

Abstract
Background:
Prevention from caries is a principle in dentistry and fissure sealant therapy is being used as a preventive method success of sealants is directly depending on their retention.
Aim:
The Aim of the present study is to evaluate effects of enamel preparation on sealant retention.
Settings and Design:
Clinical trial.
Materials and Methods:
About 57 children aged 6-8 year old took part in this study. 200 first molar teeth of these children has been randomly separated into two groups: A case group (Mechanically preparation of enamel) and a control group (conventional method, without preparation). After applying fissure sealants children were followed up 6 months later.
Statistical Analysis Used:
Mann- U- Whitney Test was used.
Results:
Complete retention after 6 month follow up was 86.7% in case group and 82.8% in control group. No significant difference was seen between the groups after 6 month follow up. (P = 0.508).
Conclusion:
Although statistical evaluation didn't show significant difference, but sealant retention was more after preparation technique.
Keywords: Fissure sealant, mechanical preparation, retention
Introduction
In dentistry, the aim is to prevent dental caries instead of cutting the teeth. It is impossible to clean deep and thin fissures with hygienic tools such as toothbrush. These pits and fissures are prone to decay and include more than 85% of decayed dental surfaces. One effective treatment to prevent occlusal cavities is the use of fissure sealant therapy. Unfortunately, it has been reported that sealant retention after a year is 85% and after 5 years is about 50%. For increasing the effect of sealants, various preparation methods has been suggested: Using Pumice to clean tooth,[1] polish system through the air,[2] to thrust sodium bi-carbonate through spraying water on dental surfaces using air-abrasive technique, shaping tooth enamel with laser and etching the enamel with phosphoric acid.[3,4] Also, it has been reported that cleaning the enamel before etching and bonding can increase the sealant retention.[5] Some studies indicated that using air-abrasion without using additional acid etching is not able to show acceptable bond strength.[4] Whereas other research suggests that abrasive technique can be as a substitute for enamel acid etching.[6] About invasive technique that pits and fissures are opened with bur and they are deepened and widened with it, it is said that this condition can cause to increase the sealant penetration to deeper fissure areas and to extend the surfaces.[7] Other study indicated that acid etching in its conventional form has apparently lower micro leakage than the method in which fissures are cleaned and roughed and then etched. Etching with phosphoric acid increases the amount of retention in fissure sealants containing resins. Although mechanical preparation of tooth causes loss of dental structure, it can also increase the retention.[8] Because of current differences related to using of substitute methods to prepare fissures, this controlled study is achieved with aim to evaluate fissure sealant retention after preparing the enamel with the common method (etching) and invasive method in children of 6 to 8 year old in pediatric department, Islamic Azad dental university.
Materials and Methods
In this experimental in vivo research, 57 children 6-8 years old that had erupted one or two pairs of first permanent molars and required fissure sealant therapy were selected. The samples didn't have any restoration, fracture, crack and sealant on fissures and identifiable decay wasn't observed in them. They have acceptable hygiene. In every child, one or two teeth were put in case group and opposite tooth in control group. Teeth were randomly classified into two group based on enamel preparation: 1. Without preparation 2. Enamel preparation with fissurotomy burs (18013, STF, S.SW), with forward and backward motion to open central fissures.[9] All teeth were isolated with cotton rolls and etched with phosphoric acid Gel 37% (3M-ESPE)[9,10] in 20 seconds[10] with current applicator in the Kit. After washing with water in 30 seconds[10,12] and replacing cotton rolls, it was dried with air without oil in 15 seconds.[10] After observing chalky appearance, the sealant material (3M-ESPE 2007 made in U.S.A) was put on the fissures according to the instructions. Light beam was put with a light-cure device (Coltolu × 2.5 Model No.C7306 USA) with output power 400 mw per cm2 in 40 seconds[9,10,12] on them. After polymerization, the sealant retention was checked with a probe. Finally, occlusion was checked and adjusted by a finishing flame shape diamond bur (SS White CFT) with cooling spray.[10] The cases were clinically evaluated after 6 months through observation by mirror and probe to check the retention. The degree of retention was classified as following: 1. sealant was completely retained. 2. Sealant was partially lost. 3. Sealant was completely lost. The amount of retention was assessed by a blind pedodontist. The results were evaluated statistically via Mann-u-Whitney test. The success and failure of fissure sealant in both groups was assessed with statistical Chi-square test and defined as following: Success = after 6 months, the sealants are completely retained. Failure = after 6 months, sealants is lost (whether complete, or partial).
Results
In this study, 57 children 6-8 years old were put under fissure sealant therapy with two preparation methods. In the 6 months recall, of 200 teeth that were received fissure sealant therapy 177 samples were assessed [Table 1]. This study evaluated the effectiveness of preparing enamel on retention of fissure sealants and that was assessed with grading [Figure 1]. Based on surveys with Mann-U-Whitney test, there was no significant difference between two groups when samples were followed according to success rate:success or failure [Table 2].
Table 1.
Evaluation of retention after 6 months
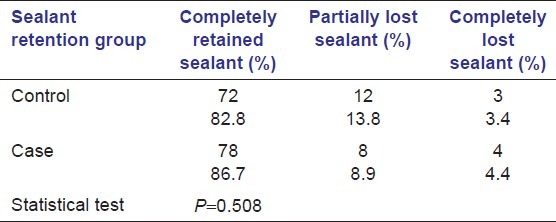
Figure 1.
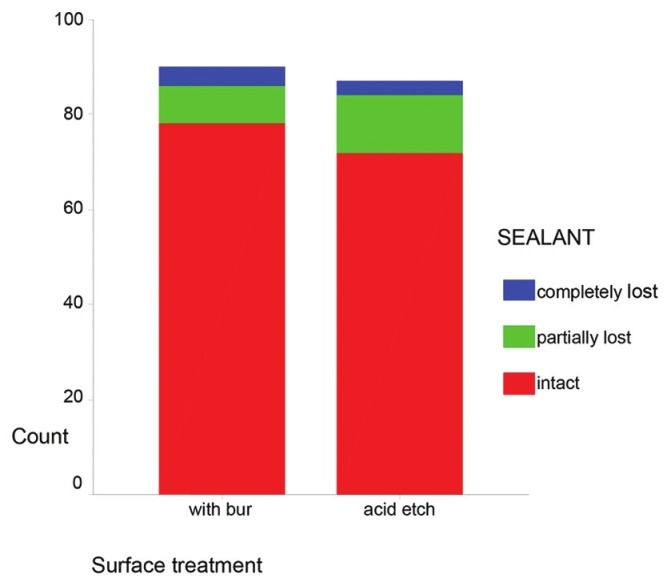
Evaluation of diffusion of redundancy of 177 specimens according to the retention grades after 6 month
Table 2.
Evaluation of the specimens according to the success rate

Discussion and Conclusion
The present study indicated that the enamel preparation with bur increases the amount of fissure sealant retention but statistically it wasn't significant compared with conventional method. In 6 months recall of 200 teeth that were received fissure sealant therapy, 177 samples were assessed. In control group, 82.8% and in Case group 86.7% of sealants were completely retained. Also, in Case group 8.9% and in control group 13.8% of the sealants were incompletely lost and in Case group 4.4% and in control group 3.4% were completely lost. The sealant retention depends on the method of preparing fissures. So, they were mechanically prepared and compared with those without preparation. The mechanical preparation widens the fissures that cause fissure sealant to penetrate more inside the fissures. Also, it removes debris and increase enamel surface energy that all cause to reduce micro-leakage.[9] Although, there are the various methods fore preparing enamel, there isn't any agreement about preference of one to another. Various burs such as ½, ¼ round and diamond komet No.8392 and …are used for preparation.[5,8,13,14]
In this study, fissurotomy bur (18013, STF, S.S.W) was used that this can be the cause of difference between this study and the study that is achieved by M.N.Youseff et al. The aim of that study was to assess the effect of enamel preparation method on micro-leakage of the flow able composite as fissure sealants and was done in-vitro. To prepare the enamel, the diamond bur No.1191 F (K.G Sorensen, 13 Brazil) with phosphoric acid 37% was used in one group, ER: YAG laser (KAVO) and phosphoric acid 37% in another group and laser alone in the third group.[15]
The study similar to our study was done by Pourhashemi et al. in Tehran University. The results indicate significant statistical difference between Case and control group. In the present study, the samples after 6 months were divided into three groups: 1) sealants are completely retained, 2) sealants are partially lost, 3) sealants are completely lost but in the Pourhashemi, s study, samples were divided into two groups 1) sealants are completely retained, 2) sealants are fallen and they were evaluated for 3 times through 1 year. Also, bur used in that study was diamond knife edge bur No.2 and another difference of this study was less sample number.
In the study achieved by Richard khanna et al. and with aim to compare enameloplasty technique with conventional technique via electronic scan microscopy (SEM), results showed that the extended penetrance of sealant by invasive technique was apparently more compared with conventional method and has less bubbles and gaps. The performance method in this study was in-vitro and the sample number used was 16 molar teeth that were low compared with other in-vitro researches.[6,8,14–16] S.B Geiger et al. believe that in teeth that is not mechanically prepared, filling of fissures is incomplete and teeth that is mechanically prepared, indicates less micro-leakage.[11] Various studies indicate that increasing enamel surface using of mechanical method increases sealant thickness and finally increasing sealant retention.[7]. The other way to increase integrity and sealant retention on pits and fissures that are widened with a bur is that outer layer which included prism-less layer is removed via this method.[12] Other research achieved by Pakdel et al. in Azad University aims to assess the effectiveness of enamel preparation on fissure sealant micro-leakage as in-vitro method. They concluded that enamel preparation with bur and acid etching cause to reduce micro-leakage.
In past, few clinical studies similar to the present study were achieved. The number of in-vitro studies[6,8,14–16] was more in which they didn't measure the real amount of retention of sealant, but they assessed the amount of penetration of sealant to enamel fissures or in other words, the length of resin tags. The results of these studies can be hardly generalized to clinical situations, because it is uncertain that whether with increasing the length of tags, the clinical retention rate also increased or not. The success of fissure sealant depends on its adhesion to enamel and its retention.[8] position of teeth in mouth, dentist's master and method can affect the clinical success.
Conclusion
Enamel preparation causes to increase fissure sealant retention in the samples of the present study but it was not statistically significant.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared
References
- 1.Waggoner WF, Siegal M. pit and fissure sealant application: Updating the technique. Am J Dent. 1996;127:351–61. doi: 10.14219/jada.archive.1996.0205. [DOI] [PubMed] [Google Scholar]
- 2.Ripa LW. Sealants revisited: An update of the effectiveness of pit and fissure sealant. Caries Res. 1993;27:77–82. doi: 10.1159/000261608. [DOI] [PubMed] [Google Scholar]
- 3.Brocklehurst PR, Joshi RI, Northeast SE. The effect of air polishing occlusal surfaces on the penetration of fissures by a sealant. Int J Paediatr Dent. 1992;90:157–62. doi: 10.1111/j.1365-263x.1992.tb00029.x. [DOI] [PubMed] [Google Scholar]
- 4.Brokmam SL, Scott RL, Eick JD. The effect of an air-polishing device on tensile bond strength of a dental sealant. Quintessenc Int. 1989;20:211–7. [PubMed] [Google Scholar]
- 5.Keen DS, Parkins FM, Crim GA. Microleakage of composite restorations preparations prepared with air abrasive techniques. J Dent Res. 1995;65:321–27. [Google Scholar]
- 6.Courson F, Renda AM, Attal J, Bouter D, Ruse D, Degrange M. In vitro evaluation of different techniques of enamel preparation for pit and fissure sealing. J Adhes Dent. 2003;5:313–21. [PubMed] [Google Scholar]
- 7.Feldens EG, Feldense CA, de Araujo FB, Souza MA. Invasive technique of pit and fissure sealants in primary molars: A SEM study. J Clin Pediatr Dent. 1994;18:187–90. [PubMed] [Google Scholar]
- 8.Eronate N, Bardakçi Y, Sipahi M. Effects of different preparation techniques on the microleakage of compomer and resin fissure sealants. J Dent child. 2003;70:250–3. [PubMed] [Google Scholar]
- 9.Khanna R, Pandey RK, Singh N, Agarwal A. A comparison of enameloplasty sealant technique with conventional sealant technique: A scanning electron microscope study. J Indian Soc Pedod Prevent Dent. 2009;27:158–63. doi: 10.4103/0970-4388.57096. [DOI] [PubMed] [Google Scholar]
- 10.Mc Donald RE, Avery DR, Dean JA. 8th ed. Maryland Heights, Missouri: Mosby Elsevier Co; 2007. Dentistry for the child and adolescent. [Google Scholar]
- 11.Geiger SB, Gulayev S, Weiss EL. Improving fissure sealant quality: Mechanical preparation and filling level. J Dent. 2000;28:407–12. doi: 10.1016/s0300-5712(00)00016-6. [DOI] [PubMed] [Google Scholar]
- 12.Garcia-Godoy F, de Araujo FB. Enhancement of fissure sealant penetration and adaptation: The enameloplasty technique. J Clin Pediatr Dent. 1994;19:13–8. [PubMed] [Google Scholar]
- 13.Castro L, Galvão AC. Comparison of three different preparation methods in the improvement of sealant retention. J Clin Pediatr Dent. 2004;28:3. doi: 10.17796/jcpd.28.3.6601q47p5364206p. [DOI] [PubMed] [Google Scholar]
- 14.Yazici AR, Kiremitçi A, Celik C, Ozgünaltay G, Dayangaç B. A two-year clinical evaluation of pit and fissure sealants placed with and without air abrasion pretreatment in teenagers. J Am Dent Assoc. 2006;137:1401–5. doi: 10.14219/jada.archive.2006.0052. [DOI] [PubMed] [Google Scholar]
- 15.Youssef M, Youssef F, Souza-Zaroni W. Effect of enamel preparation method on in vitro marginal micro leakage of a flowable composite used as pit and fissure sealant. Int J Clin Pediatr Dent. 2006;16:342–7. doi: 10.1111/j.1365-263X.2006.00751.x. [DOI] [PubMed] [Google Scholar]
- 16.Manhart J, Huth KC, Chen HY, Hickel R. Influence of the pretreatment of occlusal pits and fissures on the retention of a fissure sealant. Am J Dent. 2004;17:12–8. [PubMed] [Google Scholar]