

Abstract
Objectives
The purpose of this study was to explore the effects of Erzhi Tiangui Granule (ETG) on DNA methyltransferases (DNMT) 1 protein expression in endometrium of infertile women with Kidney-yin Deficiency syndrome.
Methods
A randomized, double-blinded, placebo-controlled clinical trial was conducted. Sixty-six (66) infertile patients who had Kidney-yin Deficiency syndrome and who were to undergo in vitro fertilization–embryo transfer (IVF-ET) were randomly assigned to either a treatment group or a control group according to a random table. Besides gonadotropin (Gn) therapy in both groups, the treatment group received ETG for 3 menstrual cycles before IVF, and the control group received placebo granules. The ETG and the placebo granules were made with similar color and shape, as well as in the same packaging. The scores of the Kidney-yin Deficiency syndrome were assessed. Other outcome measures included the dosage and duration of Gn, the number of retrieved oocytes, the rate of high-quality oocytes, the rate of high-quality embryos, the fertilization rate, and the clinical pregnancy rate. DNMT1 protein expression in the endometrium was measured in the midluteal phase.
Results
The difference in the syndrome score change before and after treatment between the two groups was statistically significant (p<0.05). The dosage and duration of Gn were significantly lower in the treatment group than those in the control group (p<0.05). The high-quality oocyte and embryo rates, and clinical pregnancy rate were all higher in the treatment group than those in the control group (p<0.05). The fertilization rate was not significant when compared to the placebo group. No difference was found in the number of retrieved oocytes between the two groups. The DNMT1 protein expression in the endometrium was much more abundant in the treatment group than that in the control group (p<0.05).
Conclusions
For the infertile patients undergoing IVF, the Chinese recipe for tonifying the Kidney as an adjunct treatment could reduce Gn dosage and treatment duration, alleviate clinical symptoms, and improve the clinical pregnancy rate. The increased level of DNMT1 protein expression after treatment may lead to enhanced endometrial receptivity. This finding may explain the improvement in clinical pregnancy rate.
Introduction
Infertility is a global issue for childbearing couples who are unable to conceive. The success of assisted reproductive technology (ART) procedures, although offering a treatment option and bringing new hope to the patients, may be restrained by poor endometrial receptivity among other challenges. It has become an important aspect of fertility research to improve endometrial receptivity and to synchronize the development of both the endometrium and the embryo. Endometrial receptivity to embryo probably depends on the concerted action of a number of gene products. The transcription regulation of these genes, either constitutive or cyclic, may be in part epigenetically controlled through DNA methylation, with a higher degree of methylation associated with a lower level of gene expression. DNA methyltransferases (DNMTs) are the key enzymes to establish and maintain DNA methylation. Among them, DNMT1 is the most abundant methytransferase in the somatic cells, and its level reflects the status of the genetic methylation.1
Erzhi Tiangui Granule (ETG), with the function of tonifying the Kidney, nourishing blood, and regulating the Chong-Ren meridian, has been applied clinically for more than 20 years and demonstrated favorable effects on female infertility. Previous studies showed that ETG could improve the quality of oocytes and promote embryo development.2,3 This study further investigated the effect of ETG on outcomes of in vitro fertilization (IVF) in infertile women and explored its mechanism by observing the DNMT1 expression in the endometrium during the implantation period.
Materials and Methods
This was a randomized, placebo-controlled study. The study was approved by the health authorities and ethics committees.
Diagnosis standard
Western medicine diagnosis standard
Infertility4 is defined as failure of a couple of reproductive age to conceive after 2 years or more with regular coitus and without using contraception.
Infertility is considered primary when it occurs in a woman who has never established a pregnancy and secondary when it occurs in a woman who has a history of one or more previous pregnancies.
Tubal obstruction is defined as an obstructed oviduct or hydrosalpinx confirmed by hystero-salpingography, or an obstructed oviduct and adhesion inside the pelvic cavity confirmed by hydrotubation through laparoscopy. 5
Diagnosis standard in Traditional Chinese Medicine.6,7
Diagnosis criteria for infertility with Kidney-yin Deficiency syndrome type are ≥2 of primary symptoms of infertility, sore lower back and knees, dry vagina, dysphoria with feverish sensation in the chest, palms, and soles; and ≥1 of secondary symptoms of early or delayed menstrual cycle, oligomenorrhea or amenorrhea, dizziness and tinnitus, tidal fever with red cheek, dry mouth and throat, emaciation, insomnia and amnesia; and with reference to the typical tongue and pulse manifestations, including red tongue with little coating and thin and rapid pulse.
Symptom scoring standard in Traditional Chinese Medicine
Each symptom is graded on a scale of I–IV based on the severity and frequency of the symptoms, with grade I indicating continuously symptomatic and affect daily life, grade II frequently symptomatic, grade III occasionally symptomatic, and grade IV no symptoms. For the primary symptoms, scores 6, 4, 2, and 0 corresponding to grades I–IV, respectively, were used; and for the secondary symptoms, scores 3, 2, 1, and 0 were used.
Inclusion criteria
The inclusion criteria were as follows: Married women between 25 and 40 years of age; diagnosed as having infertility with tubal obstruction, and Kidney-yin Deficiency syndrome; hormonal test within the normal range; and no infertile factors in their male partners.
Exclusion criteria
Exclusion criteria were as follows: Patients (1) received hormonal therapy in the preceding 3 months; (2) were inappropriate to become pregnant due to clinically significant illnesses; (3) had severe mental or psychiatric diseases, acute infection in the urogenital system, or sexually transmitted disease; (4) were diagnosed with hereditary diseases that were inappropriate to give birth per the Maternal and Child Health Law of PRC; (5) had drug abuse or harmful addiction; or (6) were exposed to radiation, toxin, or drugs that could cause fetal malformation.
The patients participating in this trial had to withdraw all the other Chinese herbal decoctions and Chinese patent medicines. Patient compliance was monitored based on the pill counts at each study visit.
Patient enrollment and grouping
All of the 66 infertile patients were recruited from the Integrative Medicine Research Centre of Reproduction and Heredity, the Affiliated Hospital of Shandong University of Traditional Chinese Medicine from June 2009 to October 2010. All participants gave written consent prior to entering the trial.
A random table was provided by Prof. Shi Zhou-hua from Shandong University of Traditional Chinese Medicine. A nurse was in charge of registration and assignment. The 66 patients were paired according to their age, disease course, and medical history and assigned randomly based on a random number table to the treatment or the control group in a 1:1 ratio.
Study protocol
The clinical trial was conducted with the approval of the ethics committees of the relevant hospital and in strict accordance with the principles stipulated in Declaration of Helsinki and Guidelines for Good Clinical Practice.
Drug composition and treatment regimen
The ETG was prepared with Fructus Ligustri Lucidi 15 g, Eclipta alba (overground part) 15 g, Fructus Lycii 15 g, Semen Cuscutae 15 g, Angelica sinensis 12 g, Radix Paeoniae alba 12 g, Radix Ligusticum wallichii 9 g, Radix rehmanniae praeparata 12 g, prepared Rhizoma cyperi 12 g, and Radix glycyrrhizae preparata 6 g by the Drug Manufacturing Unit of the Affiliated Hospital of Shandong University of Traditional Chinese Medicine. The raw herbs were mixed first, then boiled with water. The liquid extract was made into granules by spray-drying process. The ETG was packaged as 3 g/bag, batch number 01-FZ032-03. The placebo granule, composed mainly of dextrin, was prepared by the same institution in a color and shape similar to the ETG. The placebo granules were packaged as 3 g/bag, with the same package of the ETG, batch number [01] FZ032-03-1. The heavy metal and contaminant testing of the herbs showed negative results.
The treatment began three menstrual cycles prior to the scheduled IVF. ETG or placebo was given orally after being dissolved into water, 6 g each time, 3 times a day, from the 3rd day of each menstruation for 14 days in each cycle for a total of 3 menstrual periods.
Controlled ovarian hyperstimulation (COH) and in vitro fertilization
All subjects received controlled ovarian hyperstimulation following a long protocol (gonadotropin-releasing hormone /FSH-r/human menopausal gonadotropin/human chorionic gonadotropin [HCG] proposal).
On approximately 21 days of the last menstrual cycle prior to the IVF procedure (in the luteal phase), all subjects received a single dose of HCG, 10,000 IU (5000 IU per ampoule, Livzon Pharmaceutical Group Inc., Zhuhai, China, batch number 090515B) after the vaginal ultrasound confirmation of ≥3 follicles with size ≥18 mm, endometrium thickness 8–10 mm, and cervical mucus wire drawing ≥10 cm. Treatment with ETG or placebo was to discontinue on the day of HCG injection. Thirty-six (36) hours after HCG injection, oocyte retrieval (OR) was conducted under transvaginal ultrasound. IVF was performed and fertilized embryos were cultured in vitro for 3 days. Two to three high-quality embryos were selected and transferred on Day 3 after OR. Luteal phase support was provided after embryo transfer with progesterone for up to 14 days when urine or serum HCG was tested positive, defined as biochemical pregnancy, or until confirmation of clinical pregnancy, which was defined by at least one intrauterine gestational sac with fetal heartbeat documented by transvaginal ultrasound 5 weeks after embryo transfer.
The unblinding process was performed by Prof. Shi Zhou-hua from Shandong University of Traditional Chinese Medicine.
Study outcome measures
Syndrome scoring
According to the scoring standard of Chinese syndrome of Kidney-yin Deficiency, the symptoms were scored and recorded on the recruitment day (pretreatment) and the OR day (post-treatment) to evaluate the effect of treatment on the syndrome.8
Gn dosage and duration are recorded by designated personnel.
Oocyte morphology grading standard
Maturity of oocytes was classified on a scale of I–IV, with higher scores indicating more maturity, based on the morphological features, including oocyte–corona–cumulus complex, under the microscope.9
High-quality oocyte rate (%)=number of grade III oocytes/total oocyte number ×100%;
Fertilization rate (%)=oosperm number/total oocyte number×100%;
Cleavage rate (%)=blastomere number/oosperm number×100%.
Embryo quality was classified on a scale of 1–5 as described by Puissant et al.,10 and a high-quality embryo is defined as an embryo with a score ≥3.
High-quality embryo rate (%)=high-quality embryo number/oosperm number×100%.
Endometrial biopsies samples collected through a minimally invasive procedure were fixed with neutral formalin and preserved at −4°C. Expression of DNMT1 protein in endometrium was determined with a mouse anti-human monoclonal DNMT1 antibody (Abcam Co., Britain) using immunohistochemistry. The immunohistochemical analysis was performed according to the test kit instruction. The semiquantitative analysis on immunohistochemical images was carried out using a 4-point scale of 0–3 to quantify (1) staining intensity, with 0 indicating no color, 1 light brownish yellow, 3 dark brown, and 2 in between; and to quantify (2) proportion of positive cells, with 0 indicating ≤5%, 1 indicating 6%–20%, 2 indicating 21%–50%, and 3 indicating >50% positive cells. The final H-score=(1)+(2) was used to determine the expression of DNMT1 expression by immunohistochemistry.11
Adverse reactions and safety outcome measures
Patients were observed and queried for adverse reactions during the treatment period. Clinical laboratory tests (routine urine, blood, and stool tests) and electrocardiograms were performed on the day of study enrollment (pretreatment) and after embryo transfer.
Statistical analysis
Statistical analysis was performed using SPSS 16.0 for Windows (Chicago, IL). Paired t-test was used to compare the mean value of measurement data between pretreatment (baseline) and post-treatment in the same group; one-way analysis of variance was used for comparing those between groups. Categorical data were analyzed with the χ2 criterion.
Results
Patient information
No significant differences were found in age, disease duration, and medical history between the two groups (Table 1).
Table 1.
Patient Information in the Two Groups
| |
|
Age (year) |
|
Medical history (case) |
|||
|---|---|---|---|---|---|---|---|
| Group | Case | 25– | 30– | 35–40 | Disease course (year) | Primary infertility | Secondary infertility |
| Treatment | 33 | 3 | 9 | 21 | 5.73±3.27 | 9 | 24 |
| Control | 33 | 2 | 10 | 21 | 5.58±2.87 | 12 | 21 |
Comparison of the Kidney-yin Deficiency syndrome scores between groups
All 66 patients completed the study without major protocol violations, and all were included in the outcome analyses.
Comparing the pretreatment to the post-treatment scores, the Kidney-yin Deficiency syndrome score was significantly lower in the treatment group (p>0.05), while that in the control group showed no significant different. The difference in the syndrome score change from the pretreatment between the treatment and placebo groups was significant (p>0.05, Table 2).
Table 2.
Comparison of the Symptom Scores Between Groups
| Group | Case | Time | Symptom score | Change from pretreatment |
|---|---|---|---|---|
| Treatment | 33 | Pretreatment | 16.73±2.31 | −7.58±1.97** |
| Post-treatment | 9.15±1.44* | |||
| Control | 33 | Pretreatment | 17.24±2.05 | −0.39±1.12 |
| Post-treatment | 16.42±1.92 |
Compared with pretreatment in the same group.
*p>0.05; compared with the control group, **p>0.05.
Comparison of Gn dosage and duration between groups
Gn dosage was lower and duration was shorter in the treatment group than in the control group, and the differences were significant (both p<0.05, Table 3).
Table 3.
Comparison of Gn Dosage and Duration, High-Quality Oocyte Rate, High-Quality Embryo Rate, Oocyte Retrieval, and Fertilization Rate Between Groups
| Group | Case | Gn (ampoule) | r-FSH (day) | Oocyte number per patient | High-quality oocyte rate (%) | Fertilization rate (%) | High-quality embryo rate (%) |
|---|---|---|---|---|---|---|---|
| Treatment | 33 | 28.21±6.28* | 10.82±2.09* | 10.79±6.17 | 85.11* | 76.68 | 77.29* |
| Control | 33 | 31.91±6.21 | 11.97±1.79 | 11.15±5.43 | 78.80 | 70.34 | 69.11 |
Compared with the control group, *p>0.05.
r-FSH, recombinant-follicle-stimulating hormone.
Comparison of high-quality oocyte rate, high-quality embryo rate, oocyte retrieval, and fertilization rate between groups
Both the high-quality oocyte rate and high-quality embryo rate were higher in the ETG treatment group than the control group, as demonstrated in Table 3. The average number of retrieved oocytes per patient was similar between the two groups. The fertilization rate was higher in the ETG treatment group but the difference was not statistically significant (p>0.05). The biochemical pregnancy rate and clinical pregnancy rate were both 54.55% (18/33) in the treatment group, higher than the control group (36.36% [12/33] and 30.30% [10/33], respectively; χ2=3.970, p<0.05).
Comparison of endometrial DNMT1 expression between groups
Histological examination of endometrium showed a typical decidual endometrium in the treatment group with synchronous growth of stroma and glands and normal secretion in glandular epithelium. This was in contrast to the endometrium in the control group, which showed asynchronous growth of stroma and glands, and reduced gland secretion (Fig. 1).
FIG. 1.
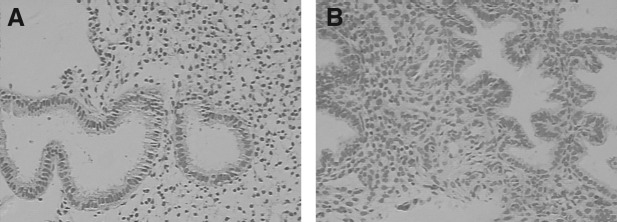
Morphological observation of endometrium (HE staining,×100). A: The control group shows asynchronous growth of stromal and glandular tissues, and decreased secretion in glandular epithelium. B: The treatment group shows decidual endometrium, synchronous growth of stromal and glandular tissues, and normal secretion in glandular epithelium.
Comparing the pregnant women from the ETG treated or control groups, endometrial DNMT1 expression demonstrated increased expression in the treated group compared with the control group, as shown in Figure 2. Statistically, the H-score of the immunohistochemical image for endometrial DNMT1 expression in the treatment group (3.31±0.46, n=33) was significantly higher than that in the control group (2.97±0.49, n=33, p>0.05).
FIG. 2.

DNA methyltransferase 1 (DMNT1) expression in the endometrium (DAB staining). A. Sample from pregnant woman from control group (×100). B. Sample from pregnant woman from control group (×200). C. Sample from pregnant woman treated with Erzhi Tiangui granule (ETG) (×100). D. Sample from pregnant woman treated with ETG (×200). The DMNT1 expression is found in the nuclei of the stromal cells and the glandular cells, and is more abundant in the treatment group than in the control group.
Comparison of endometrial DNMT1 expression between pregnant and nonpregnant cases
DNMT1 protein expressions in the endometrium of pregnant cases were significantly higher than that of nonpregnant cases, as demonstrated in Table 4.
Table 4.
Comparison of Endometrial DNA Methyltransferases 1 Expression Between Pregnant and Nonpregnant Cases (Score)
| Group | Case | H-score | t | p |
|---|---|---|---|---|
| Pregnant case | 28 | 3.34±0.54 | 2.489 | 0.015 |
| Nonpregnant case | 38 | 3.03±0.47 |
Adverse reactions
No obvious adverse reactions were found in either group during the entire study duration. No clinically significantly changes from pretreatment were found in routine tests of blood, urine, and stool, and in electrocardiogram after treatment in either group.
Discussion
Implantation is a complicated process involving concerted action of extracellular hormonal changes, interaction between embryo and endometrium, and endometrial cellular remodeling. Endometrial receptivity to embryos may depend on constitutive and cyclic expressions of certain genes.12 DNA methylation plays an important role in migration and invasiveness of chorionic villus cells.13 Yashiaki1 reported that DNMT1, DNMT3a, and DNMT3b were expressed in the nuclei of endometrial epithelial cells and stromal cells during menses, and their expression was downregulated in the secretory phase of the cycle and after Provera (medroxyprogesterone acetate) administration, indicating that DNMTs may have regulatory effects on genes associated with shedding of endometrium in the menstrual cycles.
Implantation dysfunction is an important factor affecting the success ratio of ART. There have been studies on implantation-related gene imprinting and methylation. However, few studies reported endometrial DNMT1 expression during the implantation period in infertile patients. Hu et al.14 reported that in 25 healthy women, monoallelic expression of H19 was found in endometrium during the window phase, while in 38 cases of unexplained infertility, all were di-allelic expression, suggesting that loss of gene printing may correlate with the occurrence of unexplained infertility.
Ovarian hyperstimulation may lead to abnormal expressions of two imprinted genes, Snrpn and H19, in the placenta, and it was inferred that imprinted genes were easily interfered with by extraneous factors.15 Doherty et al.16 also confirmed that loss of imprinting was possibly due to weakened activity of Dnmt1 and reduction of methylation in the upstream imprinting control region.
Presently, the regulation mechanism of DNMT expression is not clear. A study from Yoshiaki showed that the expression of DNMT3a and DNMT3b was downregulated upon treatment with female sex hormone, indicating that DNA methylation might be regulated by sex hormones.1 Chinese medicines for tonifying the Kidney and producing blood (e.g., Radix rehmanniae, Fructus Corni, tortoise-plastron glue, colla corii asini, Lycium barbarum L, etc.) were shown to increase the activity and thermostability of DNA methylase as well as its tolerability to NaCl in the brain of senile rats.17 Ginseng decoction was shown to improve DNA methylase activity in a mouse model of Kidney-Deficiency and have an effect on postponing aging.18
According to Traditional Chinese Medicine theory, the Kidney is the organ for storing essence and controls reproduction. Essence and blood share the same origin and are interchangeable. Sufficient Kidney essence provides adequate blood to nourish the uterus and creates an appropriate environment for implantation. Kidney-Deficiency may lead to a malnourished uterus incapable of supporting implantation. It was reported that Chinese medicines for tonifying the Kidney could increase uterus weight by increasing thickness of the endometrial layer and abundance of endometrial glands, and these changes were associated with the upregulated expression of receptors for estrogen and progesterone.19 Furthermore, the medicines were shown to promote blood circulation of reproductive organs.20 In clinical practice, it was also found that most of the infertile patients belonged to the Kidney-yin Deficiency syndrome type, and treatment with ETG was often prescribed and shown to have clinical benefits. Such practice was consistent with the rationale that ETG has a function of tonifying the Kidney, nourishing blood, and regulating the Chong-Ren meridian. Many pharmacological studies showed that one of the active ingredients of Fructus Ligustri Lucidi, oleanolic acid, could increase levels of estradiol, superoxide dismutase, and glutathione peroxidase, decrease MDA level, and improve the morphology and function of the ovary and adrenal gland in climacteric rats.21 Total flavonoids from Eclipta alba could significantly eliminate reactive oxygen, showing an obvious restrictive action on lipid peroxidation of lecithin and DNA oxidative damage.22 The flavonoids from Semen Cuscutae could increase the weight of the adenohypophysis, ovary, and uterus in adult rats, and weight of testicle and appendix testis in male mice, elevate the functions of gonadotropin/luteinizing hormone receptor and the reactivity of hypophysis to gonadotropin-releasing hormone, and improve secretion of villus in vivo. Its water extract may improve vagina epithelial cell cornification.23 Fructus Lycii has antioxidant, anti-aging, and anti-fatigue functions, which were reported to have good effects on female infertility.24
Our previous experimental and clinical studies revealed that the ETG granule could raise the quality of oocytes, and promote differentiation and development of oosperm and early embryo, indicating that the treatment may have an effect on reproductive endocrine function and endometrial receptivity in addition to the overall effect on tonifying the Kidney.25,26
The imprinted genes in endometrium of infertile women lose the imprinting during the implantation period. The methylation of DNA is one of the most important patterns of the gene imprinting. However, the regulation of DNMTs expression is poorly understood. The current study extended the findings from the previous studies and demonstrated that the adjunct treatment with ETG in IVF resulted in clinically significant benefits, including an increase in the quality of retrieved oocytes, a higher fertilization rate, and ultimately a higher clinical pregnancy rate. The study also demonstrated an increased expression of DNMT1 in the endometrium after ETG treatment. It is further hypothesized that the change in DNMT1 expression may alter endometrial gene expression pattern, which in turn may contribute to the improvement in endometrial receptivity and subsequent success in embryo implantation. Further research on the regulation of DNMT1 expression by ETG and the relationship between DNMT1 and endometrial receptivity is needed.
Conclusions
For the infertile patients undergoing IVF, the Chinese recipe for tonifying the Kidney as an adjunct treatment could reduce Gn dosage and treatment duration, alleviate clinical symptoms, and improve the clinical pregnancy rate. The increased level of DNMT1 protein expression after treatment may lead to the enhanced endometrial receptivity and improved embryo implantation. This finding, together with the observed higher percentages of high quality of oocytes and embryos after treatment, may explain the improvement in clinical pregnancy rate.
Acknowledgments
We wish to thank Dr. Guo Yan from China Academy of Chinese Medical Sciences for translating and revising the manuscript, and Yuewen Zhao from Queen's University in Canada for assisting revising. We are also indebted to all the other staff members for their efforts: Meng Qian, Sun Jin-long from Affiliated Hospital of Shandong T.C.M. University; Wu Hai-cui from Shandong University of Traditional Chinese medicine.
This work was supported by National Natural Science Fund project No. 30672706, Natural Science Fund project of the Department of Science and Technology in Shandong province No. ZR58, Doctor Subject Foundation of the Ministry of Education of China under Grant No. 20093731110006.
Disclosure Statement
No competing financial interests exist.
References
- 1.Yamagata Y. Asada H. Tamura I, et al. DNA methyltransferase expression in the human endometrium : Downregulation by progesterone and estrogen. Hum Reprod. 2009;24:1126–1132. doi: 10.1093/humrep/dep015. [DOI] [PubMed] [Google Scholar]
- 2.Fang L. Zhengao S. Lin M, et al. Experimental study on effect of Erzhi Tiangui Granule in improving quality of oocyte and its correlation with level of insulin-like growth factor-1R mRNA expression in ovary of mice. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2006;26:431–434. [PubMed] [Google Scholar]
- 3.Jianwei Z. Fang L. Zhengao S, et al. The influence of Erzhi Tiangui granule on the IL-1β and IL-6 of the follicle fluid and the quality of embryos during the controlled ovarian hyperstimulation. Reprod Contracep. 2007;27:714–717. [Google Scholar]
- 4.Feng Y. Shen K. Obstetrics and Gynecology. Beijing: People's Medical Publishing House; 2001. 394 pp. [Google Scholar]
- 5.Institute of Obstetrics Gynecology of Chinese Association of the Integration of Traditional Western Medicine of the Third Conference. Endometriosis, pregnancy-induced hypertension and treatment of female infertility in the Western Standard. Zhongguo Zhong Xi Yi Jie He Za Zhi. 1991;11:376–378. [Google Scholar]
- 6.Zhang Y. Chinese Gynecology. 1st ed. Beijing: China Press of Traditional Chinese Medicine; 2002. pp. 323–324. [Google Scholar]
- 7.National Bureau of Technical Supervision. National Standard of China. Chinese Term Syndrome Part of Clinical Practice. Beijing: China Standard Press; 1997. [Google Scholar]
- 8.Ma B. Chinese Gynecology. Shanghai: Shanghai Science and Technology Press; 1998. pp. 206–210. [Google Scholar]
- 9.Lu H. Lu G. Human Reproduction and Reproductive Engineering. Zhengzhou: Henan Science and Technology Press; 2001. pp. 109–110. [Google Scholar]
- 10.Puissant F. Van Rysselberge F. Barlow P, et al. Embryo scoring as a prognostic tool in IVF treatment. Hum Reprod. 1987;2:705–708. doi: 10.1093/oxfordjournals.humrep.a136618. [DOI] [PubMed] [Google Scholar]
- 11.Sant'Ana de Almeida EC. Nogueira AA, et al. Immunohistochemical expression of estrogen and progesterone receptors in endometrial polyps and adjacent endometrium in postmenopausal women. Maturitas. 2004;49:229–233. doi: 10.1016/j.maturitas.2004.02.009. [DOI] [PubMed] [Google Scholar]
- 12.Bischof P. Meissue A. Campana A. Mechanisms of endometrial control of trophoblast invasion. J Reprod Fertil Suppl. 2000;55:65–71. [PubMed] [Google Scholar]
- 13.Rahnama F. Shafiei F. Gluckman PD, et al. Epigenetic regulation of human trophoblastic cell migration and invasion. Endocrinology. 2006;147:5275–5283. doi: 10.1210/en.2006-0288. [DOI] [PubMed] [Google Scholar]
- 14.Hu C. Li L. Han L, et al. Abnormal expression of imprinting gene H19 in endometrium in women with unexplained infertility. Basic Med Sci Clin. 2003;23:503–506. [Google Scholar]
- 15.Fortier AL. Lopes FL. Darricarrère N, et al. Superovulation alters the expression of imprinted genes in the midgestation mouse placenta. Hum Mol Genet. 2008;17:1653–1665. doi: 10.1093/hmg/ddn055. [DOI] [PubMed] [Google Scholar]
- 16.Doherty AS. Mann MR. Tremblay KD. Differential effects of culture on imprinted H19 expression in the preimplantation mouse embryo. Biol Reprod. 2000;62:1526–1535. doi: 10.1095/biolreprod62.6.1526. [DOI] [PubMed] [Google Scholar]
- 17.Bai JS. He ZX. Wu ZK, et al. Effect of anti-aging drug on DNA methylase of brain in rats. Zhongguo Zhong Xi Yi Jie He Za Zhi. 1996;16:358–359. [PubMed] [Google Scholar]
- 18.Lin Y. Chen B. Chen Y. Effect of ginseng to DNA methylating enzyme vitality in mouse liver. J Fujian Coll Trad Chin Med. 1998;9:12–14. [Google Scholar]
- 19.Liu YJ. Huang GY. Yang MW, et al. Effects of Jiantai liquid on the expression of estrogen/progesterone receptors in embryo implantation dysfunction mice endometrium. Zhongguo Zhong Yao Za Zhi. 2005;30:373–376. [PubMed] [Google Scholar]
- 20.Zhang SC. Shen MX. Cai LX, et al. The Kidney nourishing herbs regulate menstruation and ovulation in rats. J Trad Chin Med. 1999;40:369–371. [Google Scholar]
- 21.Lou Y. Chen Z. Wang CX. Experimental study of oleanolic acid liquid acting on climacteric rats. J Chin Med Mater. 2005;28:584–587. [PubMed] [Google Scholar]
- 22.Wang X. Zhang J. Dai Y. Gao Y. Study on extraction of flavone from Eclipta alba and its antioxidation in vitro. Lishizhen Med Mater Med Res (Chin) 2009;20:356–358. [Google Scholar]
- 23.Qin D. She B. She Y. Effects of flavonoids of Semen Cuscutae on reproductive function of animals. Trad Chin Drug Res Clin Pharmacol (Chin) 2000;11:349–351. [Google Scholar]
- 24.Shi RC. Barbary Wolfberry Fruit. 1st. Hangzhou: Zhejiang Science Technology Press; 2002. pp. 12–22. [Google Scholar]
- 25.Lian F. Zhang J. Zhang N, et al. Integrated traditional and Western medicine therapy in vitro fertilization application. J Shandong Univ Trad Chin Med. 2002;26:182–183. [Google Scholar]
- 26.Lian F. Sun Z. Zhang J, et al. Experimental study on effect of Erzhi Tiangui recipe on quality of oocyte in mice. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2004;24:625–627. [PubMed] [Google Scholar]