
Figure 1.
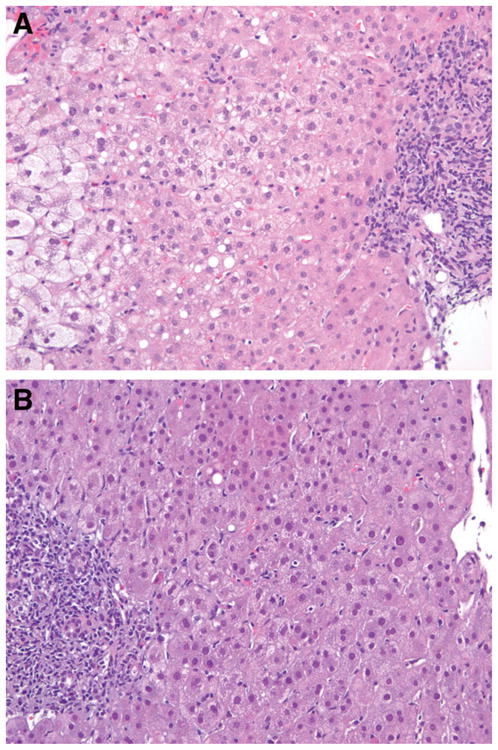
(A) Severe cholestatic HCV infection 4 months after the first transplant. The left side of the slide shows intense pericentral hepatocyte balloon degeneration. On the right, a portal tract can be seen with focal periportal cholestatic ductular proliferation and lymphocytic inflammation indicative of recurrent cholestatic DCV (hematoxylin and eosin stain, magnification ×200). (B) Recurrent HCV infection 3 months after the second transplant. On the right side, a central vein can be seen with normal pericentral hepatocytes and without ballooning. On the left, a portal tract can be seen with moderate lymphocytic inflammation that is characteristic of an early recurrent HCV infection. In the lobular parenchyma between the portal tract and central vein, there is mild inflammation with scattered sinusoidal lymphocytes and a single necrotic hepatocyte near the portal tract; these are typical features of recurrent HCV infections.