and guidelines are constantly updated. However, the management of older men with advanced disease is not optimal. Many men are denied chemotherapy based on their chronological age, not their health status. Androgen-deprivation therapy (ADT) remains the mainstay of first-line treatment of advanced disease. Once the disease becomes resistant to castration, docetaxel-based chemotherapy is the regulatory-approved standard of care, irrespective of age. The place of weekly docetaxel in patients with poor performance status and signs of frailty has to be further evaluated in clinical studies. New treatments are now available, or on the horizon, for disease that progresses during or after docetaxel therapy. Cabazitaxel and abiraterone have been shown to prolong survival, irrespective of age, and are already in clinical use having received regulatory approval. The optimal sequence for these two agents is still unknown, although there is some indication that in patients predicted to be poor responders to abiraterone (high Gleason score, progression during docetaxel therapy, rapid progression to castrate-resistant prostate cancer with ADT) cabazitaxel should be the preferred choice. Further advances are being investigated, with promising data reported from phase III trials.
Introduction
The current rate of population aging is unprecedented, and the fastest growing segment is that aged 80 years or older, which increased from 13.8 million in 1950 to 69.2 million in 2000; it is expected to further rise to 379.0 million by 2050 [1]. As a consequence, the burden of prostate cancer is expected to increase by 55% by 2030 [2]. On one hand, prostate-specific antigen (PSA) screening has led to overdiagnosis and overtreatment of prostate cancer in younger men [3]; on the other hand, older men tend to have more aggressive tumors [4], but only a minority receive curative therapy [5]. This may partially explain why two out of three deaths due to prostate cancer occur in men over the age of 75 years [6].
Management of advanced prostate cancer is not optimal in senior adults. Despite clear benefits of chemotherapy in terms of survival, tumor response, and quality of life, physicians are still reluctant to use chemotherapy in older patients because of concerns about its toxicity [7]. In contradiction to this, a majority of older patients wish to be treated as younger patients for a potential survival benefit, and they are willing to accept the risks of chemotherapy [8].
Life expectancy is highly variable between individuals, mainly due to differences in health status. The median life expectancy of a 70-year-old man in the Social Security Administration tables is 12.4 years, but a healthy man may live at least another 18 years, whereas one with comorbid conditions is expected to live for only 6.7 more years [9]. Treatment advances are contributing to increased life expectancy in men with advanced prostate cancer in early and advanced settings [10, 11].
In practice, limitations to chemotherapy use are more related to associated comorbid conditions and poor performance status than chronological age [7]. Management of patients with advanced prostate cancer should be guided by an adequate evaluation of health status, as per the International Society of Geriatric Oncology guidelines [12, 13]. This article reviews the management of advanced prostate cancer and outlines specific considerations that need to be applied to the elderly population.
First-Line Androgen-Deprivation Therapy
Androgen-deprivation therapy (ADT)—usually with the use of a single-agent luteinizing hormone-releasing hormone (LHRH) agonist or by surgical castration—is the standard approach for the first-line treatment of patients with advanced prostate cancer [14]. The value of further addition of antiandrogens in the long term to achieve maximum androgen blockade is still debated. It provides a marginal survival advantage compared to LHRH agonists alone, and it is associated with increased costs, side effects, and impairment in patients' quality of life (Fig. 1) [14, 15].
Figure 1.
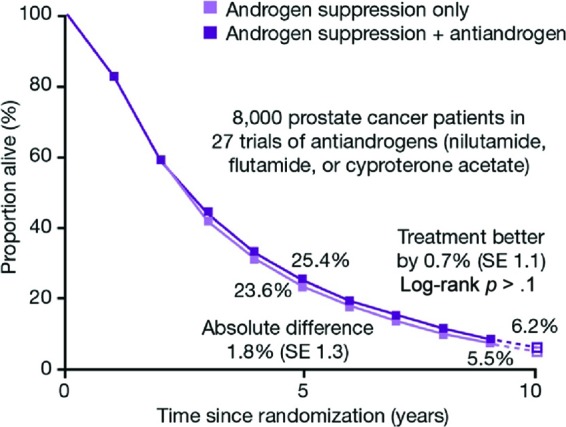
Total androgen blockade can provide a small increase in overall survival, but has significant effects on quality of life. Abbreviation: SE, standard error. Adapted from Prostate Cancer Trialists Collaborative Group. Maximum androgen blockade in advanced prostate cancer: An overview of the randomised trials. Lancet 2000;355:1491–1498, with permission.
However, at some point during their treatment, most patients with advanced prostate cancer will likely receive antiandrogen treatment [16]. In patients with progressive disease despite ADT, antiandrogen withdrawal has been shown to result in a PSA response (PSA decline of at least 50%) for a median duration of 3.5–5.0 months in 15–30% of patients [17–19]. PSA response following antiandrogen withdrawal is thought to be due to changes in the androgen signaling cascade, resulting in the antiandrogen acting as an activator, rather than an inhibitor, of the androgen receptor (AR) [20].
A phase III study of antiandrogen withdrawal, with or without ketoconazole in senior patients (median age, 72 years) with metastatic androgen-independent prostate cancer, demonstrated a significantly greater percentage of patients achieving PSA response with the addition of ketoconazole compared with antiandrogen withdrawal alone (27% vs. 11%, p = .0002) [16]. In a Southwest Oncology Group study (SWOG 9426) of antiandrogen withdrawal in 210 patients with progressive prostate cancer, after a median follow-up of 5 years, PSA responses following antiandrogen withdrawal were observed in 21% of patients [21]. Although the median progression-free survival among the study population was 3 months, 19% of patients experienced progression-free survival times of 12 months or greater. These data demonstrate that antiandrogen withdrawal can potentially result in PSA response and prolonged progression-free survival in a small number of patients.
The side effects of ADT include loss of bone density, with an increased risk of osteoporosis and a cumulative increase in the incidence of fractures [22, 23]. It is recommended that all men receiving ADT should therefore receive calcium and vitamin D supplementation, and baseline bone mineral density should be determined. Bisphosphonates or denosumab may be used if there is a documented risk for fracture or castrate-resistant prostate cancer (CRPC) with skeletal metastases [12, 13, 24, 25]. There is also a risk of metabolic side effects, diabetes, and fatal cardiac events [26–29]. Particular care should be taken with ADT in senior adults if the patient has a history of stroke, chronic heart failure, or myocardial infarction.
Sipuleucel-T is an active cellular immunotherapy that has reported efficacy in men with metastatic castrate-resistant prostate cancer (mCRPC) who have previously received ADT [30]. In a randomized phase III study, patients underwent leukapheresis and then received sipuleucel-T or placebo. The results demonstrated a relative reduction of 22% in the risk of death in the sipuleucel-T group compared with the placebo group, representing a 4.1-month improvement in median survival with sipuleucel-T. Despite this apparent survival benefit in senior men with prostate cancer (median age of patients in the sipuleucel-T group was 72 years), concerns about the study design have brought the results into concerns [31, 32]. One area of concern is the control group, where two-thirds of the collected peripheral-blood mononuclear cells (PBMCs) were not reinfused but were instead cryopreserved for possible use in a salvage study, meaning that the placebo group, but not the sipuleucel-T group, experienced repeated cell loss [30]. Also of note is that the sipuleucel-T treatment involves culturing the collected PBMCs with a chimeric protein containing granulocyte-macrophage colony-stimulating factor, whereas the placebo group PBMCs were cultured in collection medium without granulocyte-macrophage colony-stimulating factor. The presence or absence of tumor antigen was not, therefore, the only variable between the two groups.
Data that became available only after the U.S. Food and Drug Administration approval of sipuleucel-T showed that the treatment had no survival effect in patients under 65 years of age, in contrast to those aged 65 years or older where the hazard ratio (HR) for death favored sipuleucel-T [33]. These data suggest that the clinical benefit observed in the phase III trial of sipuleucel-T was driven by the effect in patients aged 65 years and older, and that in these older patients with mCRPC, sipuleucel-T may provide a survival benefit.
First-Line Chemotherapy
Virtually all patients who receive ADT will undergo disease progression to a castrate-resistant state within a median of 18 to 24 months [34]. Until 2004, there was no evidence that any treatment would offer a survival benefit for men with mCRPC. Some chemotherapy regimens had been trialed in this setting, but the condition was largely regarded as chemoresistant. Mitoxantrone was the most commonly used chemotherapeutic agent because of its palliative effects in men with mCRPC [35].
This view changed when results of two landmark randomized phase III trials demonstrated a survival benefit with docetaxel plus prednisone (Taxotere) for the first time in men with mCRPC compared with mitoxantrone plus prednisone [11, 36]. Docetaxel-based chemotherapy also demonstrated improvements in pain, PSA and quality of life in these patients. Moreover, in analysis of patients by age (<65, ≥65, and ≥75 years), the survival benefit of docetaxel was apparent for each of the groups (Fig. 2) [37]. A 2011 exploratory analysis of the TAX (Taxotere) 327 trial, focusing on the 267 men aged 75 years or older, concluded that older men had slightly more dose reductions and discontinuations for adverse events with docetaxel than mitoxantrone, but there was a trend for better improvement in quality of life, tumor response, and survival with the docetaxel 3-weekly schedule [38]. These data established docetaxel 75 mg/m2 every 3 weeks as the standard of care for first-line chemotherapy for prostate cancer, irrespective of age.
Figure 2.

Docetaxel provides a survival benefit regardless of age group. Abbreviations: ITT, intention to treat; KPS, Karnofsky performance status. Adapted from de Wit R. New hope for patients with metastatic hormone-refractory prostate cancer. Eur Urol 2006;5:817–823, with permission.
However, the tolerability of the docetaxel 3-weekly regimen has not been specifically studied in frail senior adults with poor performance status and severe comorbidities. Although weekly docetaxel is not registered for the treatment of mCRPC, it is often perceived to have less hematologic side effects compared with the 3-weekly regimen, especially in senior adults. Hence, a randomized phase II study comparing weekly docetaxel (30 mg/m2) plus prednisone with prednisone alone in 109 older men (median age, 70 years) with mCRPC evidenced a significant survival benefit for weekly docetaxel (27 months vs. 18 months) associated with improvements in pain, quality of life, and PSA response [39]. The main adverse events were nonhematologic toxicities (nail changes, alopecia, conjunctivitis, asthenia) and no febrile neutropenia was reported.
Progression After First-Line Docetaxel
Previously, once mCRPC had progressed during or following docetaxel therapy, the remaining treatment options were limited. However, in 2010 and 2011 respectively, evidence was published showing that the chemotherapy agent cabazitaxel and the hormonal treatment abiraterone offered a survival benefit in the postdocetaxel setting.
Cabazitaxel, a next-generation taxane, was developed following research to identify a drug that could overcome taxane resistance. Cabazitaxel was shown to be as effective as docetaxel against docetaxel-sensitive cell lines and tumor models, and it was active against in vitro and in vivo docetaxel-resistant tumor models [40, 41]. In the phase III TROPIC trial, cabazitaxel provided a 30% survival benefit versus mitoxantrone (15.1 months vs. 12.7 months; HR: 0.70, p < .0001) in patients who had progressed during or after docetaxel therapy (Fig. 3) [42]. After 2 years, 28% of patients in the cabazitaxel group were still alive compared with 17% in the mitoxantrone group. The median patient age was 68 years, and 18% of participants were aged 75 years or over. When stratified by age, the overall survival benefit with cabazitaxel was consistent irrespective of age.
Figure 3.

Cabazitaxel improves overall survival versus mitoxantrone regardless of age. Abbreviations: CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; PSA, prostate-specific antigen. Adapted from de Bono JS, Outard S, Ozguroglu M et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010;376:1147–1154, with permission.
Abiraterone—a potent inhibitor of cytochrome P450c17 (CYP17), a critical enzyme in androgen synthesis—has also demonstrated a significant survival benefit versus placebo in a phase III trial in patients who had progressed during or after docetaxel therapy (14.8 months vs. 10.9 months; HR: 0.65, p < .0001) [43]. The study population had a median age of 69 years, and 28% of participants were aged 75 years or over. When overall survival was assessed according to age group (<65, ≥65, or ≥75 years), the data demonstrated a consistent benefit of abiraterone in all groups (Fig. 4) [43].
Figure 4.

Abiraterone improves overall survival versus placebo regardless of age. Abbreviations: BPI, Brief Pain Inventory; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; OS, overall survival; PSA, prostate-specific antigen. Adapted from de Bono JS, Logothetis CJ, Molina A et al. Abiraterone and increased survival in metastatic prostate cancer. N Eng J Med 2011;364:1995–2005, with permission.
Table 1 summarizes the available data for docetaxel, cabazitaxel, and abiraterone in older men with prostate cancer [11, 42, 43]. There are side effects associated with both cabazitaxel and abiraterone, and particular care should be taken to manage these in senior patients with advanced disease [42, 43].
Table 1.
Docetaxel, cabazitaxel, and abiraterone in older men
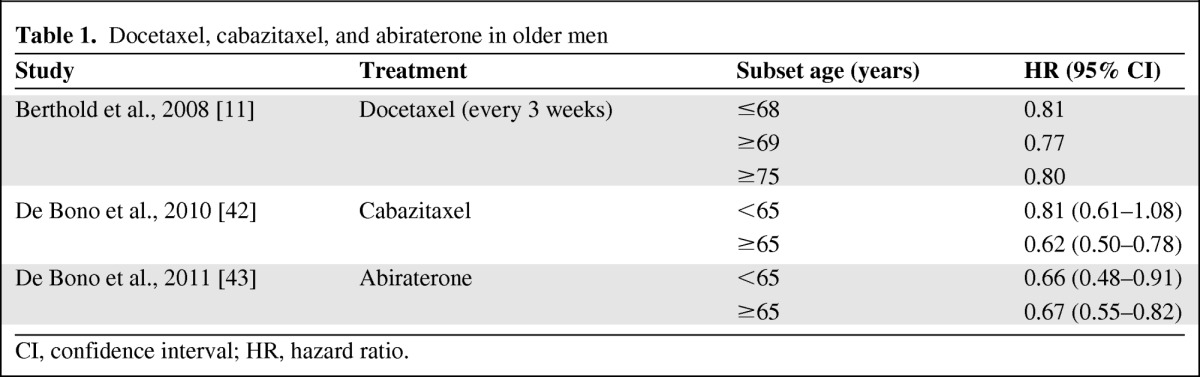
CI, confidence interval; HR, hazard ratio.
The TROPIC trial identified an increased risk of febrile neutropenia in cabazitaxel recipients (8% vs. 1% with mitoxantrone), which may be explained by the fact that patients had advanced disease and were heavily pretreated, including with radiation therapy [42]. These patients should be managed using primary prophylaxis with granulocyte colony-stimulating factor (G-CSF) where appropriate, as set out by the European Organisation for Research and Treatment of Cancer (EORTC) [44]. Cabazitaxel is also associated with an increased incidence of grade ≥3 diarrhea (6% vs. 1% with mitoxantrone), which can be a significant problem in elderly patients who are less mobile and are more prone to dehydration as a consequence of gastrointestinal problems [42]. Diarrhea—which may be reduced in patients receiving G-CSF [45]—should be managed adequately as soon as it occurs, with rehydration, adapted diet, and the use of antidiarrheal treatments as required. Proactive management of these side effects is needed to avoid treatment discontinuation and optimize efficacy of therapy.
Abiraterone is associated with an increased risk of hypokalemia, hypertension, and fluid retention (versus placebo), caused by an excess of mineralocorticoid [43]. Abiraterone should therefore be used with caution in patients with cardiovascular disease. Adrenocortical insufficiency may also occur with abiraterone use, and particular caution should be taken if daily steroid use is interrupted or infection occurs. Liver function should be monitored due to the risk of hepatotoxicity with abiraterone. Interestingly, abiraterone has recently been shown to be active in patients not preexposed to docetaxel but is not yet registered in this setting [46].
To date, no data are available to guide clinicians and patients in the optimal sequencing of cabazitaxel and abiraterone in the postdocetaxel setting. However, there is evidence to suggest that patients with a Gleason score of 8–10 or with a 16-month median delay in progression to CRPC with ADT are poor responders to subsequent endocrine manipulations including abiraterone [47, 48]. Similarly, patients with docetaxel-refractory disease do not seem to respond to abiraterone [49], whereas cabazitaxel has demonstrated a significant survival benefit in patients progressing during docetaxel therapy [42, 50]. Patient preference and disease aggressiveness may determine the first choice of treatment.
Bone-Modifying Agents
A frequent and often neglected issue with androgen deprivation is the loss of bone mass. While bisphosphonates in general have been approved for the treatment of osteoporosis, denosumab, a monoclonal antibody against RANKL, has been specifically approved for the prevention of bone loss in men receiving ADT for prostate cancer [51]. Approximately three-quarters of patients with prostate cancer develop bone metastases, often at the first diagnosis of metastatic disease [52]. Until recently, bisphosphonates were the only bone-targeted supportive treatment available [24, 53].
Denosumab has also received regulatory approval in the U.S. and Europe for preventing skeletal-related events in patients with bone metastases from solid tumors. Results from a phase III trial demonstrated that denosumab could significantly reduce the incidence of new vertebral fractures and prevent loss of bone density in men receiving ADT for prostate cancer [54]. Among the study population of this trial, 83% of the men were aged 70 years or older.
Future Treatment Options
Promising new treatment options for patients having progressed after docetaxel are expected to arrive in the near future. Enzalutamide is a first-in-class AR-signaling inhibitor. It blocks multiple steps in androgen signaling, including the binding of androgens to the AR, the nuclear translocation of AR, and the association of AR with DNA [55]. The effectiveness of enzalutamide in patients pretreated with docetaxel was assessed in the phase III AFFIRM (A Study Evaluating the Efficacy and Safety of the Investigational Drug MDV3100) study [56]. Results showed that enzalutamide can improve median overall survival by 4.8 months compared with placebo, and that its efficacy was comparable in patients younger than 65 and older than 65 years of age.
Radium-223 chloride (Alpharadin) is a new radioisotope that induces double-strand DNA breaks in adjacent tumor cells [57]. Due to the short penetration of alpha emitters, radium-223 chloride causes highly localized cell death with limited damage to surrounding normal tissue. Data from the phase III ALSYMPCA (ALpharadin in SYMptomatic Prostate CAncer) study showed that radium-223 chloride improved overall survival versus placebo (14.0 vs. 11.2 months) in patients with symptomatic bone metastases [58].
Conclusion
The management of advanced prostate cancer in senior adults is rapidly evolving with the development of new drugs able to prolong survival. Treatment decisions in this population should be based on health status (which mainly depends on the severity of comorbidities) and patient preferences, not chronological age.
ADT remains the first-line treatment in hormone-sensitive metastatic prostate cancer. In a senior adult population, evaluation of bone mineral status and prevention of osteoporosis (which may be by treatment with bisphosphonates or denosumab) are recommended.
In mCRPC, chemotherapy with docetaxel (75 mg/m2 every 3 weeks) is the present regulatory-approved standard of care, irrespective of age. The tolerability of the docetaxel 3-weekly regimen has not been specifically studied in frail older men. The place of weekly docetaxel in mCRPC should be further evaluated in this patient group.
In patients progressing during or after docetaxel, cabazitaxel and abiraterone have both been shown to prolong survival, irrespective of age. Optimal sequencing of these two agents is not known as yet but preliminary data suggest that cabazitaxel might be the preferred choice in patients with high Gleason score, patients progressing during docetaxel therapy, and patients progressing rapidly to CRPC with ADT. With cabazitaxel, care should be taken to control the risk of febrile neutropenia and diarrhea, which can be reduced with prophylactic G-CSF (as per EORTC guidelines) and proactive management of side effects. Abiraterone should be used with caution in patients with cardiovascular disease due to an increased risk of hypokalemia, hypertension, and fluid retention; regular liver test monitoring is needed due to the risk of hepatotoxicity. Rare cases of adrenocortical insufficiency have also been reported, especially when daily steroids are interrupted and infection occurs.
Although these treatment options have the potential to offer survival benefits to all men with advanced prostate cancer, there is still a need for more senior men to be included in specific advanced prostate cancer clinical trials to better understand potential limitations related to comorbidities. Further advances, such as enzalutamide and radium-223 chloride, are being investigated with promising data reported from phase III trials.
Acknowledgments
Medical Writer Assistance: Assisted, Julie Knight, Succinct Healthcare Communications, provided copyediting/proofreading, editorial, and production assistance.
Footnotes
- (C/A)
- Consulting/advisory relationship
- (RF)
- Research funding
- (E)
- Employment
- (H)
- Honoraria received
- (OI)
- Ownership interests
- (IP)
- Intellectual property rights/inventor/patent holder
- (SAB)
- Scientific advisory board
References
- 1.United Nations Department of Economic and Social Affairs Population Division. World population ageing: 1950–2050. [Accessed June 1, 2012]. Available at http://www.un.org/esa/population/publications/worldageing19502050/
- 2.Smith BD, Smith GL, Hurria A, et al. Future of cancer incidence in the United States: Burdens upon an aging, changing nation. J Clin Oncol. 2009;27:2758–2765. doi: 10.1200/JCO.2008.20.8983. [DOI] [PubMed] [Google Scholar]
- 3.Schröder FH, Hugosson J, Roobol MJ, et al. Screening and prostate cancer mortality in a randomized European study. N Engl J Med. 2009;360:1320–1328. doi: 10.1056/NEJMoa0810084. [DOI] [PubMed] [Google Scholar]
- 4.Sun L, Caire AA, Robertson CN, et al. Men older than 70 years have higher risk prostate cancer and poorer survival in the early and late prostate specific antigen eras. J Urol. 2009;182:2242–2249. doi: 10.1016/j.juro.2009.07.034. [DOI] [PubMed] [Google Scholar]
- 5.Hamilton AS, Albertsen PC, Johnson TK, et al. Trends in the treatment of localized prostate cancer using supplemented cancer registry data. BJU Int. 2010;107:576–584. doi: 10.1111/j.1464-410X.2010.09514.x. [DOI] [PubMed] [Google Scholar]
- 6.Northern Ireland Cancer Registry. Cancer of the prostate (ICD-9 185) Belfast, Ireland: Northern Ireland Cancer Registry; 1995. [Google Scholar]
- 7.Anderson J, van Poppel H, Bellmunt J, et al. Chemotherapy for older patients with prostate cancer. BJU Int. 2006;88:269–273. doi: 10.1111/j.1464-410X.2006.06526.x. [DOI] [PubMed] [Google Scholar]
- 8.Extermann M, Albrand G, Chen H, et al. Are older French patients as willing as older American patients to undertake chemotherapy? J Clin Oncol. 2003;21:3214–3219. doi: 10.1200/JCO.2003.08.091. [DOI] [PubMed] [Google Scholar]
- 9.Walter LC, Covinsky KE. Cancer screening in elderly patients: A framework for individualized decision making. JAMA. 2001;285:2750–2756. doi: 10.1001/jama.285.21.2750. [DOI] [PubMed] [Google Scholar]
- 10.Pagliarulo V, Bracarda S, Eisenberger MA, et al. Contemporary role of androgen deprivation therapy for prostate cancer. J Clin Oncol. 2012;61:11–25. doi: 10.1016/j.eururo.2011.08.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Berthold DR, Pond GR, Soban F, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer: Updated survival in the TAX 327 study. J Clin Oncol. 2008;26:242–245. doi: 10.1200/JCO.2007.12.4008. [DOI] [PubMed] [Google Scholar]
- 12.Droz JP, Balducci L, Bolla M, et al. Management of prostate cancer in older men: Recommendations of a working group of the International Society of Geriatric Oncology. BJU Int. 2010;106:462–469. doi: 10.1111/j.1464-410X.2010.09334.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Droz JP, Balducci L, Bolla M, et al. Background for the proposal of SIOG guidelines for the management of prostate cancer in senior adults. Crit Rev Oncol Hematol. 2010;73:68–91. doi: 10.1016/j.critrevonc.2009.09.005. [DOI] [PubMed] [Google Scholar]
- 14.Mottet N, Bellmunt J, Bolla M, et al. EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol. 2011;59:572–583. doi: 10.1016/j.eururo.2011.01.025. [DOI] [PubMed] [Google Scholar]
- 15.Prostate Cancer Trialists Collaborative Group. Maximum androgen blockade in advanced prostate cancer: An overview of the randomised trials. Lancet. 2000;355:1491–1498. [PubMed] [Google Scholar]
- 16.Small EJ, Halibi S, Dawson NA, et al. Antiandrogen withdrawal alone or in combination with ketoconazole in androgen-independent prostate cancer patients: A phase III trial (CALGB 9583) J Clin Oncol. 2004;22:1025–1033. doi: 10.1200/JCO.2004.06.037. [DOI] [PubMed] [Google Scholar]
- 17.Scher HI, Kelly WK. Flutamide withdrawal syndrome: Its impact on clinical trials in hormone-refractory prostate cancer. J Clin Oncol. 1993;11:1566–1572. doi: 10.1200/JCO.1993.11.8.1566. [DOI] [PubMed] [Google Scholar]
- 18.Small EJ, Srinivas S. The antiandrogen withdrawal syndrome. Experience in a large cohort of unselected patients with advanced prostate cancer. Cancer. 1995;76:1428–1434. doi: 10.1002/1097-0142(19951015)76:8<1428::aid-cncr2820760820>3.0.co;2-t. [DOI] [PubMed] [Google Scholar]
- 19.Figg WD, Sartor O, Cooper MR, et al. Prostate specific antigen decline following the discontinuation of flutamide in patients with stage D2 prostate cancer. Am J Med. 1995;98:412–414. doi: 10.1016/S0002-9343(99)80323-4. [DOI] [PubMed] [Google Scholar]
- 20.Taplin ME, Bubley GJ, Shuster TD, et al. Mutation of the androgen-receptor gene in metastatic androgen-independent prostate cancer. N Engl J Med. 1995;332:1393–1398. doi: 10.1056/NEJM199505253322101. [DOI] [PubMed] [Google Scholar]
- 21.Sartor AO, Tangen CM, Hussain MHA, et al. Antiandrogen withdrawal in castrate-refractory prostate cancer: A Southwest Oncology Group trial (SWOG 9426) Cancer. 2008;11:2393–2400. doi: 10.1002/cncr.23473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Daniell HW. Osteoporosis after orchiectomy for prostate cancer. J Urol. 1997;157:439–444. [PubMed] [Google Scholar]
- 23.Shahinian VB, Kuo YF, Freeman JL, et al. Risk of fracture after androgen deprivation for prostate cancer. N Engl J Med. 2005;352:154–164. doi: 10.1056/NEJMoa041943. [DOI] [PubMed] [Google Scholar]
- 24.Aapro M, Saad F. Bone-modifying agents in the treatment of bone metastases in patients with advanced genitourinary malignancies: A focus on zoledronic acid. Ther Adv Urol. 2012;4:85–101. doi: 10.1177/1756287212441234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: A randomised, double-blind study. Lancet. 2011;377:813–822. doi: 10.1016/S0140-6736(10)62344-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Keating NL, O'Malley AJ, Smith MR. Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J Clin Oncol. 2006;27:4448–4456. doi: 10.1200/JCO.2006.06.2497. [DOI] [PubMed] [Google Scholar]
- 27.D'Amico AV, Denham JW, Crook J, et al. Influence of androgen suppression therapy for prostate cancer on the frequency of timing of fatal myocardial infarctions. J Clin Oncol. 2007;25:2420–2425. doi: 10.1200/JCO.2006.09.3369. [DOI] [PubMed] [Google Scholar]
- 28.Hayes JH, Chen MH, Moran BJ, et al. Androgen-suppression therapy for prostate cancer and the risk of death in men with a history of myocardial infarction or stroke. BJU Int. 2010;106:979–985. doi: 10.1111/j.1464-410X.2010.09273.x. [DOI] [PubMed] [Google Scholar]
- 29.Nguyen PL, Chen MH, Beckman JA, et al. Influence of androgen deprivation therapy on all-cause mortality in men with high-risk prostate cancer and a history of congestive heart failure or myocardial infarction. Int J Radiat Oncol Biol Phys. 2012;82:1411–1416. doi: 10.1016/j.ijrobp.2011.04.067. [DOI] [PubMed] [Google Scholar]
- 30.Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363:411–422. doi: 10.1056/NEJMoa1001294. [DOI] [PubMed] [Google Scholar]
- 31.Longo DL. New therapies for castration-resistant prostate cancer. N Engl J Med. 2010;363:479–481. doi: 10.1056/NEJMe1006300. [DOI] [PubMed] [Google Scholar]
- 32.Huber ML, Haynes L, Parker C, et al. Interdisciplinary critique of sipuleucel-T as immunotherapy in castration-resistant prostate cancer. J Natl Cancer Inst. 2012;104:273–279. doi: 10.1093/jnci/djr514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Fan C, George B, Bross P. CBER clinical review: Sipuleucel-T. [Accessed June 1, 2012]. Available at http://www.fda.gov/downloads/biologicsbloodvaccines/cellulargenetherapyproducts/approvedproducts/ucm214540.pdf.
- 34.Petrylak DP, Tangen CM, Hussain MA, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351:1513–1520. doi: 10.1056/NEJMoa041318. [DOI] [PubMed] [Google Scholar]
- 35.Tannock IF, Osoba D, Stockler MR, et al. Chemotherapy with mitoxantrone plus prednisone or prednisone alone for symptomatic hormone-resistant prostate cancer: A Canadian randomized trial with palliative end-points. J Clin Oncol. 1996;14:1756–1764. doi: 10.1200/JCO.1996.14.6.1756. [DOI] [PubMed] [Google Scholar]
- 36.Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–1512. doi: 10.1056/NEJMoa040720. [DOI] [PubMed] [Google Scholar]
- 37.de Wit R. New hope for patients with metastatic hormone-refractory prostate cancer. Eur Urol. 2006;5:817–823. [Google Scholar]
- 38.Seruga B, Horgan M, Pond GR. Tolerability and efficacy of chemotherapy in older men with metastatic castrate-resistant prostate cancer (mCRPC) in the TAX 327 trial. J Clin Oncol. 2011;29(suppl) doi: 10.1016/j.jgo.2013.12.001. Abstract 4530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Fosså SD, Jacobsen AB, Ginman C, et al. Weekly docetaxel and prednisolone versus prednisolone alone in androgen-independent prostate cancer: A randomised phase II study. Eur Urol. 2007;52:1691–1698. doi: 10.1016/j.eururo.2007.01.104. [DOI] [PubMed] [Google Scholar]
- 40.Galsky MD, Dritselis A, Kirkpatrick P, et al. Cabazitaxel. Nat Rev Drug Discov. 2010;9:677–678. doi: 10.1038/nrd3254. [DOI] [PubMed] [Google Scholar]
- 41.Mita AC, Denis LJ, Rowinsky EK, et al. Phase I and pharmacokinetic study of XRP6258 (RPR 116258A), a novel taxane, administered as a 1-hour infusion every 3 weeks in patients with advanced solid tumors. Clin Cancer Res. 2009;15:723–730. doi: 10.1158/1078-0432.CCR-08-0596. [DOI] [PubMed] [Google Scholar]
- 42.de Bono JS, Outard S, Ozguroglu M, et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet. 2010;376:1147–1154. doi: 10.1016/S0140-6736(10)61389-X. [DOI] [PubMed] [Google Scholar]
- 43.de Bono JS, Logothetis CJ, Molina A, et al. Abiraterone and increased survival in metastatic prostate cancer. N Eng J Med. 2011;364:1995–2005. doi: 10.1056/NEJMoa1014618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Aapro MS, Bohlius J, Cameron DA, et al. 2010 update of EORTC guidelines for the use of granulocyte-colony stimulating factor to reduce the incidence of chemotherapy-induced febrile neutropenia in adult patients with lymphoproliferative disorders and solid tumours. Eur J Cancer. 2011;47:8–32. doi: 10.1016/j.ejca.2010.10.013. [DOI] [PubMed] [Google Scholar]
- 45.Myrup B, Valerius NH, Mortensen PB. Treatment of enteritis in chronic granulomatous disease with granulocyte colony stimulating factor. Gut. 1998;42:127–130. doi: 10.1136/gut.42.1.127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Johnson & Johnson. Study unblinded: ZYTIGA (abiraterone acetate) plus prednisone for asymptomatic or mildly symptomatic chemotherapy-naïve patients with metastatic castration-resistant prostate cancer. [Accessed June 1, 2012]. Available at http://www.jnj.com/connect/news/all/study-unblinded-zytiga-abiraterone-acetate-plus-prednisone-for-asymptomatic-or-mildly-symptomatic-chemotherapy-naive-patients-with-metastatic-castration-resistant-prostate-cancer.
- 47.Azria D, Massard C, Tosi D, et al. An ambispective observational study in the safety and efficacy of abiraterone acetate in the French temporary authorizations for use (ATU): Predictive parameters of response. J Clin Oncol. 2012;30(5 suppl) Abstract 149. [Google Scholar]
- 48.Loriot Y, Massard C, Albiges L, et al. Personalizing treatment in patients with castrate-resistant prostate cancer: A study of predictive factors for secondary endocrine therapies activity. J Clin Oncol. 2012;30(5 suppl) Abstract 213. [Google Scholar]
- 49.Mukherji D, Pezaro CJ, Bianchini D, et al. Response to abiraterone acetate in the postchemotherapy setting in patients with castration-resistant prostate cancer whose disease progresses early on docetaxel. J Clin Oncol. 2012;30(5 suppl) Abstract 17. [Google Scholar]
- 50.de Bono JS, Outard S, Ozguroglu M, et al. A subgroup analysis of the TROPIC trial exploring reason for discontinuation of prior docetaxel and survival outcome of cabazitaxel in metastatic castration-resistant prostate cancer (mCRPC) J Clin Oncol. 2012;29(suppl) Abstract 4526. [Google Scholar]
- 51.Schulman C, Irani J, Aapro M. Improving the management of patients with prostate cancer receiving long-term androgen deprivation therapy. BJU Int. 2012;109:13–21. doi: 10.1111/j.1464-410X.2012.11216.x. [DOI] [PubMed] [Google Scholar]
- 52.Coleman RE. Metastatic bone disease: Clinical features, pathophysiology and treatment strategies. Cancer Treat Rev. 2001;27:165–176. doi: 10.1053/ctrv.2000.0210. [DOI] [PubMed] [Google Scholar]
- 53.Aapro M, Saad F, Costa L. Optimizing clinical benefits of bisphosphonates in cancer patients with bone metastases. The Oncologist. 2010;15:1147–1158. doi: 10.1634/theoncologist.2007-0245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Smith MR, Egerdie B, Toriz NH, et al. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N Engl J Med. 2009;361:745–755. doi: 10.1056/NEJMoa0809003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Chen Y, Clegg NJ, Scher HI. Anti-androgens and androgen-depleting therapies in prostate cancer: New agents for an established target. Lancet Oncol. 2009;10:981–991. doi: 10.1016/S1470-2045(09)70229-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Scher HI, Fizazi K, Saad F, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012 Aug 15; doi: 10.1056/NEJMoa1207506. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 57.Parker C, Heinrich D, O'Sullivan JM, et al. Overall survival benefit of radium-223 chloride (Alpharadin) in the treatment of patients with symptomatic bone metastases in castration- resistant prostate cancer (CRPC): A phase III randomised trial (ALSYMPCA). Presented at the European Multidisciplinary Cancer Congress; September 23–27, 2011; Stockholm, Sweden. [Google Scholar]
- 58.Parker C, Heinrich D, O'Sullivan JM, et al. Overall survival benefit and safety profile of radium-223 chloride, a first-in-class alpha-pharmaceutical: Results from a phase III randomized trial (ALSYMPCA) in patients with castration-resistant prostate cancer (CRPC) with bone metastases. J Clin Oncol. 2012;30(5 suppl) Abstract 8. [Google Scholar]