
Figure 1.
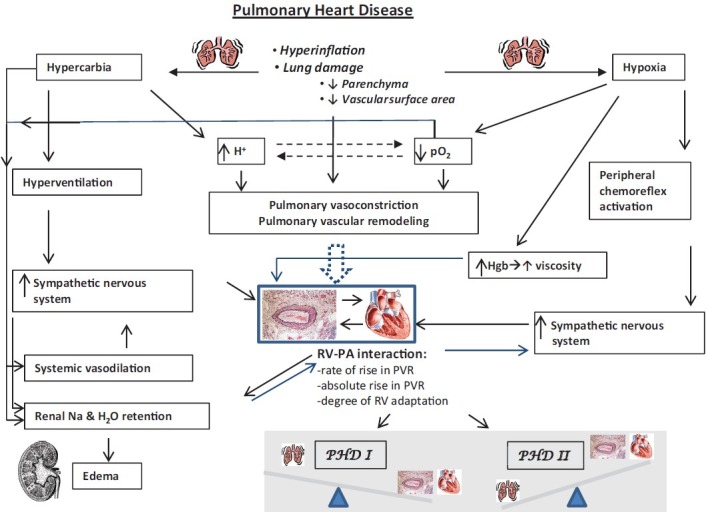
Flow diagram depicts the varying effects that abnormal lung structure and function may have an integrated physiology. Note the numerous ways in which abnormal respiratory structure and function can affect the pulmonary vascular structure and function. Similarly, how these perturbations can either directly, indirectly, or via feedback mechanisms, effect cardiac (especially right ventricular) function. A key concept in this diagram is how these varying pathophysiologic stimuli affect the cardiopulmonary unit, and namely, the right ventricular-pulmonary arterial interaction (RV-PA interaction). The nature of the RV-PA interaction dictates the relative impact of any given degree of pulmonary hypertension and pulmonary vascular disease on overall circulatory homeostasis. If the RV-PA interaction permits for relative adaptation of the RV to RV afterload, typically, the degree of lung pathology will predominate over the degree of RV-PA pathology. In this case, the type I PHD phenotype is present, where the respiratory pathology dominates the clinical picture. If there is a maladaptive RV-PA interaction, the degree of RV dysfunction and pulmonary vascular disease will often override the lung pathology, and the type II PHD phenotype is present.