
Figure 4.
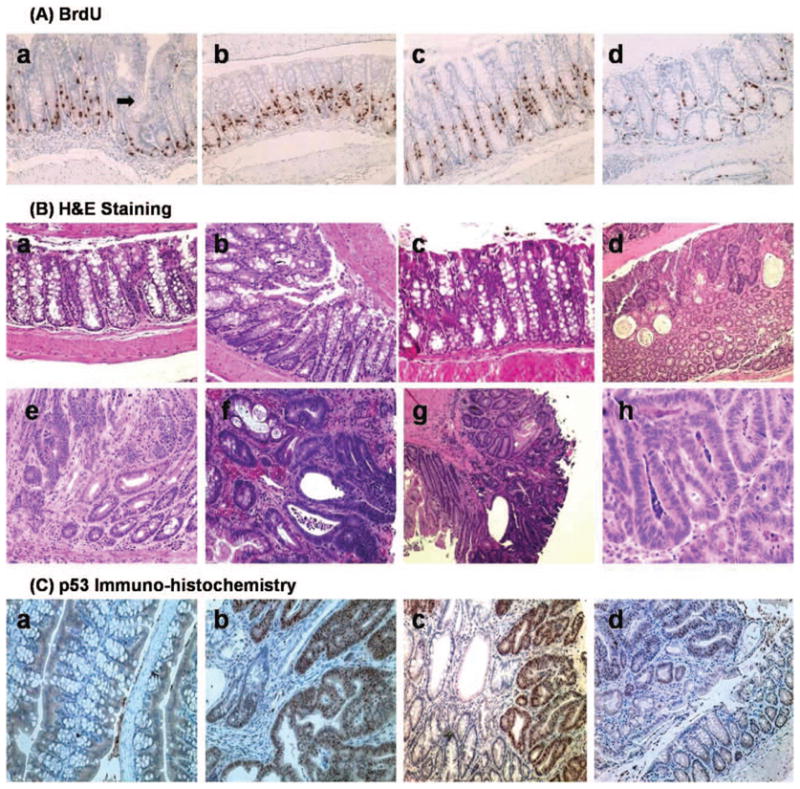
(A) Immunohistochemical staining of BrdU labeling (200×) shown in representative groups (a) hGAS colon. Arrow demonstrates an area of crypt fission, which may eventually transform into adenoma, (b) hGAS/p53RH crypt also demonstrating a high degree of BrdU labeling, (c) p53RH colon, and (d) Wild type C57BL6 colon showing a relatively lower LI and crypt depth. (B) Hematoxylin and eosin staining shows the differences in histopathology across the four study groups. (a) Normal area of colon showing uninvolved crypts in a WT untreated mouse (100×). (b) HE staining of an hGAS mouse distal colon (age approx. 10 weeks) showing aberrant crypt foci (ACF) and increased crypt depth (200×). (c) Hypertrophic crypts in the double mutant hGAS/p53RH animal that was not treated with AOM (control) at thirty weeks of age. (d) Note the large vacuolization and increased cellular debris, a characteristic finding secondary to rapid cell turnover in colonic adenocarcinoma. (e) Is an adenoma (200×) developing in a WT mice that was AOM treated. Noteworthy is the loss of crypt architecture and increase in immature crypts with increase in stromal matrix. (f) Shows an advanced moderately differentiated tumor in an hGAS mouse (400×). (g) Represents a moderately differentiated adenocarcinoma (100×) that is invading the serosa in an AOM treated double mutant mouse. (h) Tubular adenoma in a p53RH mutant mouse at 200× magnification respectively. (C) p53 immunohistochemistry done on representative sections in all the four study groups: (a) Wild type colon showing no cellular localization of p53 protein. Intranuclear accumulation of p53 protein is clearly visualized in Figures(b) and (c) respectively, magnified to 200× here. The tumors in the hGAS/p53RH colon in (b) and p53RH colon in (c) have the accumulation of intranuclear p53 protein. In Figure(c) areas of normal colon are also visible (lightly stained) but the areas showing the abnormal crypts (tumor) contain dark brown stained nuclei, which suggest p53 protein. (d) Colonic adenoma in an hGAS mouse with no immunohistochemical evidence of p53 accumulation.