

Abstract
AIM: To measure patient perceptions about preventing hepatocellular carcinoma (HCC) and to predict the factors that influence patient willingness to receive therapy.
METHODS: A cross-sectional descriptive study was conducted at an outpatient clinic of a medical institution in southern Taiwan. Four hundred patients with chronic hepatitis B/C were recruited as participants. Two structured questionnaires based on the health belief model were utilized in this study, including the scales of perceptions about preventing HCC and knowledge of hepatitis B/C.
RESULTS: The statistical results demonstrated that the participants’ perceived susceptibility (r = -0.22, P < 0.001), benefits (r = -0.11, P = 0.028) and cues to action (r = -0.12, P = 0.014) about the prevention of HCC was significantly correlated with their age. The participants’ perceptions were also associated with their educational levels, household incomes and knowledge of hepatitis. Older patients and those with a lower socioeconomic status tended to have negative perceptions and less knowledge of hepatitis. Multivariate logistic regression further indicated that the participants’ age (B = -0.044, SE = 0.017, odds ratio = 0.957, P = 0.008, 95%CI: 0.926-0.989) and perceived barriers (B = -0.111, SE = 0.030, odds ratio = 0.895, P < 0.001, 95%CI: 0.845-0.949) were correlated with their willingness to receive antiviral therapy.
CONCLUSION: Healthcare professionals should provide appropriate and effective guidance to increase their patients’ awareness and to decrease the perceived barriers for continuing surveillance and antiviral therapy.
Keywords: Antiviral therapy, Health perception, Hepatitis B, Hepatitis C, Hepatocellular carcinoma, Health knowledge
Core tip: Chronic hepatitis B/C carriers may benefit from regular surveillance for allowing an early diagnose of hepatocellular carcinoma (HCC). In addition, raising awareness of and health perceptions about HCC, and increasing willingness to receive antiviral therapy for preventing the development of HCC are crucial in patients with chronic hepatitis B/C, particularly in rural areas.
INTRODUCTION
Chronic liver disease is the eighth most common cause of death, and hepatocellular carcinoma (HCC) is the second leading cause of cancer-related death in Taiwan[1]. More than 80% of primary HCC is attributed to chronic infection with hepatitis B/C viruses[2,3]. To prevent further development of HCC, patients infected with hepatitis B/C should maintain a healthy lifestyle, reduce alcohol consumption, undergo regular liver function tests and abdominal sonography, and receive antiviral therapy, if necessary[4,5]. Chronic infection with hepatitis B/C is the most important cause of HCC. The early development of HCC is asymptomatic, and patients with chronic hepatitis are usually unaware of their carrier status, the symptoms and signs of HCC, and the importance of regular surveillance and treatment. During the early stage of HCC, when tumors are less than 2 cm in diameter, even expert radiologists have difficulty differentiating a cirrhotic nodule from a malignant tumor[4]. These tumors are highly heterogeneous, and HCC is nearly always fatal once the tumors cannot be eradicated by surgical or ablative approaches[4]. In addition, patients with HCC detected at the early asymptomatic stage have better survival rates than those who are diagnosed when symptomatic[6]. Therefore, increasing awareness of and health perceptions about HCC are crucial in patients with chronic hepatitis B/C, particularly in rural areas.
Perceptions about preventing HCC
Henchoz et al[7] defined perceived health as “an individual’s evaluation of his or her own health” which can determine personal health values and influence health behaviors[8]. Furthermore, Kartal et al[9] stated that “self-perceived health is a subjective measure that can be calculated at an individual level. It gives an indication of how an individual feels about the condition of his/her own health.” To examine patient perceptions about preventing HCC, a health belief model was utilized as a theoretical framework in the present study. The health belief model was formulated using five concepts to explain attitudes and behaviors of individuals, including perceived susceptibility, perceived severity, perceived benefits of action, perceived barriers to action, and cues to action[10,11]. The model was developed to predict compliance with preventive health recommendations[6,12] and to specify the individuals’ values and beliefs about health and their influence on choices, especially for explaining screening behaviors[2,13].
Perceived susceptibility refers to a person’s experience with a potentially harmful condition[11]. This concept measures whether patients with asymptomatic hepatitis perceive themselves as being at high risk and believe that they could acquire HCC. Perceived severity indicates individual concerns about the seriousness and consequences to the quality of life upon development of cancer, including the physical, mental, and social perspectives[11]. This concept can measure the impact of chronic hepatitis on a person’s life and his or her belief that people infected could possibly die from liver cancer.
Perceived benefits of action refer to whether one believes the potential effectiveness of recommended health actions in preventing or reducing the risk or seriousness of a disease[11]. Perceived benefits of action can assess one’s beliefs that regular screening and antiviral therapy reduce the risks of progressing to liver cirrhosis and cancer.
Perceived barriers to action are the negative aspects of anticipated health behaviors that patients adopt for prevention or early detection of hepatic cancer, such as the inconvenience of seeing a doctor, the waiting time and pain involved in giving blood samples, and the side effects from taking medications. Patients may believe that regular screening of liver function and abdominal sonography are not necessary if they do not experience any symptoms of discomfort. Moreover, if patients receive antiviral therapy, they may develop physical and psychological side effects, such as fever, headache, fatigue, nausea, vomiting, anxiety and even depression. These adverse events often make patients feel uncomfortable, resulting in early withdrawal from therapy.
Cues to action measure the perceived social and environmental influences that stimulate an individual’s desire to take health-related action[11]. The concept can assess whether individuals with hepatitis have any family members, relatives or friends who are infected with hepatitis or whether the patients have ever followed the advice of healthcare professionals about regular check-ups of liver function, abdominal sonography, and antiviral therapy. Therefore, the five concepts of the health belief model were applied in the present study to explore health perceptions about preventing HCC among patients with chronic hepatitis B/C.
Knowledge of hepatitis
Most people are not aware of the routes of viral transmission of hepatitis B/C and that these viruses spread more easily than the human immunodeficiency virus[14]. Ma et al[15] found that populations with minimal education and low socioeconomic status are vulnerable to hepatitis infection. If high-risk groups with chronic hepatitis are not aware of the importance of regular surveillance and antiviral therapy, then their condition could gradually progress to liver cirrhosis and hepatic cancer. Wai et al[16] identified that those hepatitis B carriers with high knowledge were significantly younger, and more likely to have received college education in Singapore. Treloar et al[17] conducted a cross-sectional survey and indicated that knowledge is a precursor to decisions about treatment of hepatitis C, particularly for those patients who are less engaged with hepatitis C treatment and those with lower literacy.
The prevention of HCC in high-risk populations depends on regular serum screening, abdominal sonography and antiviral therapy. Regular screening of liver function, including assays to measure serum aspartate aminotransferase and alanine aminotransferase levels, α-fetoprotein assays and abdominal sonography are strongly recommended for patients with chronic hepatitis to ensure earlier detection of HCC and better survival[6,18]. Therefore, the purpose of the present study was to measure patient perceptions about the prevention of HCC, knowledge of hepatitis B/C, and frequency of hepatic check-ups, as well as to predict the factors that influence patient willingness to receive antiviral therapy.
MATERIALS AND METHODS
Participants
Four hundred patients with chronic hepatitis B/C from the outpatient clinic in a medical institution were recruited as participants. The teaching hospital is located in a rural area in southern Taiwan. The markers for hepatitis B are positive hepatitis B surface antigen (HBsAg) and positive antibody for hepatitis C (anti-HCV)[18]. The inclusion criteria for participants were (1) HBsAg (+) and anti-HBs (-), and/or (2) anti-HCV (+) in serum tests for more than 6 mo. The patients who were younger than 18 years and those who did not meet the inclusion criteria were excluded from this study. The sampling schema is shown in Figure 1.
Figure 1.
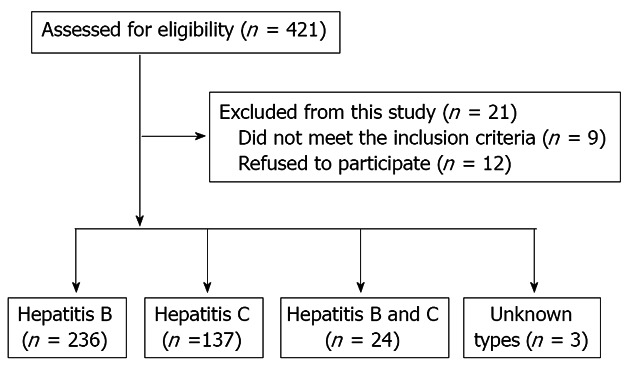
Sampling schema.
Instruments
This study had a cross-sectional, descriptive design. Two structured questionnaires developed by Chao et al[19] and based on a health belief model were utilized in this investigation, namely, the scales of perceptions about preventing HCC and knowledge of hepatitis B/C. After obtaining permission from the original developers, a pilot test was conducted with 40 target adults (who did not participate in the main study) to examine whether there were any ambiguous statements in the questionnaires and to establish the reliability and validity of the instruments.
The scale of perceptions about preventing HCC consisted of five dimensions and 34 items, including the dimensions of perceived susceptibility (3 items), perceived severity (5 items), perceived benefits (3 items), perceived barriers (15 items), and cues to action (8 items). Each item was designed as a 5-point Likert scale, ranging from 1 “strongly disagree” to 5 “strongly agree.” Higher scores indicated greater degrees of perceived susceptibility, severity, benefits, barriers and cues to action. Cronbach’s alpha values were as follows: whole scale, 0.8; perceived susceptibility, 0.71; perceived severity, 0.78; perceived benefits, 0.68; perceived barriers, 0.84; and cues to action, 0.77[19]. The internal consistency reliability with Cronbach’s alpha was 0.72 in this study. The values of Cronbach’s alpha for each dimension of perception indicated the reliability of the questionnaire utilized in this study.
The scale of knowledge of hepatitis B/C had 15 items, including liver function (2 items), blood tests for hepatitis (1 item), symptoms of hepatitis (2 items), definition of hepatitis (1 item), modes of viral transmission (4 items), screening to prevent liver cancer (2 items) and infectious status of hepatitis (3 items). Participants responded to these items using the following options: 0 = “do not know” or “false” and 1 = “true.” The total scores of 15 items represented a dimension of the participants’ knowledge. A higher score indicated a better understanding of hepatitis. The internal consistency with the Kuder-Richardson coefficient was previously determined to be 0.71[19], whereas in the present study, the Kuder-Richardson coefficient was 0.62.
Procedure
Approval to conduct this study was obtained from the institutional review board. This study was conducted between January and December of 2010. When patients visited the outpatient hepatic clinic and met the inclusion criteria, the researchers used convenient sampling to choose the participants. Subsequently, the participants were placed in another room to complete the questionnaires without interruption. All of the questionnaires were anonymous and separated from the consent forms. Prior to administering the questionnaires, the researchers informed the patients of the purpose of this study and explained that the responses would not influence their treatment.
Statistical analysis
The Statistical Package for the Social Sciences (SPSS, Chicago, IL, United States) version 17.0 was used to analyze the data. The data analysis for this study included descriptive statistics, independent-samples t-tests, the chi-square test, a one-way analysis of variance (ANOVA), Pearson’s correlation, and logistic regression.
RESULTS
Participants’ demographics
Four hundred questionnaires were distributed and completed by 174 females (43.5%) and 226 males (56.5%). The average age of the respondents was 54 years (rang: 18-89 years). The participants’ demographic information is summarized in Table 1.
Table 1.
Participants’ demographics (n = 400) n (%)
| Participants’ demographics | Value |
| Gender | |
| Female | 174 (43.5) |
| Male | 226 (56.5) |
| Marital status | |
| Married | 353 (88.3) |
| Single | 27 (6.8) |
| Widowed | 10 (2.5) |
| Divorced/separated | 9 (2.3) |
| Educational level | |
| Illiterate | 41 (10.3) |
| Elementary school | 109 (27.3) |
| Junior high school | 73 (18.3) |
| High school | 104 (26) |
| College/university | 62 (15.5) |
| Graduate school | 11 (2.8) |
| Occupation | |
| Laborers | 82 (20.5) |
| Businessmen | 61 (15.3) |
| Farmers | 36 (9.0) |
| Fishermen | 9 (2.3) |
| Military personnel | 2 (0.5) |
| Government employees | 19 (4.8) |
| Homemakers | 78 (19.5) |
| Others | 113 (28.3) |
| Household income (NT dollars/mo) | |
| Below 10000 | 101 (25.3) |
| 10000-20000 | 63 (15.8) |
| 21000-30000 | 78 (19.5) |
| 31000-40000 | 47 (11.8) |
| 41000-50000 | 35 (8.8) |
| Above 50000 | 76 (19.0) |
Participants’ hepatitis-related information
In this survey, 236 (59%) participants had hepatitis B, and 137 (34.3%) had hepatitis C. Twenty-four (6.0%) participants reported having both hepatitis B and C, and three (0.5%) did not know what types of hepatitis they had. In terms of vaccination, 298 patients (74.5%) responded that they had never been vaccinated for hepatitis B. Thirty-eight patients (9.5%) had received the vaccine, and 64 (16.0%) did not know if they had been vaccinated.
Most of the patients (n = 292, 73.0%) reported that the virus had been found during a regular physical examination, 45 (11.3%) through the screening process for blood donation, 21 (5.3%) upon health screening in the community and 42 (10.5%) in other ways. Moreover, 332 patients (83.0%) were willing to receive antiviral therapy, 35 patients (8.8%) did not want to receive the therapy, and 33 patients (8.3%) were unaware that this antiviral therapy was available or whether they needed to receive this therapy.
Regarding the sources of hepatitis-related health information, 282 participants stated that they obtained this information from healthcare professionals, 189 from their relatives and friends, 220 from television, 173 from newspapers and magazines, and 70 from educational pamphlets or brochures. In addition, over one-half of the participants underwent regular blood screening every 3 mo (n = 247, 61.8%) and abdominal sonography every 6 mo (n = 183, 45.8%) according to the statistical results.
Health perceptions and knowledge of hepatitis
The mean scores for each dimension of the health perceptions were as follows: perceived susceptibility, 10.26 ± 2.18; perceived severity, 20.43 ± 3.53; perceived benefits, 12.07 ± 1.63; perceived barriers, 37.60 ± 7.06; and cues to action, 27.01 ± 4.73. The mean score for knowledge of hepatitis B/C in this study was 7.36 ± 1.87.
Relationships among the patients’ demographics, health perceptions, knowledge, screening, and willingness to receive antiviral therapy
Pearson’s correlation revealed significantly negative correlations between the participants’ age and their health perceptions, except for perceived severity and barriers. Likewise, the participants’ age was significantly and negatively correlated with their level of knowledge (γ = -0.20, P < 0.001). The statistical results also suggested that the participants’ perceptions had a significantly positive correlation with their knowledge of hepatitis. In addition, the patients’ gender was not significantly correlated with their perceptions (except for perceived barriers) and knowledge, as presented in Table 2.
Table 2.
Relationships between the participants' demographics, health perceptions, and knowledge of hepatitis (n = 400)
| Variables | Perceived susceptibility | Perceived severity | Perceived benefits | Perceived barriers | Cues to action | Knowledge |
| Age1 | -0.22 (< 0.001) | -0.07 (0.162) | -0.11 (0.028) | 0.08 (0.121) | -0.12 (0.014) | -0.20 (< 0.001) |
| Gender2 | 1.53 (0.135) | 0.92 (0.362) | 0.23 (0.819) | 2.14 (0.039) | -0.04 (0.967) | -1.14 (0.254) |
| Marital status3 | 0.64 (0.589) | 1.91 (0.127) | 0.40 (0.753) | 0.19 (0.905) | 0.08 (0.973) | 1.13 (0.336) |
| Education level3 | 2.96 (0.008) | 1.30 (0.257) | 3.95 (0.001) | 6.31 (<0.001) | 2.27 (0.036) | 9.17 (< 0.001) |
| Occupation3 | 2.52 (0.015) | 0.92 (0.489) | 0.92 (0.490) | 2.55 (0.014) | 0.59 (0.767) | 2.61 (0.012) |
| Monthly income3 | 2.27 (0.047) | 0.63 (0.679) | 3.91 (0.002) | 3.91 (0.002) | 2.87 (0.015) | 6.59 (< 0.001) |
| Willingness to receive therapy3 | -0.75 (0.453) | -1.15 (0.252) | -0.42 (0.675) | 3.55 (< 0.001) | -1.67 (0.096) | -0.48 (0.633) |
| Had received a vaccine3 | 2.98 (0.052) | 0.07 (0.937) | 2.04 (0.131) | 1.94 (0.145) | 3.14 (0.044) | 13.88 (< 0.001) |
| Frequency of blood screening3 | 1.28 (0.265) | 3.67 (0.001) | 0.43 (0.859) | 1.87 (0.084) | 1.66 (0.129) | 1.44 (0.198) |
| Frequency of abd. sonography3 | 0.51 (0.830) | 1.44 (0.188) | 0.55 (0.798) | 3.66 (0.001) | 1.48 (0.173) | 2.74 (0.009) |
Data are presented as
r of Pearson’s correlation/
t of independent t-test/
F of one-way analysis of variance (P value).
Moreover, a one-way ANOVA indicated that there were significantly positive correlations between the participants’ educational levels and their perceptions (except for perceived severity) and knowledge of hepatitis. Significant relationships were found between the patients’ frequency of blood screening for HCC prevention and the perceived severity (F = 3.67, P = 0.001) as well as between the frequency of abdominal sonography and perceived barriers (F = 3.66, P = 0.001).
Furthermore, the frequency of abdominal sonography was significantly correlated with the patients’ knowledge (F = 2.74, P = 0.009) and with being vaccinated (F = 13.88, P < 0.001). A significant correlation existed between the participants’ willingness to receive antiviral therapy and perceived barriers (F = 3.55, P < 0.001). The researchers further divided the participants into three groups by age (18-39 years, 40-64 years, and 65-89 years old). A significantly positive correlation was found between the participants’ age and their willingness to receive antiviral therapy (χ2 = 13.97, P = 0.007), but there was no correlation between the participants’ gender and their willingness to receive therapy (χ2 = 2.35, P = 0.309).
Predictors for willingness to receive antiviral therapy
The participants’ age, five dimensions of health perceptions and knowledge of hepatitis were analyzed as independent variables in the multivariate logistic regression. The results indicated that the participants’ age (B = -0.044, SE = 0.017, odds ratio= 0.957, P = 0.008, 95%CI: 0.926-0.989) and perceived barriers (B = -0.111, SE = 0.030, odds ratio = 0.895, P < 0.001, 95%CI: 0.845-0.949) were significantly associated with their willingness to receive antiviral therapy, as presented in Table 3. Adjusting for other effects in the logistic regression model, for every one-year increase in age, the participants were 0.957 times less likely to have received antiviral therapy.
Table 3.
Predictors of receiving antiviral therapy: Logistic regression (n = 364)
| Variables | B | SE | OR | P | 95%CI |
| Age | -0.044 | 0.017 | 0.957 | 0.008 | 0.926-0.989 |
| Perceptions | |||||
| Susceptibility | 0.011 | 0.096 | 1.011 | 0.912 | 0.837-1.220 |
| Severity | 0.061 | 0.053 | 1.063 | 0.255 | 0.957-1.180 |
| Benefits | -0.156 | 0.130 | 0.856 | 0.232 | 0.663-1.105 |
| Barriers | -0.111 | 0.030 | 0.895 | < 0.001 | 0.845-0.949 |
| Cues to action | 0.059 | 0.042 | 1.060 | 0.160 | 0.977-1.150 |
| Knowledge | -0.102 | 0.117 | 0.903 | 0.383 | 0.719-1.135 |
DISCUSSION
Most of the participants in this study had elementary and high school educations, and their household incomes were between $10000 and $ 30000 NT dollars. The patients in rural areas had lower educational levels and household incomes than those in urban areas. The results revealed that the participants’ education levels were significantly correlated with their health perceptions and knowledge about hepatitis. This finding is consistent with the previous study[16,20]. The participants’ education levels were not associated with the perceived severity in this study, which may be because the patients themselves might not have perceived the potentially severe consequences of being hepatitis carriers and might not have been aware of the asymptomatic development of HCC.
In addition, Hsu et al[21] stated that educational attainment and knowledge of hepatitis B are associated with individual willingness to receive screening and vaccination. As previous studies have indicated, subjects with higher levels of knowledge were significantly more likely to receive blood screening for hepatitis B and to have received the vaccine[14,22-25]. However, the majority of the participants responded that they had never been vaccinated for hepatitis B prior to infection. Therefore, healthcare providers should educate patients with chronic hepatitis to increase their awareness and knowledge and to take action for prevention or early detection of HCC.
Likewise, household income was significantly and positively correlated with perceived susceptibility, benefits, barriers, cues to action, and knowledge. This finding revealed that patients with lower incomes perceived less susceptibility, benefits, and cues to action for preventing liver cancer, and they had less knowledge of hepatitis. These results were similar to those of a previous study[14]. Thus, it is necessary to focus on the low socioeconomic population and to increase their perceptions and knowledge to reduce health disparities about liver cancer in the community.
Moreover, the vast majority of the participants usually obtained hepatitis-related health information and knowledge from healthcare professionals, public media (such as television, newspapers and magazines), and educational brochures and pamphlets. Cacoub et al[26] indicated that the therapeutic education for those hepatitis patients can improve the probability of compliance with antiviral therapy. Hence, to raise perceptions and knowledge related to HCC, appropriate and effective instruction based on the individual’s age and educational level is crucial, especially in rural areas.
Furthermore, the predictors for patient willingness to receive antiviral therapy were age and the perceived barriers. The participants’ age was negatively associated with their health perceptions and knowledge of hepatitis. This finding indicates that elderly patients tend to have lower perceived susceptibilities, benefits, and cues to action for prevention of liver cancer; less knowledge about hepatitis; and less willingness to receive antiviral therapy. Similarly, Henchoz et al[7] found that the paradox between health status and health perception diverges with advancing age.
Conversely, the participants’ perceived barriers had a significantly negative relationship to their willingness to receive antiviral therapy. High barriers to screening and adverse consequences from antiviral therapy such as pain, high costs, and time expenditure may discourage patients from regular screenings and cause them to withdraw early from antiviral therapy. This finding is also consistent with previous studies[2,19]. Thus, identifying the patients’ inherent barriers is the first crucial step for increasing participation in preventive behaviors[2].
There were two limitations in the present study. Because the participants were restricted to an outpatient clinic of a rural medical institution, generalization beyond this population may be limited. Further research should be conducted in multiple diverse areas. In addition, this study had a cross-sectional descriptive design, and its analytic results do not indicate causality.
In conclusion, patient health perceptions about preventing HCC are related to their age, education levels, household income, and knowledge of hepatitis. Members of the high-risk population of hepatitis B/C carriers should be aware of the serious consequences of chronic active infection and should receive regular surveillance and treatment. To successfully complete a series of medical regimens, detailed explanation and communication regarding possible adverse effects are essential before starting antiviral therapy, especially in elderly individuals. In terms of the implications for clinical practice, healthcare professionals should reduce patient discomfort and inconvenience as much as possible and should strive to remove barriers to screening and treatment. Moreover, clinicians may utilize educational programs as an intervention to increase patient perception, knowledge and willingness to receive antiviral therapy.
ACKNOWLEDGMENTS
The authors sincerely appreciate the research assistants for data collection and entry and thank the participants who provided information.
COMMENTS
Background
Chronic liver disease is the eighth most common cause of death, and hepatocellular carcinoma (HCC) is the second leading cause of cancer-related death in Taiwan. More than 80% of primary HCC is attributed to chronic infection with hepatitis B/C viruses. The early development of HCC is asymptomatic, and patients with chronic hepatitis are usually unaware of their carrier status, the symptoms and signs of HCC, and the importance of regular surveillance and treatment.
Research frontiers
The participants’ educational levels were significantly correlated to their health perceptions (except for perceived severity) and knowledge about hepatitis. The elderly patients and those with lower household incomes tend to have lower perceived susceptibility, benefits, and cues to action for prevention of HCC, less knowledge about hepatitis and less willingness to receive antiviral therapy. The results indicated that the participants’ age and perceived barriers were significantly associated with their willingness to receive antiviral therapy.
Innovations and breakthroughs
Chronic hepatitis B/C carriers may benefit from regular surveillance for allowing an early diagnose of HCC. In addition, raising awareness of and health perceptions about HCC, and increasing willingness to receive antiviral therapy for preventing the development of HCC are crucial in patients with chronic hepatitis B/C, particularly in rural areas.
Applications
In terms of the implications for clinical practice, healthcare professionals should reduce patient discomfort and inconvenience as much as possible and should strive to remove barriers to screening and treatment. Moreover, clinicians may utilize educational programs as an intervention to increase patient knowledge and willingness to receive antiviral therapy.
Terminology
Health perception is defined as “an individual’s evaluation of his or her own health”. Health perception can determine personal health values and influence health behaviors.
Peer review
The authors conducted a cross-sectional descriptive study to identify several important factors of healthy perceptions about preventing HCC in Taiwan. The participants’ age and perceived barriers were correlated with their willingness to receive antiviral therapy. The study was novel and well-constructed and the results have many implications in the field of preventive medicine.
Footnotes
Supported by E-Da Hospital, EDAHP 99021
P- Reviewers Sakamoto N, Wang K S- Editor Gou SX L- Editor A E- Editor Zhang DN
References
- 1.The statistical analysis of causes of death. [cited 2012 Jun 25] Available from: http://www.doh.gov.tw/ufile/doc/2010-statistics%20of%20cause%20of%20death.pdf.
- 2.Ma GX, Fang CY, Shive SE, Toubbeh J, Tan Y, Siu P. Risk perceptions and barriers to Hepatitis B screening and vaccination among Vietnamese immigrants. J Immigr Minor Health. 2007;9:213–220. doi: 10.1007/s10903-006-9028-4. [DOI] [PubMed] [Google Scholar]
- 3.Robotin MC, George J, Supramaniam R, Sitas F, Penman AG. Preventing primary liver cancer: how well are we faring towards a national hepatitis B strategy? Med J Aust. 2008;188:363–365. doi: 10.5694/j.1326-5377.2008.tb01656.x. [DOI] [PubMed] [Google Scholar]
- 4.Wilson JF. Liver cancer on the rise. Ann Intern Med. 2005;142:1029–1032. doi: 10.7326/0003-4819-142-12_part_1-200506210-00024. [DOI] [PubMed] [Google Scholar]
- 5.Riley TR, Smith JP. Preventive care in chronic liver disease. J Gen Intern Med. 1999;14:699–704. doi: 10.1046/j.1525-1497.1999.11188.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wai CT, Wong ML, Ng S, Cheok A, Tan MH, Chua W, Mak B, Aung MO, Lim SG. Utility of the Health Belief Model in predicting compliance of screening in patients with chronic hepatitis B. Aliment Pharmacol Ther. 2005;21:1255–1262. doi: 10.1111/j.1365-2036.2005.02497.x. [DOI] [PubMed] [Google Scholar]
- 7.Henchoz K, Cavalli S, Girardin M. Health perception and health status in advanced old age: A paradox of association. J Aging Stud. 2008;22:282–290. [Google Scholar]
- 8.Brandon LJ, Proctor L. Comparison of health perceptions and health status in African Americans and Caucasians. J Natl Med Assoc. 2010;102:590–597. doi: 10.1016/s0027-9684(15)30636-2. [DOI] [PubMed] [Google Scholar]
- 9.Kartal A, İnci FH. A cross-sectional survey of self-perceived health status and metabolic control values in patients with type 2 diabetes. Int J Nurs Stud. 2011;48:227–234. doi: 10.1016/j.ijnurstu.2010.07.004. [DOI] [PubMed] [Google Scholar]
- 10.Champion VL. Instrument development for health belief model constructs. ANS Adv Nurs Sci. 1984;6:73–85. doi: 10.1097/00012272-198404000-00011. [DOI] [PubMed] [Google Scholar]
- 11.Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2:328–335. [Google Scholar]
- 12.Armstrong SN, Anderson M, Le ET, Nguyen LH. Application of the Health Belief Model to bariatric surgery. Gastroenterol Nurs. 2009;32:171–178. doi: 10.1097/SGA.0b013e3181a7cf5a. [DOI] [PubMed] [Google Scholar]
- 13.Yarbrough SS, Braden CJ. Utility of health belief model as a guide for explaining or predicting breast cancer screening behaviours. J Adv Nurs. 2001;33:677–688. doi: 10.1046/j.1365-2648.2001.01699.x. [DOI] [PubMed] [Google Scholar]
- 14.Hislop TG, Teh C, Low A, Li L, Tu SP, Yasui Y, Taylor VM. Hepatitis B knowledge, testing and vaccination levels in Chinese immigrants to British Columbia, Canada. Can J Public Health. 2007;98:125–129. doi: 10.1007/BF03404323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ma GX, Shive SE, Toubbeh JI, Tan Y, Wu D. Knowledge, attitudes, and behaviors of Chinese hepatitis B screening and vaccination. Am J Health Behav. 2008;32:178–187. doi: 10.5555/ajhb.2008.32.2.178. [DOI] [PubMed] [Google Scholar]
- 16.Wai CT, Mak B, Chua W, Tan MH, Ng S, Cheok A, Wong ML, Lim SG. Misperceptions among patients with chronic hepatitis B in Singapore. World J Gastroenterol. 2005;11:5002–5005. doi: 10.3748/wjg.v11.i32.5002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Treloar C, Hull P, Bryant J, Hopwood M, Grebely J, Lavis Y. Factors associated with hepatitis C knowledge among a sample of treatment naive people who inject drugs. Drug Alcohol Depend. 2011;116:52–56. doi: 10.1016/j.drugalcdep.2010.11.018. [DOI] [PubMed] [Google Scholar]
- 18.Chen TH, Chen CJ, Yen MF, Lu SN, Sun CA, Huang GT, Yang PM, Lee HS, Duffy SW. Ultrasound screening and risk factors for death from hepatocellular carcinoma in a high risk group in Taiwan. Int J Cancer. 2002;98:257–261. doi: 10.1002/ijc.10122. [DOI] [PubMed] [Google Scholar]
- 19.Chao WH, Huang MC. Use of the health belief model in predicting screening among HBsAg positive staff in a medical center. Unpublished master’s dissertation. Taiwan: National Cheng Kung University; 2008. p. 134. [Google Scholar]
- 20.Thompson MJ, Taylor VM, Yasui Y, Hislop TG, Jackson JC, Kuniyuki A, Teh C. Hepatitis B knowledge and practices among Chinese Canadian women in Vancouver, British Columbia. Can J Public Health. 2003;94:281–286. doi: 10.1007/BF03403606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hsu CE, Zhang G, Yan FA, Shang N, Le T. What made a successful hepatitis B program for reducing liver cancer disparities: an examination of baseline characteristics and educational intervention, infection status, and missing responses of at-risk Asian Americans. J Community Health. 2010;35:325–335. doi: 10.1007/s10900-010-9238-5. [DOI] [PubMed] [Google Scholar]
- 22.Chan OK, Lao TT, Suen SS, Lau TK, Leung TY. Knowledge on hepatitis B infection among pregnant women in a high endemicity area. Patient Educ Couns. 2011;85:516–520. doi: 10.1016/j.pec.2010.11.006. [DOI] [PubMed] [Google Scholar]
- 23.Hwang JP, Huang CH, Yi JK. Knowledge about hepatitis B and predictors of hepatitis B vaccination among Vietnamese American college students. J Am Coll Health. 2008;56:377–382. doi: 10.3200/JACH.56.44.377-382. [DOI] [PubMed] [Google Scholar]
- 24.Yamazhan T, Durusoy R, Tasbakan MI, Tokem Y, Pullukcu H, Sipahi OR, Ulusoy S. Nursing students’ immunisation status and knowledge about viral hepatitis in Turkey: a multi-centre cross-sectional study. Int Nurs Rev. 2011;58:181–185. doi: 10.1111/j.1466-7657.2010.00869.x. [DOI] [PubMed] [Google Scholar]
- 25.Wang WL, Wang CJ, Tseng HF. Comparing knowledge, health beliefs, and self-efficacy toward hepatitis B prevention among university students with different hepatitis B virus infectious statuses. J Nurs Res. 2009;17:10–19. doi: 10.1097/JNR.0b013e3181999ca3. [DOI] [PubMed] [Google Scholar]
- 26.Cacoub P, Ouzan D, Melin P, Lang JP, Rotily M, Fontanges T, Varastet M, Chousterman M, Marcellin P. Patient education improves adherence to peg-interferon and ribavirin in chronic genotype 2 or 3 hepatitis C virus infection: a prospective, real-life, observational study. World J Gastroenterol. 2008;14:6195–6203. doi: 10.3748/wjg.14.6195. [DOI] [PMC free article] [PubMed] [Google Scholar]