
Figure 11.
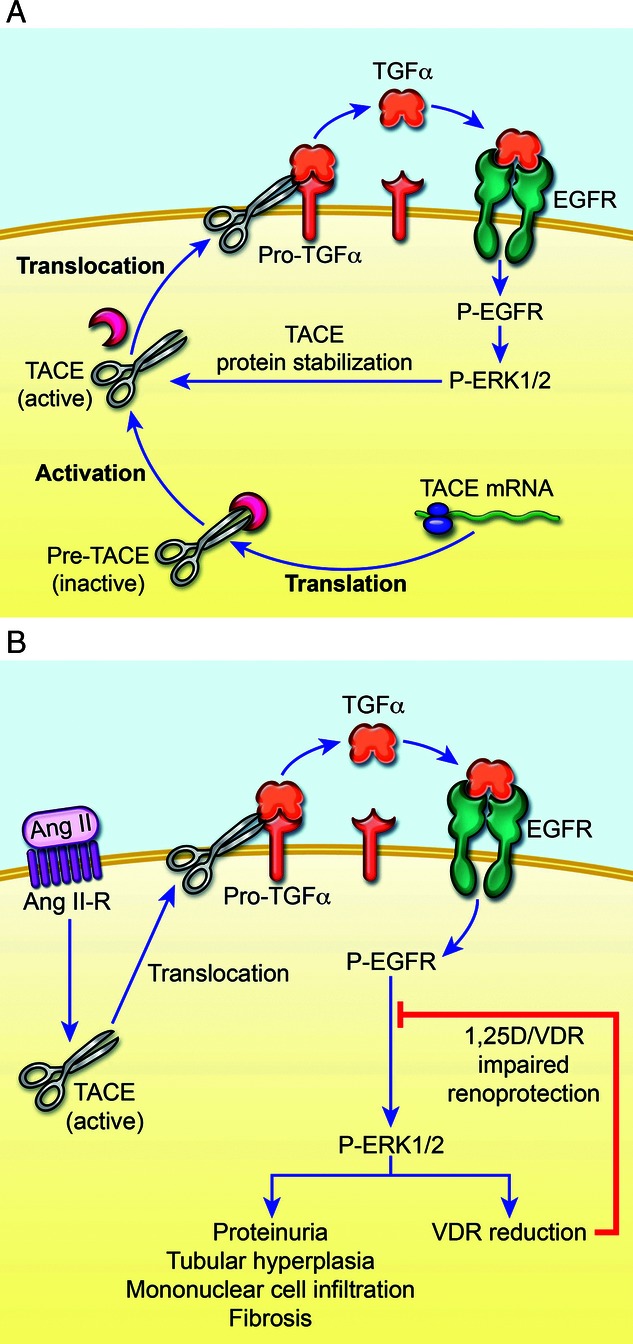
A,B. Angiotensin–II Control of TACE, TGF-α, and EGF-R in Parathyroid and Kidney (Adapted from: Dusso A, Gonzalez EA, Martin KJ. Vitamin D in chronic kidney disease. Best Pract Res Clin Endocrinol Metab 2011; 25: 647–655, and Dusso A, Arcidiacono MV, Yang J, Tokumoto M. Vitamin D inhibition of TACE and prevention of renal osteodystrophy and cardiovascular mortality. J Steroid Biochem Mol Biol 2010; 121: 193–198.) (A) Intracellular TACE (tumor necrosis factor alpha converting enzyme) translated from its mRNA in an inactive form has activation and translocation to membrane accomplished by removal of an inhibitory component. TACE in its active form is strongly stabilized by the phosphorylated EGFR (epidermal growth factor receptor) via P-ERK1/2 forming a “feed-forward” loop with TACE action via its sheddase action on Pro-TGF-α (transforming growth factor alpha [TGF-α]) generating TGF-α able to activate more EGFR and continue the cycle resulting in more generation of each participant in a “vicious cycle” with marked pathologic consequences. P-ERK ½ (extracellular signal related kinase or MAP-kinase) a general form of kinase involved in cellular effect amplifications. (B) Angiotensin II (ANG II) together with its receptor shown as the activating and translocating factor for TACE acting to generate TGF-α as the main ligand for EGFR, which when phosphorylated acts via P-ERK ½ in many pathologic roles in renal disease. P-ERK ½ diminishes the activity of calcitriol by lowering VDR levels. In parathyroids, the P-EGFR translocates to nucleus to markedly stimulate cyclin enzymes producing parathyroid hyperplasia.