
Figure 7.
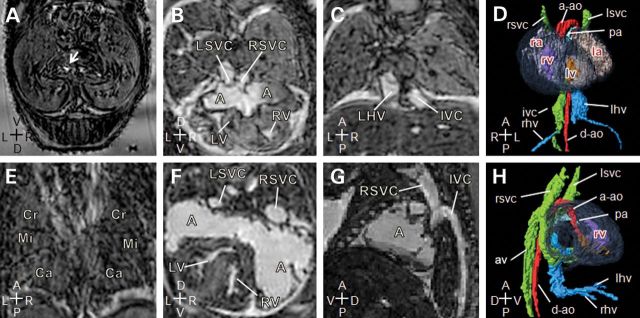
Laterality and complex cardiovascular abnormalities in Zic3flox/y; T-cre embryos. Magnetic resonance imaging of 15.5 dpc mutant embryos. (A and E) Transverse and coronal sections of a Zic3flox/y; T-cre embryo showing a midline stomach (arrow) and right pulmonary isomerism. (B–D) Transverse, coronal sections and three-dimensional reconstruction (ventral view) of a Zic3flox/y; T-cre embryo showing a large atrial septal defect, resulting in a common atrium (A), into which drains the left and right superior vena cava (LSVC, RSVC). The heart is malpositioned to the right (dextrocardia). Inferior vena cava (IVC) is continuous on the right and receives the right hepatic veins (rhv) prior to entering the atrium, while the left hepatic veins (LHV) enter separately. (F–H) Transverse, sagittal sections and three-dimensional reconstruction (right view) of a Zic3flox/y; T-cre embryo showing a normal positioned heart with a dilated common atrium (A), into which drains the left and right superior vena cava (LSVC, RSVC). Inferior vena cava (IVC) is interrupted and drains via the azygous vein (AV) to the right superior vena cava (RSVC). The hepatic veins come together and enter the atria without joining the IVC. Axis: D, dorsal; V, ventral; R, right; L, left; A, anterior; P, posterior.