

Introduction
The ground has shifted in US health care. With President Obama's reelection in November 2012, the Affordable Care Act is here to stay, and tens of millions of Americans soon will gain access to health insurance. Numerous experiments are underway to better organize and coordinate care at the levels of the individual practice, the “medical neighborhood,” and the larger health system.1–5 Underlying these activities is a fundamental switch from a reactive care system oriented toward sickness (in which individual providers were paid for discrete elements of care) to a proactive care system oriented toward wellness, where teams and systems share accountability for the health of individual patients and populations.
How can internal medicine graduate medical education (GME) help meet this challenge? This article presents the evidence-based recommendations and opinions of selected leaders in general internal medicine based on iterative conversations before, during, and after the 2011 Society of General Internal Medicine (SGIM) Education Summit.
Recognizing that today's physician training programs may not adequately prepare physicians for tomorrow's models of health care delivery,6,7 there have been many calls over the past decade for medical education reform.8–14 As we consider the future of US health reform, it is clear we need to address at least 3 interdependent problems. We must (1) improve quality, (2) drive out waste, and (3) expand the notion of health care to include the social determinants of health that account for 70% of the burden of disease.15 These problems require us to reconsider the formation of tomorrow's workforce.
Our article focuses on the specific implications of US health reform for internal medicine GME. We describe the required competencies that will allow tomorrow's comprehensive primary care internist to thrive in a proactive US care system. We then propose 3 recommendations for reforming internal medicine GME training to foster that vision.
The SGIM Education Summit
In 2011, the Josiah Macy Jr Foundation and others sponsored and advised a SGIM Education Summit to address 2 questions: (1) What are the educational implications of current practice transformations to primary care home models? (2) What must we do differently to prepare internal medicine residents for their futures practicing in and leading patient-centered medical homes? The summit included 7 work groups,16 with each group having engaged in prework literature reviews and conference calls to generate preliminary recommendations. A single face-to-face meeting was convened where work groups' concepts and recommendations were shared, debated, and refined. This report is the result of deliberations among the policy work group members.
The Vision
The comprehensive primary care practice of the future should be the place where most patients can receive most of their care. For this to be true, tomorrow's primary care internists will need to specialize in managing comprehensive care, becoming effective members of patient-centered teams, and empowering community-oriented partnerships. What follows here is a brief summary of the essential competencies needed to perform each of these key roles.
Managing Comprehensive Care
For sake of brevity, we assume that readers are familiar with the Accreditation Council for Graduate Medical Education (ACGME) requirements for resident education in internal medicine.17 In addition to this vital foundation and the 6 ACGME competencies, we emphasize 2 additional competencies: comprehensive scope of care and longitudinal care planning.
Comprehensive primary care practices will need to expand their scope of care in the areas of advanced chronic disease, common outpatient procedures, and inpatient continuity of care. Two innovations will be important for managing advanced chronic disease: (1) patient registries, with responsibilities shared across the interprofessional primary care team,18,19 and (2) decision support by subspecialists, selected and incentivized to promote high-quality care in the comprehensive primary care practice.20
Tomorrow's comprehensive primary care internist, similar to current family practice physicians, will be able to competently perform common outpatient procedures needed by their patient population (eg, intrauterine device placement, colposcopy, suture of lacerations, incision and drainage of abscesses, joint injection). In some settings, comprehensive internists will provide integrated care by managing their patients in both the inpatient and outpatients arenas. The frequency of the need for the procedure or service, the individual's ability to develop competency in performing them, and ongoing quality monitoring should determine the scope of any physician's practice. At stake in each of these elements of expanded practice is the need to optimize continuity with a longitudinal care team.
Longitudinal planning refers to creating care plans congruent with patients' preferences and the time horizons for their conditions. For diagnoses of limited expected duration (eg, minor orthopedic injuries), care plans will be relatively short, ending when the episode of illness concludes. For chronic diagnoses expected to last a lifetime, care planning should encompass interventions to slow the progression of illness, reduce the severity and frequency of acute exacerbations, and when appropriate, facilitate end-of-life planning. During vulnerable transitions between care sites, longitudinal planning should begin with input from patients, their families, and their primary care team, and then optimize coordination between sending and receiving providers.
Becoming Effective Members of Patient-Centered Teams
In the area of effective team membership, 2 additional competencies are needed: team leadership and team “followership.” Team leadership requires skills in process improvement, workflow refinement, purposeful delegation, responding to performance metrics, and providing ongoing team member education and mentoring.21 Equally important is team followership and creating conditions that foster trust and enable others to act. At the heart of interprofessionalism is the recognition that multiple kinds of expertise (clinical, social, system, population, etc.) are needed to deliver comprehensive primary care.22,23 Tomorrow's internists must therefore practice participant leadership, inviting other team members to lead in turn, using their specific expertise to meet the patient or population needs at hand.
Empowering Community-Oriented Partnerships
Substantial evidence indicates that social determinants of health have a profound bearing on the public's health.15,24 Yet actions to modify those social determinants have traditionally fallen outside the purview of the health care sector. The comprehensive primary care internist of the future should actively seek out community partners and work to amplify their reach and impact. The physician's role is to adopt an open, community-oriented stance, foster trusting relationships with key community stakeholders, and then work with those stakeholders to identify priority social determinants and develop integrated clinical and community-based interventions to address them. This approach harkens back to the original US community health centers in Boston, Massachusetts, and Mound Bayou, Mississippi.25,26
The Way Forward for Internal Medicine GME
Assuming the development of payment models congruent with optimal primary care, what educational reforms are needed to prepare internal medicine graduates to thrive in the comprehensive primary care practices of the future?
We propose 3 reforms, discussed below and summarized in the table.
Table.
Recommendations for Internal Medicine Graduate Medical Education Reform
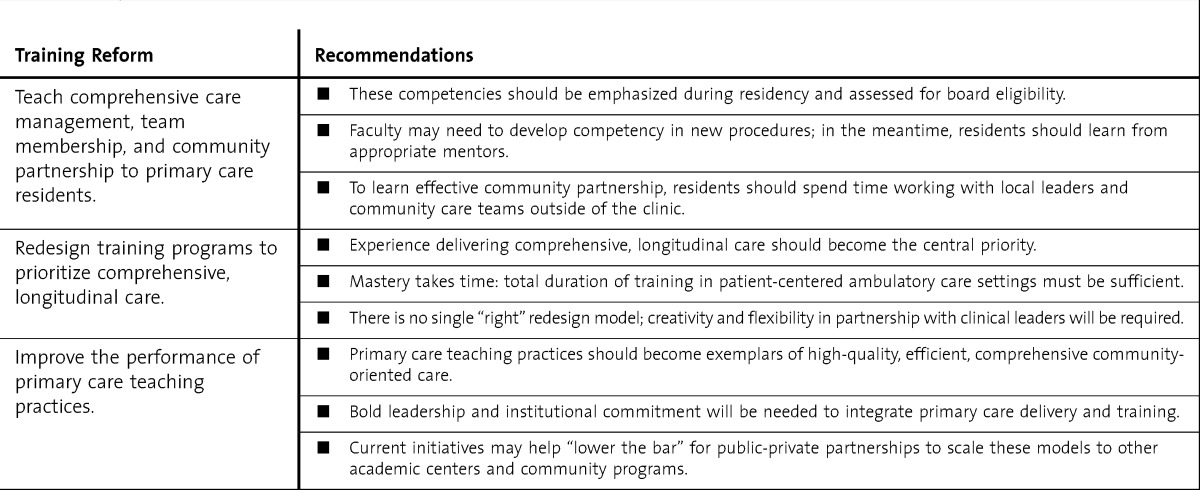
Training Reform 1: Teach Comprehensive Care Management, Team Membership, and Community Partnership to Primary Care Residents
Formal training in these areas should include classroom-based learning, project/goal-directed learning, and longitudinal reflective practice (ie, both “reflection-in-action,” which occurs in the workplace, and “reflection-on-action,” which occurs later).27 Assessment of developing competency in these areas should proceed throughout residency training. For residents to be capable of caring for most problems with which patient populations present, patient need, rather than traditional specialty boundaries, should drive the skills taught in residency. This will require that faculty develop competency in new procedures and, in the meantime, that residents learn these skills from the appropriate mentors.
We recommend that part of the evaluation for board eligibility include direct observation of performance in teams of various types (eg, multilevel inpatient teams, interprofessional medical home teams). We recognize that learning advanced teamwork and communication skills is a lifelong endeavor. The graduates' early years in practice should deliberately supplement residency learning in these domains.
Primary care residents should also spend time learning from, and working alongside, leaders in their local communities outside the confines of the clinic. Residents could, for example, be embedded in community care teams composed of social workers, behavioralists, dieticians, and home health nurses. Community dwell time may be needed if residents are to learn how to build durable and productive relationships with community partners.
Training Reform 2: Redesign Training Programs to Prioritize Comprehensive Longitudinal Care
Currently, most internal medicine training—even in primary care–oriented residencies—occurs in the hospital.17 As a result, graduates pursuing careers in primary care are underprepared for ambulatory practice.28 For training programs to produce graduates with the necessary skill sets, experience delivering comprehensive, longitudinal care must become the central priority.29
During the past few years, many internal medicine residency programs have implemented block-rotation approaches to meeting Residency Review Committee requirements for ambulatory training.30,31 Although current block models do provide an immersion experience for trainees, the program design remains fundamentally discontinuous. Little is known about the optimal duration of these ambulatory blocks as a strategy to inculcate the knowledge, skills, practices, and values needed for mastering competencies in managing comprehensive care, providing effective team membership, and empowering community-oriented partnerships. Mastery takes time. Total duration of training in patient-centered ambulatory care settings must be sufficient for residents to have a chance at becoming competent.
There is no single best way of restructuring residents' ambulatory experiences to ensure longitudinal and comprehensive training; creativity and flexibility in partnership with clinical leaders will be required. At the very least, residency programs must abolish the common practices of “flexing” clinic days and no-clinic rotations to accommodate inpatient service needs. Without predisposing any particular rotational design solution, residency programs must be held to a minimum patient-centered and learner-centered continuity requirement. This stability is a precondition for incorporating residents into longitudinal teams, which will be necessary for them to observe, learn, and practice effective teamwork.32
Training Reform 3: Improve the Performance of Primary Care Teaching Practices
Many primary care teaching practices do not exemplify the highest standards of comprehensive care management, patient-centered teamwork, or community partnerships to modify the social determinants of health. As a result, primary care residents are taught 1 thing and shown another. This is not only a setup for suboptimal learning but also a promotion of cynicism, burnout, and avoidance for a primary care career.33 Learning environments matter.34,35 We propose that primary care teaching practices should become focal points and exemplars of high-quality, efficient, comprehensive community-oriented care.
Teaching practices cannot achieve a transformation of this magnitude in isolation. Bold leadership and institutional commitment will be needed to integrate the primary care delivery mission with the education and training missions within academic centers. Clinical leaders must identify resources to catalyze necessary changes in personnel, work flows, space, and so on. Community training programs, by virtue of their smaller size and reduced “inertia,” may actually be better positioned to develop exemplary teaching practices. Learning collaboratives should be organized to share and build on lessons learned from their experiences.
Three relevant initiatives are underway. The Harvard Medical School Center for Primary Care has launched an Academic Innovations Collaborative to foster innovation in education and care delivery at 18 Harvard-affiliated primary care teaching practices. Students and residents work with practice leaders to improve performance in 4 areas: (1) team-based care, (2) management and prevention of chronic illness, (3) management of patients with multiple illnesses, and (4) patient empowerment and behavioral change.36 Meanwhile, the Kraft Center for Community Health (currently in Boston but with plans to expand to western Massachusetts in the coming year) has developed a 2-year fellow and practitioner program to foster hybrid leadership careers in community health. Kraft trainees practice primary care in a community health center, have protected time to participate in formal learning sessions and complete a mentored scholarly project, and receive loan repayment in exchange for a 2- to 3-year service obligation in a federally qualified health center.37 In addition, the Veterans Health Administration is funding 5 Centers of Excellence in Primary Care Education to redesign education and training for health professionals, including internal medicine residents, nurse practitioners, pharmacists, and psychologists, among others.38 Faculty, trainees, and clinical team members are collaborating to improve learning about and delivering patient-centered care in interprofessional, team-based, primary care practices. Experience from these initiatives may help lower the bar for public-private partnerships to replicate and scale these models to other academic medical centers and freestanding community training programs.
Conclusion
We envision comprehensive primary care practices of the future as the places where most patients can receive most of their care. If tomorrow's primary care internists are to thrive in such practices, their residency training will need to invest them with additional competencies in managing comprehensive care, becoming effective members of patient-centered teams, and empowering community-oriented partnerships. We propose 3 reforms for internal medicine GME: (1) teach comprehensive care management, team membership, and community partnership to primary care residents; (2) redesign training programs to prioritize comprehensive, longitudinal care; and (3) improve the performance of primary care teaching practices. We believe internal medicine GME has a vital role to play in US health reform: preparing future primary care internists to succeed in comprehensive primary care practice.
Footnotes
Patrick T. Lee, MD, is currently Medical Director of the Primary Care Center at Cambridge Health Alliance, Director of Education at the Kraft Center for Community Health, and Instructor in Medicine at Harvard Medical School, and he was Director, Global Primary Care Program at Massachusetts General Hospital at the time of writing; Mark W. Friedberg, MD, MPP, is Natural Scientist at RAND Corporation and Clinical Instructor in Medicine, Harvard Medical School and Division of General Internal Medicine, Brigham and Women's Hospital; Judith L. Bowen, MD, is Professor of Medicine at Oregon Health & Science University and Education Consultant for the Veterans Health Administration Office of Academic Affiliations; Susan C. Day, MD, MPH, is Director of Ambulatory Quality and Practice Improvement and Professor of Medicine at the University of Pennsylvania; Charles M. Kilo, MD, MPH, is Chief Medical Officer at Oregon Health & Science University; Christine A. Sinsky, MD, FACP, is Internal Medicine Physician at the Medical Associates Clinic.
All authors participated in the Society of General Internal Medicine (SGIM) Education Summit, and are grateful to the following funders, advisory board organizations, and external advisors for their sponsorship and contributions to the 2011 SGIM Education Summit.
Funding: Josiah Macy Jr Foundation supported the Education Summit. Additional financial support for the Summit was provided by the United Health Foundation. The American College of Physicians, Primary Care Progress, and the Veterans Health Administration office of Academic Affiliations provided in-kind support.
Advisory board organizations: The American Board of Internal Medicine, the American College of Physicians, the Association of Program Directors in Internal Medicine, the Clerkship Directors in Internal Medicine, and the Society of General Internal Medicine. External advisors: The Bureau of Health Professions/Health Resources and Services Administration, the Macy Foundation, the National Initiative for Children's Healthcare Quality, Primary Care Progress, the Robert Wood Johnson Foundation, and the Veterans Health Administration Office of Academic Affiliations.
References
- 1.Fisher ES. Building a medical neighborhood for the medical home. N Engl J Med. 2008;359(12):1202–1205. doi: 10.1056/NEJMp0806233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sinsky CA. The patient-centered medical home neighbor: a primary care physician's view. Ann Intern Med. 2011;154(1):61–62. doi: 10.7326/0003-4819-154-1-201101040-00010. [DOI] [PubMed] [Google Scholar]
- 3.American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, American Osteopathic Association. 2007. Joint Principles of the Patient-Centered Medical Home. http://www.pcpcc.net/joint-principles. Accessed April 1, 2013. [Google Scholar]
- 4.Alexander GC, Kurlander J, Wynia MK. Physicians in retainer (“concierge”) practice: a national survey of physician, patient, and practice characteristics. J Gen Intern Med. 2005;20(12):1079–1083. doi: 10.1111/j.1525-1497.2005.0233.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wasson JH, Anders SG, Moore LG, Ho L, Nelson EC, Godfrey MM, et al. Clinical microsystems, part 2: learning from micro practices about providing patients the care they want and need. Jt Comm J Qual Patient Saf. 2008;34(8):445–452. doi: 10.1016/s1553-7250(08)34055-0. [DOI] [PubMed] [Google Scholar]
- 6.Blank L, Kimball H, McDonald W, Merino J ABIM Foundation, ACP Foundation, European Federation of Internal Medicine. Medical professionalism in the new millennium: a physician charter 15 months later. Ann Intern Med. 2003;138(10):839–841. doi: 10.7326/0003-4819-138-10-200305200-00012. [DOI] [PubMed] [Google Scholar]
- 7.Institute of Medicine. Health Professions Education: A Bridge to Quality. Washington, DC: National Academies Press; 2003. [PubMed] [Google Scholar]
- 8.Holmboe ES, Bowen JL, Green M, Gregg J, DiFrancesco L, Reynolds E, et al. Reforming internal medicine residency training: a report from the Society of General Internal Medicine's task force for residency reform. J Gen Intern Med. 2005;20(12):1165–1172. doi: 10.1111/j.1525-1497.2005.0249.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Weinberger SE, Smith LG, Collier VU Education Committee of the American College of Physicians. Redesigning training for internal medicine. Ann Intern Med. 2006;144(12):927–932. doi: 10.7326/0003-4819-144-12-200606200-00124. [DOI] [PubMed] [Google Scholar]
- 10.Larson EB, Fihn SD, Kirk LM, Levinson W, Loge RV, Reynolds E, et al. The future of general internal medicine: report and recommendations from the Society of General Internal Medicine (SGIM) Task Force on the Domain of General Internal Medicine. J Gen Intern Med. 2004;19(1):69–77. doi: 10.1111/j.1525-1497.2004.31337.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Association of Program Directors in Internal Medicine. Fitzgibbons JP, Bordley DR, Berkowitz LR, Miller BW, Henderson MC. Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine. Ann Intern Med. 2006;144(12):920–926. doi: 10.7326/0003-4819-144-12-200606200-00010. [DOI] [PubMed] [Google Scholar]
- 12.Charap MH, Levin RI, Pearlman RE, Blaser MJ. Internal medicine residency training in the 21st century: aligning requirements with professional needs. Am J Med. 2005;118(9):1042–1046. doi: 10.1016/j.amjmed.2005.06.009. [DOI] [PubMed] [Google Scholar]
- 13.Arora V, Guardiano S, Donaldson D, Storch I, Hemstreet P. Closing the gap between internal medicine training and practice: recommendations from recent graduates. Am J Med. 2005;118(6):680–685; discussion 685–687. doi: 10.1016/j.amjmed.2005.03.022. [DOI] [PubMed] [Google Scholar]
- 14.Cooke M, Irby DM, O'Brien BC. Educating Physicians: A Call for Reform of Medical School and Residency. San Francisco, CA: Jossey-Bass; 2010. [Google Scholar]
- 15.World Health Organization Commission on Social Determinants of Health. Closing the gap in a generation: health equity through action on the social determinants of health. Geneva: WHO Press; 2008. [DOI] [PubMed] [Google Scholar]
- 16.Chang A, Bowen JL, Buranosky RA, Frankel RM, Ghosh N, Rosenblum MJ, et al. Transforming primary care training-patient-centered medical home entrustable professional activities for internal medicine residents [published online ahead of print September 21, 2012] J Gen Intern Med. doi: 10.1007/s11606-012-2193-3. doi:10.1007/s11606-012-2193-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Graduate Medical Education in Internal Medicine. 2009. https://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/140_internal_medicine_07012009.pdf. Accessed February 4, 2013. [Google Scholar]
- 18.Campion FX, Tully GL, Barrett JA, Andre P, Sweeney A. Improving quality of care using a diabetes registry and disease management services in an integrated delivery network. Dis Manag. 2005;8(4):245–252. doi: 10.1089/dis.2005.8.245. [DOI] [PubMed] [Google Scholar]
- 19.Helfrich CD, Savitz LA, Swiger KD, Weiner BJ. Adoption and implementation of mandated diabetes registries by community health centers. Am J Prev Med. 2007;33(1)(suppl):S50–S58; quiz S59–S65. doi: 10.1016/j.amepre.2007.04.002. [DOI] [PubMed] [Google Scholar]
- 20.Arora S, Thornton K, Murata G, Deming P, Kalishman S, Dion D, et al. Outcomes of treatment for hepatitis C virus infection by primary care providers. N Engl J Med. 2011;364(23):2199–2207. doi: 10.1056/NEJMoa1009370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.DeChurch LA, Mesmer-Magnus JR. The cognitive underpinnings of effective teamwork: a meta-analysis. J Appl Psychol. 2010;95(1):32–53. doi: 10.1037/a0017328. [DOI] [PubMed] [Google Scholar]
- 22.Coleman MT, Roberts K, Wulff D, van Zyl R, Newton K. Interprofessional ambulatory primary care practice-based educational program. J Interprof Care. 2008;22(1):69–84. doi: 10.1080/13561820701714763. [DOI] [PubMed] [Google Scholar]
- 23.Leasure E, Jones R, Meade R, Sanger MI, Thomas KG, Tilden VP, et al. There is no “I” in teamwork in the patient centered medical home: defining teamwork competencies for academic practice. Acad Med. In press doi: 10.1097/ACM.0b013e31828b0289. [DOI] [PubMed] [Google Scholar]
- 24.Marmot M, Atkinson T, Bell J, Black C, Broadfoot P, Cumberlege J, et al. Fair Society, Healthy Lives: Strategic Review of Health Inequalities in England post-2010. UCL London: Institute of Health Equity, The Marmot Review; 2010. [Google Scholar]
- 25.Geiger HJ. Community-oriented primary care: a path to community development. Am J Public Health. 2002;92(11):1713–1716. doi: 10.2105/ajph.92.11.1713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Geiger HJ. The first community health centers: a model of enduring value. J Ambul Care Manage. 2005;28(4):313–320. doi: 10.1097/00004479-200510000-00006. [DOI] [PubMed] [Google Scholar]
- 27.Branch WT, Jr, Paranjape A. Feedback and reflection: teaching methods for clinical settings. Acad Med. 2002;77(12, pt 1):1185–1188. doi: 10.1097/00001888-200212000-00005. [DOI] [PubMed] [Google Scholar]
- 28.Bowen JL, Salerno SM, Chamberlain JK, Eckstrom E, Chen HL, Brandenburg S. Changing habits of practice. Transforming internal medicine residency education in ambulatory settings. J Gen Intern Med. 2005;20(12):1181–1187. doi: 10.1111/j.1525-1497.2005.0248.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hirsh DA, Ogur B, Thibault GE, Cox M. “Continuity” as an organizing principle for clinical education reform. N Engl J Med. 2007;356(8):858–866. doi: 10.1056/NEJMsb061660. [DOI] [PubMed] [Google Scholar]
- 30.Warm EJ. Interval examination: the ambulatory long block. J Gen Intern Med. 2010;25(7):750–752. doi: 10.1007/s11606-010-1362-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Warm EJ, Schauer DP, Diers T, Mathis BR, Neirouz Y, Boex JR, et al. The ambulatory long-block: an Accreditation Council for Graduate Medical Education (ACGME) educational innovations project (EIP) J Gen Intern Med. 2008;23(7):921–926. doi: 10.1007/s11606-008-0588-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Salas E, DiazGranados D, Klein C, Burke CS, Stagl KC, Goodwin GF, et al. Does team training improve team performance? a meta-analysis. Hum Factors. 2008;50(6):903–933. doi: 10.1518/001872008X375009. [DOI] [PubMed] [Google Scholar]
- 33.Dowdy DW. Trained to avoid primary care. Ann Intern Med. 2011;154(11):776–777. doi: 10.7326/0003-4819-154-11-201106070-00012. [DOI] [PubMed] [Google Scholar]
- 34.Haidet P, Kelly PA, Bentley S, Blatt B, Chou CL, Fortin AHVI, et al. Not the same everywhere: patient-centered learning environments at nine medical schools. J Gen Intern Med. 2006;21(5):405–409. doi: 10.1111/j.1525-1497.2006.00417.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Dornan T, Boshuizen H, King N, Scherpbier A. Experience-based learning: a model linking the processes and outcomes of medical students' workplace learning. Med Educ. 2007;41(1):84–91. doi: 10.1111/j.1365-2929.2006.02652.x. [DOI] [PubMed] [Google Scholar]
- 36.Center for Primary Care, Harvard Medical School. Center's Academic Innovations Collaborative. https://primarycare.hms.harvard.edu/what-we-do/program-primary-care-innovation/academic-innovations-collaborative. Accessed December 20, 2012. [Google Scholar]
- 37.The Kraft Center for Community Health. Community Health Centers. http://www.kraftcommunityhealth.org/Participate/Community-Health-Centers/Default.aspx. Accessed December 20, 2012. [Google Scholar]
- 38.US Dept of Veterans Affairs. VA Centers of Excellence in Primary Care Education. http://www.va.gov/oaa/rfp_coe.asp. Accessed December 20, 2012. [Google Scholar]