
Figure 2.
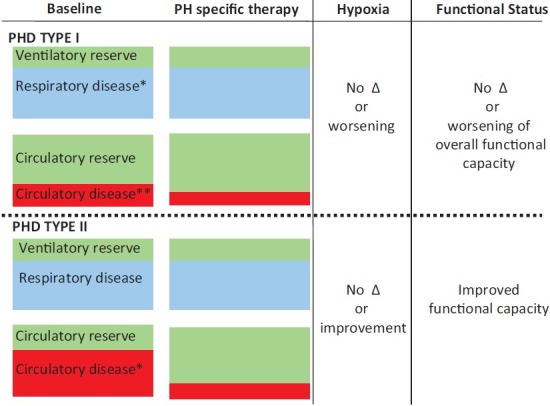
Illustrates the qualitative degree of respiratory disease (blue) and ventilatory reserve (green) as well as circulatory disease (red) and reserve (green) of subjects with Type I (top half of figure) and Type II pulmonary heart disease (bottom half of figure). Note that in the Type I phenotype, there is significant respiratory disease at baseline; the degree of respiratory disease >degree of circulatory disease. Therefore, the circulatory reserve is >degree of ventilatory reserve. In response to PH specific therapy, the balance of respiratory disease and ventilatory reserve remain unchanged. The degree of circulatory disease decreases modestly, with a small increase in circulatory reserve. Given no change in the respiratory disease in response to therapy and only a small improvement in circulatory function, there is no net change in functional capacity. If oxygenation worsens significantly, the functional status may even decline. Note that in the Type II phenotype, there is a similar degree of baseline respiratory disease and ventilatory reserve as seen in the Type I subject. However, there is a much greater degree of circulatory disease, such that the degree of circulatory disease is comparable to the degree of respiratory disease. As such, the degree of circulatory reserve is much lower than in the type I PHD example. In response to PH specific therapy, the balance of respiratory disease and ventilatory reserve remain unchanged. However, the degree of circulatory disease decreases substantially while there is a significant improvement in circulatory reserve. The degree of hypoxia may not change, or may even improve. This most often leads to a net improvement in functional status. *Respiratory disease-may refer to obstructive or restrictive respiratory disorders. **Circulatory disease-refers to the severity of right ventricular afterload (pulmonary vascular resistance) and the degree of right ventricular dysfunction.